
Abstract
It is becoming increasingly apparent that although anxiety and depression are separate concerns, there is considerable overlap of clinical symptoms and pathophysiological processes. Research shows that comorbidities, anxiety, and depression are most common than either disorder alone. Coronary heart disease and mental illness are among the leading causes of morbidity and mortality worldwide. Cardiac surgery places extensive stress on spouses who often are more worried than the patients themselves. Spouses can experience challenging and demanding situations when their partner becomes critically ill.
In the present research, spouses showed normal anxiety levels, but when assessed separately, women’s anxiety scores were significantly higher compared to men. There was no significant difference between male and female spouses’ depression scores. Correlation analysis showed a positive relationship between anxiety and depression scores explaining that with rise in anxiety scores, there was an increase in depression scores in female spouses. Spouses who were unemployed felt overwhelmed with not being financially competent to manage expenses incurred for surgery and pre- and postoperative care. Lastly, a lack of social support led to anxiety in nuclear families.
Introduction
CHD, also known as ischemic heart disease or coronary artery disease, is a common term for the build-up of a waxy substance, called plaque, in the heart’s arteries, leading to the failure of coronary circulation to supply adequate blood circulation to cardiac muscle and surrounding tissue—a phenomenon that can result in myocardial infarction. 1
The main risk factors for CHD include dyslipidemia, diabetes, arterial hypertension, obesity, smoking, and a sedentary lifestyle, as well as stress, older age, male gender, and a family history of CHD. 2
Although there is bidirectional association between mental and physical illness, an association between depression and CHD is now well established.3,4
Spousal Experiences During Cardiac Operations
Heart disease may lead to patients’ physical and emotional distress, job loss, disability, and reduced quality of life. 5 While empirical research suggests that coronary artery bypass graft (CABG) surgery is stressful for the patient, 6 the patient’s spouse may be under more stress than the patient. 7
The spouse may demonstrate poorer psychological adjustment and higher levels of anxiety and depression than the patient, both immediately and following acute cardiac events, such as acute myocardial infarction (AMI), heart failure, 8 CABG surgery, 5 as well as during the first 3 months after hospital discharge.9,10
During and after acute cardiac interventions, spouses complain of neglect in an environment devoted to the patient. 11 Spouses may also be more immediately concerned about the changing marital roles, as the burden of care giving and other responsibilities falls on their shoulders. 12
Anxiety
Anxiety is something we hear in our everyday conversations. Due to distinct reasons, there is a significant increase in anxious thoughts in all age groups. Anxiety is a feeling of feeling overwhelmed due to fear or dread which causes uneasiness resulting in physiological symptoms of restlessness.
Depression
Depression on the other hand negatively affects our cognition and processing of information. There is a marked sense of sadness accompanied by self-worthlessness and if not checked in time can lead to suicidal ideations. During a depressive episode, the person experiences depressed mood (feeling sad, irritable, empty) or a loss of pleasure or interest in activities for at least 2 weeks.
Anxiety From Depression—Overlap in Diagnosis
Generalized anxiety disorder is strongly comorbid with, and commonly precedes, major depression. While on one hand depression causes feelings of sadness, hopelessness, and reduced energy. On the other hand, anxiety creates feelings of nervousness, worry, or dread. Although the two conditions are different, patients can have both at the same time. Overlapping symptoms between the two can be seen in a person’s agitation and restlessness.
Disturbances in serotonin and norepinephrine neurotransmitters result in both anxiety and depression. 13 It has been noted that a major depressive disorder after the onset of an anxiety disorder is frequently diagnosed in clinical setups like outpatient department as well in patients undergoing treatments for an ongoing illness. 14
With respect to major depression, a worldwide survey reported that 45.7% of individuals with lifetime major depressive disorder had a lifetime history of one or more anxiety disorder as studied by Kessler et al. 15
From the point of inheritance, anxiety and depressive disorders are moderately heritable (approximately 40%), and evidence suggests shared genetic risk across these internalizing disorders. Among internalizing disorders, the highest level of shared genetic risk is between major depressive disorder and generalized anxiety disorder. 16
Cognitive Correlates of Anxiety and Depression: Helplessness Model
Evidence-based research shows how anxiety and depression are moderately correlated with each other. This concurrence is associated with emotional states of negative affect, stressful life events, impaired cognitive processes, and that they share a common biological/genetic predisposition. 17
Aim of This Study
Any patient undergoing either an investigation or a surgical intervention needs social support and that is where spousal support becomes most dominant. It is evident from visits to the hospital to pre- and postoperative care. This study aims to highlight the mental well-being of spouses before CABG intervention. As surgical procedures can be unexpected and tense for the patient and their families, a need to discuss spouse’s state of mind was considered crucial from therapy point of view.
