
Abstract
Isolated subclavian artery is a rare anomaly where the subclavian artery, instead of originating from the aorta, is connected to the ipsilateral pulmonary artery via ductus arteriosus. Presentation varies from asymptomatic to vertebrobasilar insufficiency and claudication of the ipsilateral arm. About 100 odd cases were reported in the literature. Some of them underwent definitive surgical repair, ie, reimplantation and others underwent percutaneous closure of patent ductus arteriosus thereby reducing stealing of blood and improvement of circulation in the ipsilateral arm. We are reporting a case of isolated left subclavian artery with a rare association of bilateral PDA.
Introduction
The isolated left subclavian artery is a rare anomaly with an incidence of 0.8% of all right aortic arches 1 which amounts to 4/100000 in the general population. Most of them are usually associated with other cardiac structural anomalies such as TOF, VSD, and Arch anomalies. 2
Case Report
The child was evaluated at a peripheral hospital for a breath-holding spell at 6 months of age and diagnosed with PDA. He presented at our hospital at 2 years of age with class-II breathlessness.
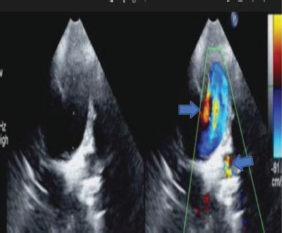
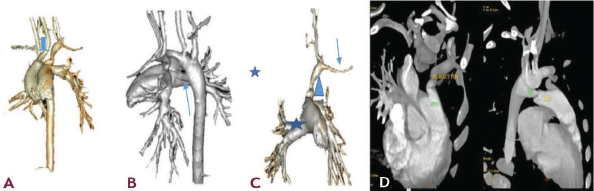
On examination, the child was acyanotic, respiratory rate of 26/min, pulse rate of 108/min, and BP (right upper limb) 90/60 mmHg. On auscultation, he had a continuous murmur in the upper right parasternal space. 2D echo revealed the right aortic arch with the right descending aorta, continuous retrograde flow into the pulmonary artery from both right and left sides (Figure 1), left subclavian artery was not originating from the aortic arch. we then checked the left upper limb pulse volume which had less pulse volume and blood pressure (76/52). We made a provisional diagnosis of the isolated left subclavian artery and right aortic arch with bilateral PDA. CT angiogram (Figure 2) was also done which confirmed our diagnosis.
Parasternal Short Axis Color Doppler across PA Showing Retrograde Continuous Flow into PA from Both Right and Left Side Indicating Bilateral PDA.
(A) Non-dividing First Aortic Branch-Left Carotid Artery (Arrow) (B) Right Side PDA (C) Left Subclavian Artery (Arrow) Is Connected to MPA (Atar) via Left PDA (Arrowhead) (D) Bilateral PDA.
Aortic angiogram in AP view showed right aortic arch with right descending aorta. Left common carotid, right common carotid, and right subclavian arteries arising from the aortic arch as first, second, and third branches, respectively (Figure 3a). There was a right-side PDA from descending aorta to RPA (Figure 3b). Later frames of aortic angiogram showed retrograde filling of the left subclavian (Figure 3c) which was connected to MPA via left PDA which was confirmed by selective right vertebral artery injection. There was retrograde flow into MPA from the left subclavian artery via left PDA (Figure 3d) indicating the steal phenomenon. The left subclavian artery was accessed from the venous side crossing RA->RV->MPA->Left PDA.
(A) Right Aortic Arch and 1st Non-dividing Aortic Arch Branch (Arrow) (B) Right PDA (Arrow) Filling MPA (c) Right Vertebral Artery (Star) Angiogram Faintly Filling Left Subclavian (Arrow) (D) Left PDA Connecting Left Subclavian and MPA (E) 6/4 PDA Occluder (Arrow) in Right PDA and 5×5 Coil (Arrowhead) in Left PDA.
