
Abstract
Double outlet right ventricle is a very rare association in a patient with tricuspid atresia. The anomaly has been documented in a young boy with illustrative echocardiogram, angiographic images and cardiac computed tomographic imaging. The images describing the rare anomaly would be good to understand the importance of segmental analysis in a complex heart disease.
Case Description
A 6-year-old boy weighing 14.9 kg presented to us the history of pulsatile bilateral bidirectional Glen shunt for single ventricle and pulmonary stenosis physiology at the age of 8 months. He had mild effort intolerance, oxygen saturation of 84%. The pulse rate was 80/min, the first heart sound was normal with a single second heart sound. There was 2/6 ejection systolic murmur heard at the second left intercostal space. Chest x-ray had features of reduced pulmonary blood flow. Echocardiogram revealed tricuspid atresia, unrestrictive atrial septal communication, large muscular ventricular septal defect (VSD) shunting from left to right ventricle. The left ventricle was dilated. The right ventricle was hypoplastic. Both of the outflows were predominantly originating from the right ventricle. There was significant aorta-mitral discontinuity (Figure 1 A-E). Echocardiogram in the subcostal view showed the aorta was left and anterior and pulmonary artery was right and posterior. The pulmonary artery was rightward and posterior with full commitment to the right ventricle whereas aorta was left and anterior with predominant (more than 50%) commitment to the right ventricle. Mild antegrade pulmonary flow was present with pulmonary stenosis gradient of 78 mmHg (Figure 2 A-F). The right Glenn shunt flow was good (Figure 1F). The angiogram done in another institute before (Figure 3 A-C) and after the bilateral Glenn shunt (Figure 3 D-F) confirmed the diagnosis of tricuspid atresia, muscular VSD, hypoplastic right ventricle with both great vessels predominately committed to the right ventricle. The great arteries were L malposed. The left pulmonary artery origin was suspected to be narrow in the previous institution as found in the medical record. A computed tomographic pulmonary angiogram done outside to delineate pulmonary tree showed good bilateral Glenn shunt flow. Both of the great arteries were seen committed to the right ventricle in the CT angiogram (Figure 4 A-D). The final diagnosis was tricuspid atresia, nonrestrictive muscular VSD, double outlet right ventricle and L malposed great arteries, and severe pulmonary stenosis in a child having bilateral bidirectional pulsatile Glenn shunt. The child is listed for Fontan completion.
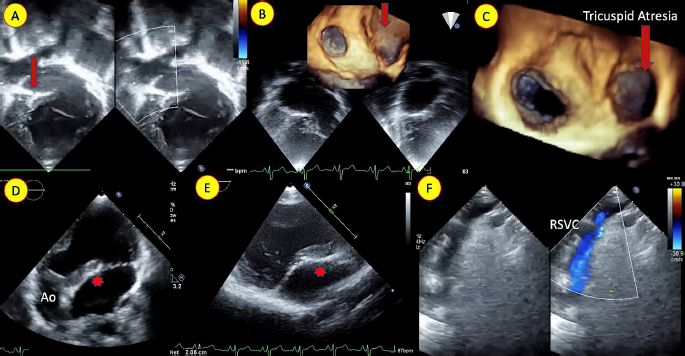
(A) Echocardiogram in apical four chamber view with color doppler showing tricuspid atresia (arrow). (B,C) 3-dimensional enface view showing atretic tricuspid valve (arrow). (D,E) Apical 5 chamber and parasternal long axis view delineating long aortomitral discontinuity (*). (F) Suprasternal view showing good right Glenn shunt flow.
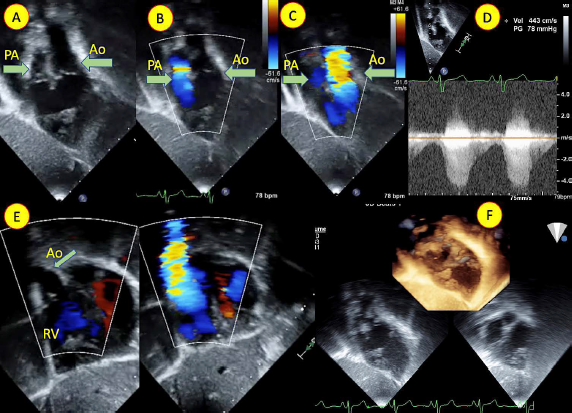
(A,B,C) Echocardiogram in subcostal oblique view and (E) subcostal short axis view with color doppler showing both the outflow (arrow) predominantly committed to the right ventricle (RV) (D) The antegrade gradient across pulmonary artery was 78 mmHg. (F) 3-dimensional echocardiographic view showing both the outflows from the RV. Ao (Aorta), PA (pulmonary artery).
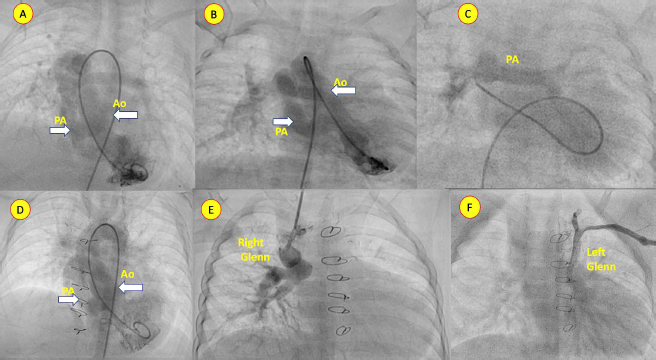
Angiogram at basal state (A,B,C) and post-bilateral bidirectional Glenn shunt (D,E,F) delineating the anatomy. (A,B,C) Frontal view angiogram showing aorta (Ao) and pulmonary artery (PA) from right-sided ventricle (arrow). Post Glenn shunt angiogram showing both great vessels predominantly committed to the right-sided ventricle. Good flow in the right (E) and left (F) Glenn shunt seen.
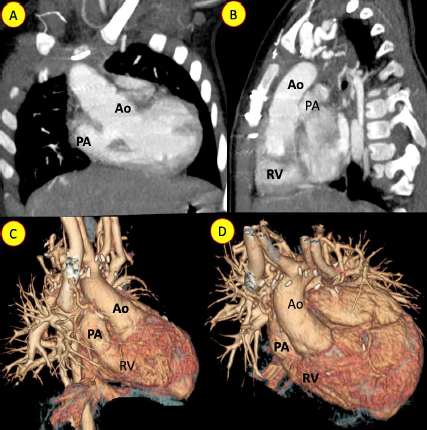
Computed tomographic angiogram in frontal (A) and lateral view (B) showing aorta (Ao) and pulmonary artery (PA) from the right and anterior ventricle. (C,D) 3-dimensional reconstruction showing the great vessel from the right-sided ventricle.
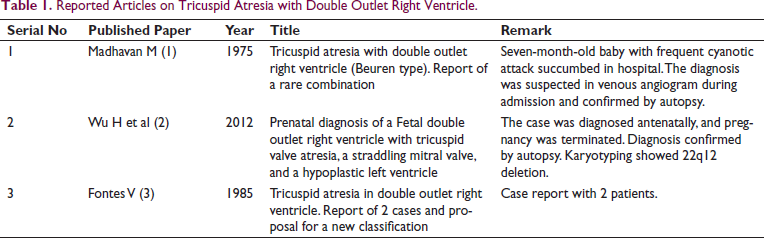
Reported Articles on Tricuspid Atresia with Double Outlet Right Ventricle.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.