
Abstract
A 60-year-old male with recurrent episodes of supraventricular tachycardia on regular medications had another episode. Was taken up for electrophysiological study and radiofrequency ablation (EPS and RFA) under 3-D electro-anatomical mapping (EAM). The challenges in the case were need for isoprenaline infusion for sustenance of tachycardia and relatively wider area of ablation requirement for success.
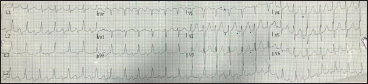
A 60-year-old male, with no atherosclerotic risk factors, had recurrent episodes of palpitations and giddiness over last 5 years. He was evaluated for the same and was advised a specialist referral for the same for an electrophysiological study (EPS). He opted for medical management at that point in time so was started on long acting betablockers for his tachycardia. He used to remain asymptomatic for about 8 to 9 months, but palpitations used to recur after that. Most of these breakthrough episodes were very short and no tachycardia ECG’s could be documented during them. The last episode lasted for a long time leading to a hospital referral and the tachycardia was documented on a 12-lead ECG at a remote centre as is shown in Figure 1. The patient was hemodynamically stable at the time of presentation so was treated with a beta blocker tablet which reverted the tachycardia to normal sinus rhythm with 1:1 atrioventricular conduction. After this episode the patient decided to take a specialist consult and an EPS was advised under 3D electro-anatomical mapping (EAM) support.
Presenting ECG shows a long RP Tachycardia (as is pointed out in V2 lead).
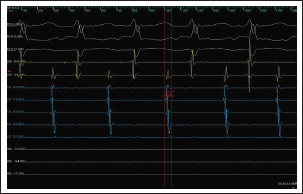
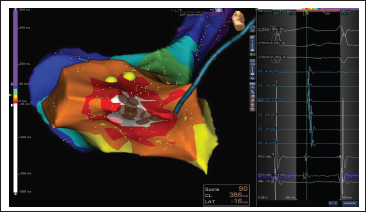
Patient had normal baseline AH and HV intervals. The clinical tachycardia was induced during the EPS with burst pacing as well as with multiple atrial extra-stimulus (AES) protocols. Based on the P-wave morphology [negative in V1; positive in V2-V4; and negative in II, III, aVF] as per the previously published algorithm, 1 the tachycardia was suspected to be having the focus around inferior tricuspid annulus. Isoprenaline infusion was needed to sustain the tachycardia. The tachycardia could not be entrained but ventriculo-atrial dissociation could be demonstrated. The intracardiac activation showed a long VA tachycardia with concentric activation [from CS proximal (CS9,10) to CS Distal (CS1,2) bipole] with earliest activation at the proximal CS (earlier than surface P-wave by 46ms) (Figure 2). This area just outside the coronary sinus ostium around inferior tricuspid annulus was mapped with 3D EAM support, to find an earlier point (about 16mins earlier than CS9,10 which was the intracardiac reference) and dense mapping was done in this region. The propagation map suggested focal origin of the tachycardia which was then ablated at and around the earliest point of activation (Figure 3). No tachycardia could be induced after the ablation even with isoprenaline with burst pacing and multiple AES protocols (waiting period 30 mins post procedure).
Intracardiac recordings confirmed a long VA tachycardia with the earliest A in proximal CS, which was 46ms earlier than the surface P wave.
Earliest region of activation with the earliest point of activation 16 ms earlier than CS9,10 (intracardiac reference).
In conclusion, atrial tachycardias are difficult to map, especially when they are non-well-sustained during the EPS. A 3D EAM helps us to map such tachycardia and ablate at and around the point of earliest activation with very high accuracy which helps with the final success of the procedure.
Footnotes
Acknowledgement
The author would like to thank Dr Praveen Kulkarni, Senior Cardiologist, Global Hospital, Mumbai for the support related to the case.
Consent Statement
A written informed consent has been taken from the patient to share the case details and images related to the procedure
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.