
Abstract

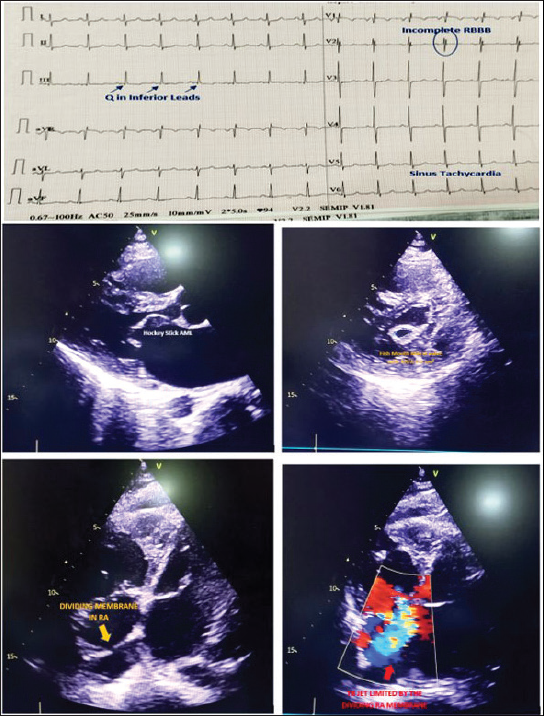
We present a case of 22-year-young male with bilateral tibia fracture since last 20 days presenting in emergency medicine with acute onset shortness of breath since last 2 days. On clinical examination, he had blood pressure of 100/60 mm Hg in right arm supine position with resting heart rate of 100 beats per min and SpO2 of 88% in room air. Electrocardiogram (EKG) revealed incomplete right bundle branch block and the emergency resident rushed for a computed tomography (CT) pulmonary angiogram to rule out acute pulmonary embolism without any delay. Strikingly, CT pulmonary angiogram revealed cardiomegaly with dilated main pulmonary artery suggestive of pulmonary arterial hypertension and suffused pulmonary hilum with bilateral interlobular septal thickening and bilateral minimal pleural effusion. CT could not rule out bilateral micro-fat embolism. NT-proBNP was raised in thousands and D-Dimer was also raised. After the resident returned, bedside cardiology consultation was asked. On auscultation, the patient had cardiomegaly with right ventricular apex with loud S1, long midiastolic rumble at apex, loud P2 with narrow split, and pansystolic murmur of tricuspid regurgitation with presence of Caravallo sign. Chest X-ray revealed mitralization of the left border of heart. Echocardiography revealed the uncommon presence of cor triatriatum dexter where right atrium was divided into 2 chambers by a thin flap of membrane without any obstruction, and the forward motion of the jet of severe tricuspid regurgitation was limited by the dividing flap present in the right atrium (Figure 1). Patient had also severe rheumatic mitral stenosis (mitral valve area [MVA] 0.6 cm2 with mean diastolic gradient [MDG] 29/15 mm Hg) with severe tricuspid valve regurgitation and severe passive pulmonary arterial hypertension (right ventricular systolic pressure [RVSP]: 102 mm Hg estimate from TR jet). Patient was kept on oxygen therapy, betablocker, and high-dose diuretic therapy after which he was stable. Although balloon dilatation of the dividing right atrial membrane could be done along with PBMV, we advised the patient to undergo complete surgical repair, that is, mechanical mitral valve replacement with tricuspid valve repair due to presence of severe organic tricuspid regurgitation along with excision of the dividing right atrial membrane. Our case is a rare illustration of the presence of cor triatriatum dexter in a case of rheumatic mitral stenosis 1 which masqueraded as acute pulmonary embolism in a young. Even the emergency room resident should auscultate the precordium in a patient presenting with acute breathlessness before shifting for CT pulmonary angiogram. Clinical examination always supersedes the clinical suspicion.
Cor Triatriatum Dexter With Severe Rheumatic Mitral Stenosis Masquerading as Acute Pulmonary Embolism in a Young.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Institutional Ethical Committee (IEC) clearance has been obtained.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed Patient Consent has been obtained.