Hypotheses
H1: There will be significant differences in the anxiety scores of spouses.
H2: There will be significant differences in the depression scores of spouses.
H3: There will be correlation between depression and anxiety scores of spouses.
H4: Age will have noteworthy influence on anxiety and depression scores in spouses.
H5: Occupation will influence anxiety and depression scores in spouses.
H6: Family type will affect levels of anxiety and depression in spouses.
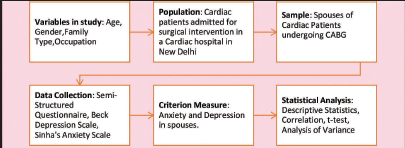
Research Design
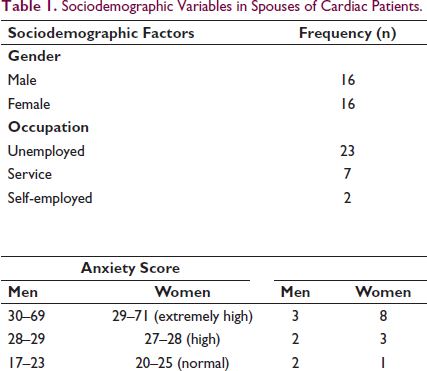
A research design was created with socioeconomic variables that can influence levels of anxiety and depression scores in the sample prior to their spouse’s surgery (Table 1).
Sociodemographic Variables in Spouses of Cardiac Patients.
Procedure
Researcher met patients and their families daily to discuss their concerns regarding surgery and if possible, addressed their psychological needs. Consent forms were signed after discussing rationale for this research. Results were shared with spouses separately and if needed, counseling was offered as a therapeutic modality for calming concerns before their spouse’s surgery.
Tools Used
Unstructured Questionnaire to gather sociodemographic information from participants
Beck Depression Inventory (BDI) by Aaron T Beck is a 21-question multiple-choice self-report inventory, one of the most widely used psychometric tests for measuring the severity of depression. This test reports correlation coefficient of 0.86 for the test items, and the Spearman-Brown correlation for the reliability of 0.93. Test-retest reliability ranged from 0.48 to 0.86 in give studies of psychiatric patients and 0.60 to 0.83 in 6 nonpsychiatric populations. 18
Sinha’s Comprehensive Anxiety Test (SCAT) consists of 90 items, significant at 0.01 levels. Higher the scores show higher the anxiety. The coefficient of reliability determined by using the product-moment correlation was 0.85 and by using Spearman was 0.92. The coefficient of validity was 0.62, which is significant beyond 0.01 level of confidence.
Scoring
BDI—Less than 10 explains no or minimal depression, 10 to 18 ranges in mild-to-moderate depression, 19 to 29 diagnosed as moderate-to-severe depression, and 30 and above as severe depression.
Sinha Comprehensive Anxiety Scale: The maximum possible score of this test is 90 and minimum scores is zero. Each item scored 1 for positive response and zero for negative response. The sum of all positive or yes responses would be the total anxiety score of the individual.
Results
Our sample had equal number of male and female spouses (n = 16) who came from nuclear and joint family setups (n = 16). In our sample, spouses were unemployed (n = 23, 73%), that is, either stay-at-home spouses or retired employees and in the age range of 60 to 70 years (n = 11, 34%) respectively.
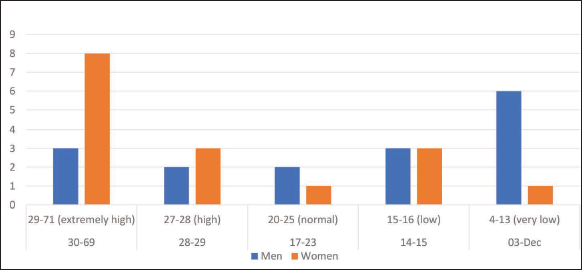
In our sample, we observed that on anxiety scores, most men showed low anxiety (n = 6, 38%) whereas women showed high anxiety (n =8, 50%). Spouses showed a mean anxiety score of (22.5), which is in the normal range for both male and female spouses. But when assessed separately, women anxiety scores were significantly higher as compared to men (t = 2.41* P value = .02). Thus, we can say that in the present study, we accept Hypothesis 1 that states that there will be significant differences in the anxiety scores of spouses.
