
Abstract
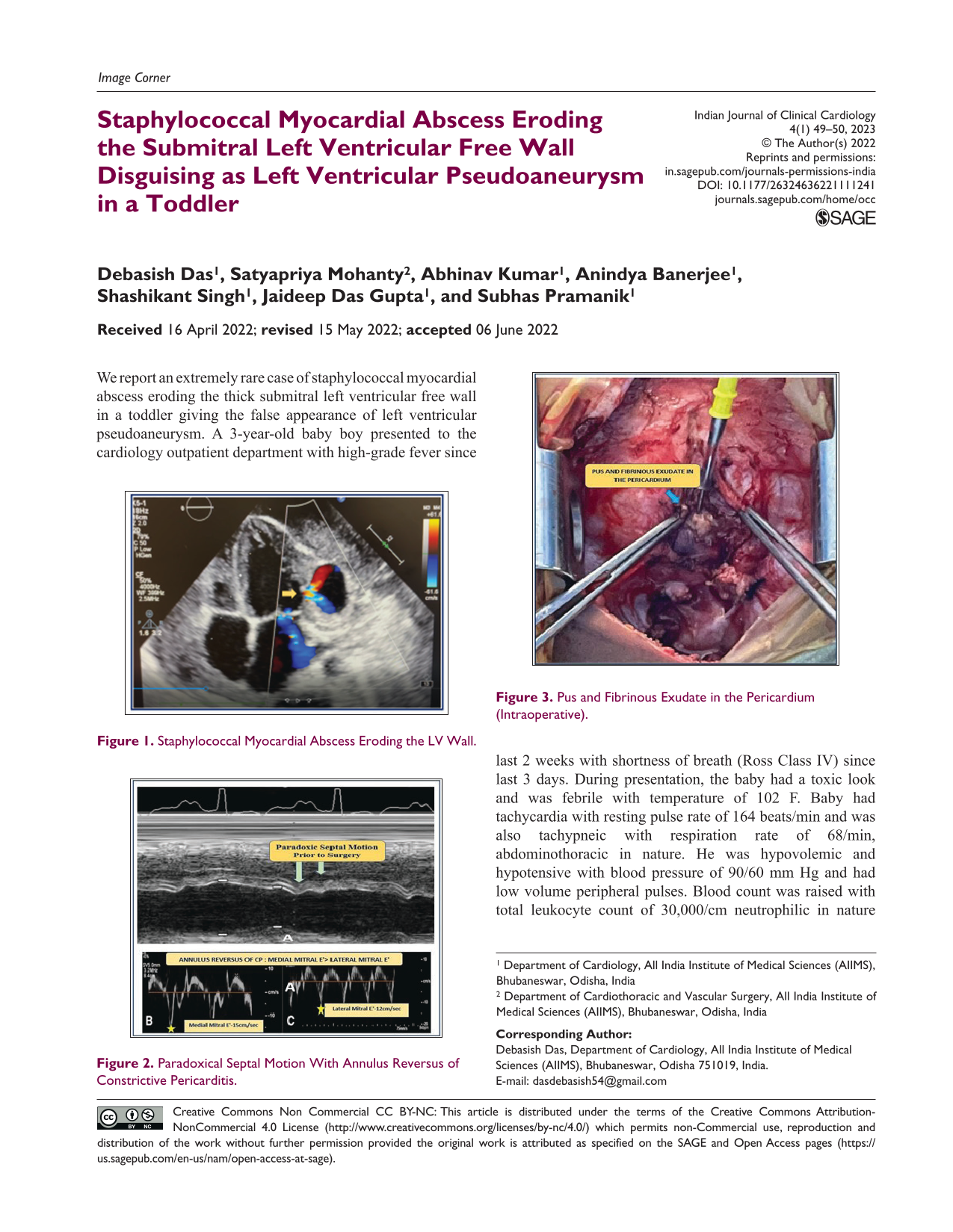
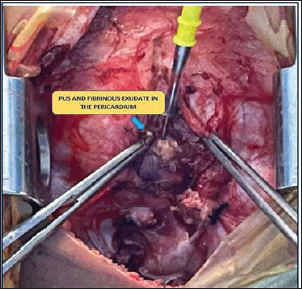
We report an extremely rare case of staphylococcal myocardial abscess eroding the thick submitral left ventricular free wall in a toddler giving the false appearance of left ventricular pseudoaneurysm. A 3-year-old baby boy presented to the cardiology outpatient department with high-grade fever since last 2 weeks with shortness of breath (Ross Class IV) since last 3 days. During presentation, the baby had a toxic look and was febrile with temperature of 102 F. Baby had tachycardia with resting pulse rate of 164 beats/min and was also tachypneic with respiration rate of 68/min, abdominothoracic in nature. He was hypovolemic and hypotensive with blood pressure of 90/60 mm Hg and had low volume peripheral pulses. Blood count was raised with total leukocyte count of 30,000/cm neutrophilic in nature with C-reactive protein of 30 ng/mL and raised procalcitonin. Chest X-ray posteroanterior view revealed the presence of right paracardiac consolidation. Echocardiography revealed the presence of a large myocardial abscess in the submitral region eroding the left ventricular free wall creating a false impression of left ventricular pseudoaneurysm (Figure 1). The blood passing through the eroded left ventricular wall was forming a small pool inside the myocardial wall and the myocardial abscess was also vomiting out pus to the whole pericardial sac which was filled with organized thick layer of pus and fibrinous exudate almost as thick as the left ventricle dimension. Septal bounce was prominent in echocardiography indicating early phase of effusive constrictive pericarditis along with paradoxic septal motion and annulus reversus (Figure 2). The child had engorged inferior vena cavae with mild ascites also. He was evaluated for primary immunodeficiency in the form of Job syndrome. Serum IgE was within normal limit (<60 IU/mL). Blood culture revealed the growth of methicillin-sensitive Staphylococcus aureus which was sensitive to meropenem and vancomycin. He was planned for surgical evacuation of the pooled pus in the pericardial sac (Figure 3) with pericardiectomy and marsupialization of the pericardial sac in the submitral region so that the area of left ventricular erosion by myocardial abscess would heal by secondary intention and it will be sealed off by the fibrosed pericardial wall. The site of erosion in the left ventricular wall could not be sutured as the weakened left ventricular wall by the myocardial abscess would not hold the purse string bite for apposition. Post procedure, the baby was kept on intravenous antibiotic therapy for 14 days with meropenem and vancomycin. The baby became afebrile after 7 days of antibiotic therapy without any shortness of breath and was doing well in follow-up after 1 month. Our case is the first description of staphylococcal myocardial abscess eroding the left ventricular free wall in a toddler with simultaneous effusive constrictive pericarditis. Toxic staphylococcus can also erode the thick left ventricular wall. 1
Staphylococcal Myocardial Abscess Eroding the LV Wall.

Paradoxical Septal Motion With Annulus Reversus of Constrictive Pericarditis.
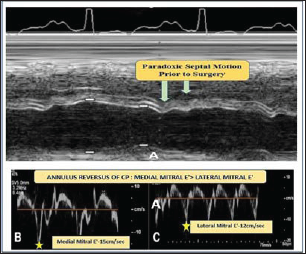
Pus and Fibrinous Exudate in the Pericardium (Intraoperative).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Institutional Ethical Committee (IEC) approval has been obtained.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Informed patient consent has been obtained.