
Abstract
A 32-year-old male presented with complaints of chest discomfort and resting palpitations since 1 day. He is nonsmoker, nondiabetic, and normotensive. Electrocardiogram showed changes of ventricular tachycardia. He has episodes of recurrent brief palpitations since 3 to 4 years. Echo showed global hypokinesia of left ventricle, mild systolic and diastolic dysfunction of left ventricle, trivial mitral regurgitation, and trivial tricuspid regurgitation. Cardiac magnetic resonance imaging (MRI) and cardiothoracic positron emission tomography (PET) scan were done.
Cardiac MRI Findings
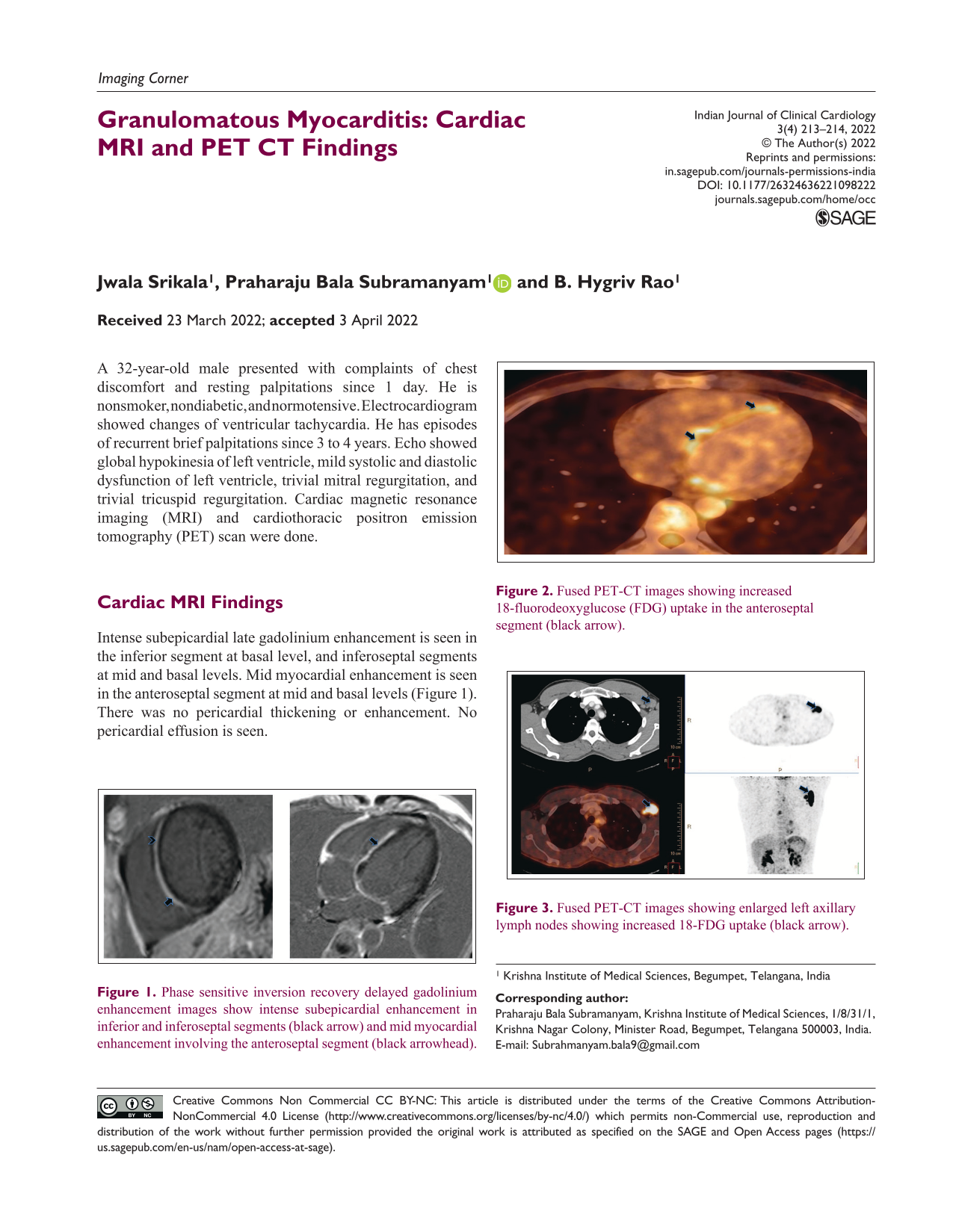
Intense subepicardial late gadolinium enhancement is seen in the inferior segment at basal level, and inferoseptal segments at mid and basal levels. Mid myocardial enhancement is seen in the anteroseptal segment at mid and basal levels (Figure 1). There was no pericardial thickening or enhancement. No pericardial effusion is seen.
Phase sensitive inversion recovery delayed gadolinium enhancement images show intense subepicardial enhancement in inferior and inferoseptal segments (black arrow) and mid myocardial enhancement involving the anteroseptal segment (black arrowhead).
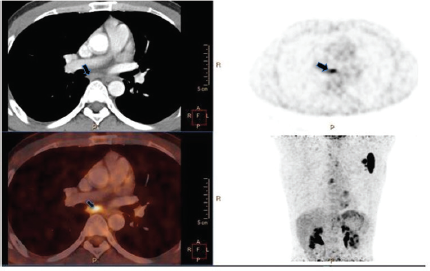
PET CT Findings
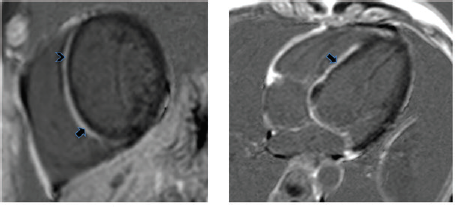
Increased 18-fluorodeoxyglucose (FDG) uptake is seen in the myocardial septum at all levels. Increased 18-FDG uptake is noted in few mediastinal lymph nodes and an enlarged left axillary lymph node (Figures 2-4).
Fused PET-CT images showing increased 18-fluorodeoxyglucose (FDG) uptake in the anteroseptal segment (black arrow).
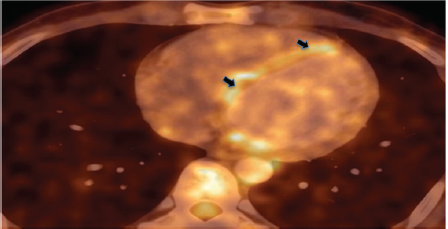
Fused PET-CT images showing enlarged left axillary lymph nodes showing increased 18-FDG uptake (black arrow).
Fused PET-CT images showing subcarinal lymph node showing increased 18-FDG uptake (black arrow).
Cardiac MRI and PET computed tomography (CT) features were in favor of granulomatous myocarditis, most probably due to sarcoidosis. However, because of the mediastinal and axillary lymphadenopathy, tuberculous myocarditis was also considered.
Excision biopsy was done from the left axillary lymph node. Histopathological examination showed features of necrotizing granulomatous inflammation favoring Koch’s etiology. Along with other supportive biochemical and microbiology investigations, a diagnosis of tuberculous granulomatous myocarditis was made.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.