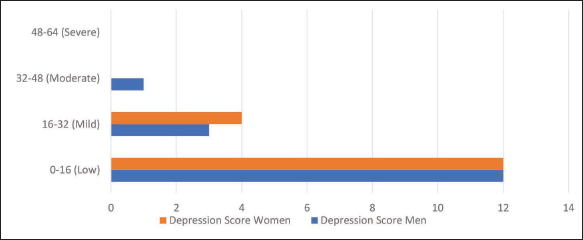
Regarding scores on depression, both male and female spouses showed insignificant/no depression in the present study as mean depression score in the sample was 11.5 (ranged from mild-to-moderate range). Thus, we can say that in the present study, we reject Hypothesis 2 that states that there will be significant differences in the depression scores of spouses as shown in Table 2.
Statistical Analysis of the Sample.
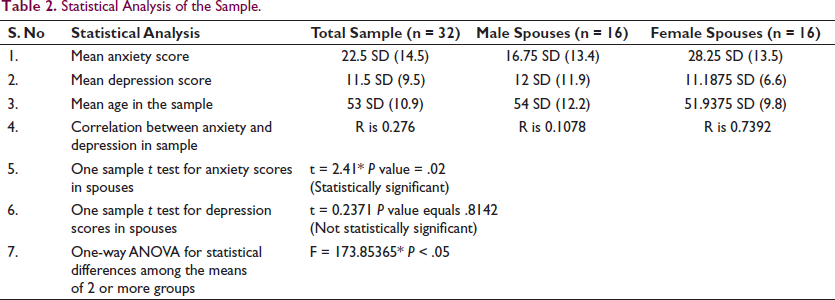
While analyzing correlation between anxiety and depression scores, we noticed a weak but a positive correlation in the sample. This explains that with the rise in anxiety scores, there was an increase in depression scores in spouses, especially in women. Thus, we accept Hypothesis 3 that states that there will be correlation between depression and anxiety scores of spouses.
Sociodemographic variables like age, family type, and occupation were analyzed with anxiety and depression scores using one-way ANOVA and results showed significant statistical relationship in socio-demographic variables and sample scores.
Analysis of mean scores of all variables in the study explains significant difference in the age of the spouses and their occupation. This explains that higher the age, lesser their occupational involvement.
Age also showed significant differences in family type which showed elderly spouses in nuclear family setup were looking after their spouses for cardiac treatment. With age we also noticed a mean anxiety score of 22.5 (normal levels). This explains that with age comes wisdom to control anxious thoughts and to deal with situation assertively, as spouses support patients during vulnerable moments before heart surgery as shown in Table 3.
Post-Hoc Tukey HSD on Variables in the Study.
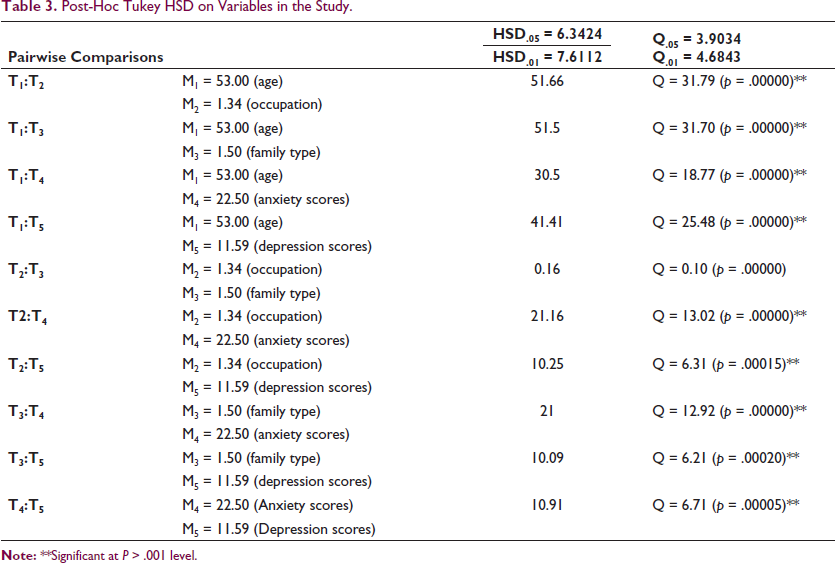
Hence, in the present study we accept Hypothesis 4 that states that age will have significant influence on anxiety and depression scores in spouses.