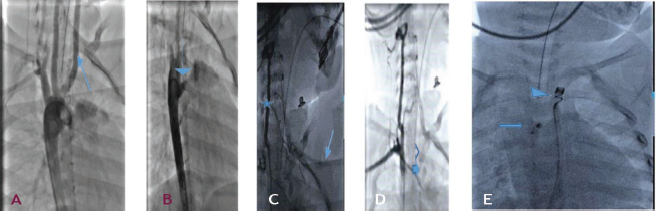
The right-side PDA was closed with a 6/4 LIFETECH® (Shenzhen, China) PDA occluder deployed through a 6F Cook® flexor Ansel sheath (Bloomington, Indiana, USA). The left side PDA was closed with a 5×5 Cook® coil (Bloomington, Indiana, USA), deployed through 5F MPA (Bloomington, Indiana, USA) (Figure 3e). The procedure was uneventful. Left upper limb BP improved immediately after the intervention.
Discussion
The right aortic arch is formed by the regression of the left dorsal aorta and the persistence of the right dorsal aorta. During normal development, fourth aortic arch connects the left seventh intersegmental artery, ie, the future left subclavian artery and aorta. Regression of the fourth aortic arch results in the isolation of the left subclavian artery. The left sixth aortic arch which develops into ductus arteriosus connects the isolated left subclavian with the pulmonary artery. 3 The seventh intersegmental artery (left subclavian) remains connected to the vertebral artery due to which there is a retrograde flow from the circle of Willis to the left subclavian resulting in cerebrovascular insufficiency. Sometimes right sixth aortic arch also persists resulting in bilateral ductus arteriosus. 4
The clinical picture of isolated subclavian is variable. About 70% of patients are asymptomatic. 2 Symptomatic patients present with neurological symptoms like syncope, transient ischemic attacks or headache because of subclavian steal resulting in vertebrobasilar insufficiency. They may present with claudication and restricted growth of the ipsilateral arm. They have low blood pressure and low volume pulses in the affected arm. Many of the patients remain asymptomatic. Also, many symptomatic patients are diagnosed late because of the rarity of the condition. In our case, patient had no symptoms and presented as a case of PDA and the final diagnosis was made after 2d echocardiography which was confirmed by a CT angiogram.
Treatment for isolated subclavian arteries includes both surgery and percutaneous intervention. Surgery is the definitive treatment where the subclavian is connected to the aorta either directly or via a bypass graft. Percutaneous closure of ductus arteriosus is also a possible treatment. If the patient is asymptomatic percutaneous device closure of the patent ductus arteriosus can be done. PDA closure decreases the amount of stealing from the circle of Willis and may improve blood supply to the ipsilateral upper limb but does not prevent the subclavian stealing from the circle of Willis and does not ensure the adequate blood supply to the limb. Hence these patients should be closely followed for symptoms and they may need surgical correction in future. If the patient presents with symptoms of limb ischemia or neurological symptoms, it is better to surgically correct the defect. Surgery is the only treatment of choice when associated with other complex congenital heart diseases. There are case reports of successful device closure of PDA in symptomatic patients5, 6. In these reports, patients improved symptomatically after the closure of the PDA. We did percutaneous device closure of bilateral PDA in the patient with isolated left subclavian with bilateral PDA. The procedure was uneventful and left upper limb blood pressure improved immediately after the procedure. The patient was discharged on the next day of the procedure.
Conclusion
At present, surgical implantation of isolated subclavian to the aorta is the standard treatment. Percutaneous closure of PDA in asymptomatic patients is a possible option but they need to be followed for the development of symptoms of vertebrobasilar insufficiency. Even though there are reports of device closure of PDA in symptomatic patients, we need further data to consider it as a treatment of choice in the isolated subclavian artery.
Footnotes
Declaration of Conf licting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This is a case report and the patient was not subjected to any newer and unapproved pharmacological or interventional. so ethical committee approval is not required.
Patient Consent
Parents gave consent to publish this case.