
Abstract

Dear Editor,
A 60-year-old female patient, a cigarette smoker with a history of hyperlipidemia presented to the hospital with a 1-h episode of retrosternal chest pain. Physical examination revealed nothing remarkable. Electrocardiography (ECG) showed >0.1 mV ST-segment elevation (STE) in II, aVF, III, and V6, and ST-segment depression (STD) in aVL, I, and V1 to V4 (Figure 1A), ≥0.05 mV STE in V5R and V6R (Figure 1B), and >0.05 mV STE in V7 to V9 (Figure 1C). The patient received a diagnosis of infero-postero-lateral wall STE-myocardial infarction (MI) and was referred for emergency coronary angiography. Which is the culprit artery, based on the ECG findings?
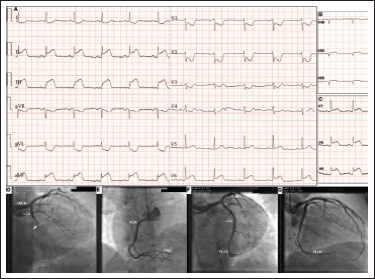
Interpretation of the ECG with use of vector concepts reveals an ST-segment vector pointing downward and somewhat rightward between +90° and +120° (STE III > II and STD aVL > I) as well as backward with less STD in V1 to V3 than STE in the inferior leads. Consequently, based on conventional ECG criteria, the right coronary artery (RCA) was most likely the culprit artery.1-3 Importantly, the ECG also reveals about 0.1 mV STD in aVR, that is a lead facing through the left ventricular cavity, the apex, and lateral wall and is directionally opposite to I, II, V5, and V6, with the latter showing about 0.2 mV STE in this case. Therefore, the ECG indicates extension of the infarction to the apical inferior and apical lateral walls thereby suggesting the presence of a large posterior-lateral left ventricular branch (PLVB). 4 The overall ECG evidence, including an isoelectric ST-segment in V4R and STD in V3 to V4 and STE in V7 to V9, which indicate extension of the infarction to the inferobasal (formerly posterior) wall can be justified by distal occlusion of a dominant RCA supplying a large PLVB. Nonetheless, the inferior-lateral wall is also supplied by the LCx artery, the occlusion of which may also result in STD in aVR. Indeed, the latter ECG sign has been reported to be more common in LCx artery-related than RCA-related MI. 4 Furthermore, in a LCx artery-related MI, the larger the inferior myocardial territory supplied by the culprit artery, as happens in a left- or codominant circulation, the more is the ST-segment vector displaced to the right and downward, thereby manifesting as an RCA-related MI in the ECG. 2 In fact, this was the case we were confronted with. Our patient had an occluded codominant LCx artery supplying a PLVB successfully recanalized with stenting (Figure 1D-G). Consequently, the correct answer to the question posed in the beginning of this report is that based on the ECG, the culprit artery is either the LCx artery or the RCA supplying a large-sized PLVB. The STE in V5R and V6R could be reciprocal to a posteriorly directed ST-segment vector manifested as STD in V3 to V4. 3
This case calls attention to the presence of STD in aVR in inferior STE-MI that suggests involvement of the inferolateral, apical inferior, and apical lateral walls which are supplied by a PLVB stemming either from the LCx artery or the RCA. This ECG sign (STD in aVR ≥0.1 mV) has been identified as a marker of large infarct and impaired myocardial reperfusion, thereby facilitating identification of high-risks patients and consequently application of the most appropriate therapies likely to benefit such patients. 5 Furthermore, as highlighted herein, it should also raise suspicion for possible misidentification of the RCA instead of the LCx artery as the culprit vessel by conventional ECG algorithms. Inclusion of aVR into ECG analysis may therefore help avoid diagnostic and therapeutic misadventures and this can be facilitated by ECG display of the limb leads in their anatomically contiguous order (Cabrera sequence) incorporating AVR (+30°). 5
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.