Spouses who were unemployed (stay-at-home spouses or retired) felt overwhelmed with not being financially competent to manage expenses incurred for surgery and pre- and postoperative care. Analysis helped us to accept Hypothesis 5 which states that occupation will influence anxiety and depression scores in spouses.
Lastly, spouses coming from joint families had normal range of anxieties which could be due to uncertainties before spouse’s surgery and postop recovery. Lack of social support was one aspect leading to anxiety due to nuclear setup. Also, as there were few people to interact or share concerns, spouses of cardiac patients shared depressive thoughts. Thus, in the present research, we accept Hypothesis 6 which states that family type will affect levels of anxiety and depression in spouses.
Discussion
This study was conducted to evaluate anxiety and depression for spouses whose partners were undergoing CABG procedure. Our participants discussed how swiftly they had to share family burden along with increased parental and household responsibilities. Also, they discussed how often they struggled to balance their needs with those of other family members and do not feel longing and intimacy with their partners. These experiences were of loss of emotional, social, and economic support from their spouses as well as altered plans for shared future.
Present study showed significant research findings as follows:
Female partners (wives) showed significantly higher anxiety scores as compared to male partners (husbands) which is congruent with past research findings that state that stress was more strongly related to symptoms in women, suggesting that they may have a greater susceptibility to surrounding stress, and to somatic illness stress (Figure 1). This might contribute to the sex difference in psychiatric illness. 19
With the rise in anxiety scores, there was an increase in depression scores in spouses, especially in women (Figure 2). These findings comply with past research which explain anxiety and depressive disorders being more prevalent in women, with an approximate 2:1 ratio in women compared with men during women’s reproductive years. 20
With age comes wisdom to control anxious thoughts and to deal with situation assertively, as spouses support patients during vulnerable moments before heart surgery. These findings are compatible with past research where older spouses were more in control as the surgical event may have been expected and therefore less anxiety producing. Also, most younger spouses had dependents at home, and therefore reasonable that the stress of major heart surgery would be greater for a 40-year-old than for a 79-year-old. 21
Spouses who were unemployed (stay-at-home spouses or retired) felt overwhelmed with not being financially competent to manage expenses incurred for surgery and pre- and postoperative care. These findings comply with some studies that indicate that women are more sensitive than men to the events happening to their spouses22,23 and are thus more vulnerable to emotional transmission. 24
Lack of social support was one aspect leading to anxiety due to nuclear setup. Also, as there were few people to interact or share concerns, spouses of cardiac patients shared depressive thoughts.
These findings are in line with past research which suggests that there is a positive relationship between loneliness and depression and anxiety. 25
Spouses often experience greater anxiety and depression and less perceived control than patients themselves. Attention to the psychological distress experienced by spouses of patients who have suffered a cardiac event may improve outcomes in patients. 7
Anxiety scores in Spouses.
Depression scores in Spouses.
Studies demonstrated that spouses who have a key role in caregiving of their husbands or wives who are suffering from CAD are at increased risk of developing psychological problems such as anxiety, depression, and increased stress level.7,26 This could cause a vicious cycle as patients have more difficulty to deal with their own psychosocial problems when their spouses are more anxious, depressed, or stressful, 27 where wife’s feeling of vulnerability resulted from dependency on others’ status and basic needs. For men it would be feeling at loss to express themselves openly specially with grief and requiring assistance with daily life especially if there are children. Patients who are supported by their family members, especially their spouses, recover faster than those who do not have such support. 28
Conclusion
Patients and their spouses experience difficulties like dealing with physiological symptoms, role changes in the family, frequent hospitalization, forced retirement, financial stress, and reduction in social support leading to disharmony in the couple system. This study kept in mind spouses’ mental well-being who are primary caretakes to the patients lined up for bypass grafting. Results showed that female spouses showed more anxiety than male spouses and there was a strong correlation between their anxiety and depression scores. Older spouses showed anxiety due to nuclear setup and lack of social support. Lack of occupation was seen as an antecedent to anxious symptoms in spouses due to financial burden for partner’s treatment.
Footnotes
Limitations
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.