
Abstract

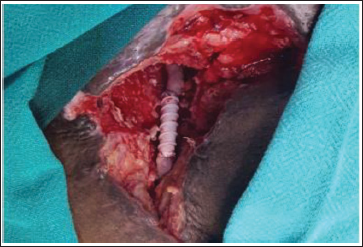
Fifty-four-year-old male patient with diabetes mellitus and hypertension presented with right lower abdominal pain and right lower limb swelling for a six-month duration in November 2021. On clinical examination, there was a hard-fixed mass measuring 8 × 10 cm in the right iliac fossa extending to till right inguinal crease, with right lower limb pitting edema. Contrast CT of the abdomen and pelvis showed a retroperitoneal tumor measuring 14 × 11 × 9 cm, encasing the external iliac vessels for a length of 6 cm. Fat plane with right psoas muscle was lost. The middle third of the ureter, distal 2 cm of common iliac artery and the internal iliac artery was draping over the mass. A venous doppler study of the right lower limb showed no evidence of deep vein thrombosis. Image-guided core needle biopsy from the lesion showed a malignant spindle cell neoplasm suggestive of leiomyosarcoma (Desmin and SMA positive, CD34, CD117 and S-100 Negative). The case was discussed in a multidisciplinary board meeting and was planned for neoadjuvant radiotherapy. He received 50.4 Gy of radiation in 28 fractions from 23rd December 2021 to 30th January 2022. Post-neoadjuvant radiation response assessment showed stable disease. We could not proceed with resection with vascular reconstruction in view of the covid pandemic. Hence, he was planned for neoadjuvant chemotherapy as per the multidisciplinary board meeting. Accordingly, he received three cycles of systemic therapy (Adriamycin and Ifosfamide). The disease was stable after neoadjuvant chemotherapy. He had undergone resection of a retroperitoneal tumor on 6th July 2022. Intraoperatively we noticed extensive adhesion of the sigmoid and its mesocolon to the urinary bladder and pelvic peritoneum (RT-induced). A retroperitoneal mass of 12 × 9 cm was arising from the right psoas muscle, encasing the right external iliac artery and vein (including deep inferior epigastric vessels) with the distal part of common iliac vessels (3 cm), and internal iliac vessels closely abutting the tumor. The middle third of the right ureter (6 cm) was draped over the posteromedial surface of the tumor. Mass was extending superiorly till aortic bifurcation and inferiorly till inguinal ligament. Posterolateral tumor was closely abutting the lateral pelvic wall and obturator nerve. Right gonadal vessels were draped over tumor. The right internal iliac vein and artery, right gonadal vessels, and right vas deferens were sacrificed during extensive resection. Right ureter, obturator nerve, and lumbosacral root were preserved. As R0 resection was not possible in view of the involvement of S2 neural foramina, the tumor was divided and external iliac vessels were dissected of the tumor. Postoperatively patient had developed a surgical site infection with dehiscence of the rectus sheath, managed by re-suturing the rectus sheath and wound dressings. He was discharged on the 18th postoperative day with instructions for daily wound care. The final histopathology report was pleomorphic leiomyosarcoma measuring 12 × 10 × 8 cm. On his 40th postoperative day during high-dose postoperative radiotherapy, he presented to the emergency department with a history of sudden onset of active bleeding from a lower abdominal wound. After initial resuscitation patient was shifted to the operating room for exploration. On exploration found to have 1 × 1 cm defect on the anterior wall of the external iliac artery 6 cm proximal to the origin of the deep femoral artery. The vessel wall 1 cm distal and proximal to the defect was unhealthy. Hence unhealthy segment of the external iliac artery was resected (5 cm) and reconstructed with a ringed PTFE graft (Figure 1) (end-to-end anastomosis with 5.0 polypropylene). On follow-up with NOAC after one month and three months, the right external iliac artery was flowing well in doppler with no evidence of thrombus inside without any limb ischemia. Our case is an extremely rare illustration of radiotherapy-induced perforation of external iliac artery 1 which was successfully reconstructed with a ringed PTFE graft. From 1961 to 1981 at the University of Kentucky Medical Center, there were 20 patients with the radiation-induced vascular injury which included 11 carotid blue outs and one iliac artery rupture. 2 In those eras vascular surgery was not so developed, and ligation of the iliac artery led to severe ischemia requiring hip disarticulation. Three patients had radiation-induced carotid stenosis and three patients had radiation-induced focal stenosis of the iliofemoral artery which were successfully treated with bypass grafting. Radiation-induced arteriopathy involves carotid, subclavian, coronary and femoral. Operative repair with polytetrafluoroethylene and saphenous vein graft is successful in those radiation-induced arteriopathies. 3
Ringed PTFE Graft over Ruptured Right External Iliac Artery.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Ethical Committee (IEC) approval has been obtained.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Informed patient consent has been obtained.