
Abstract

Case
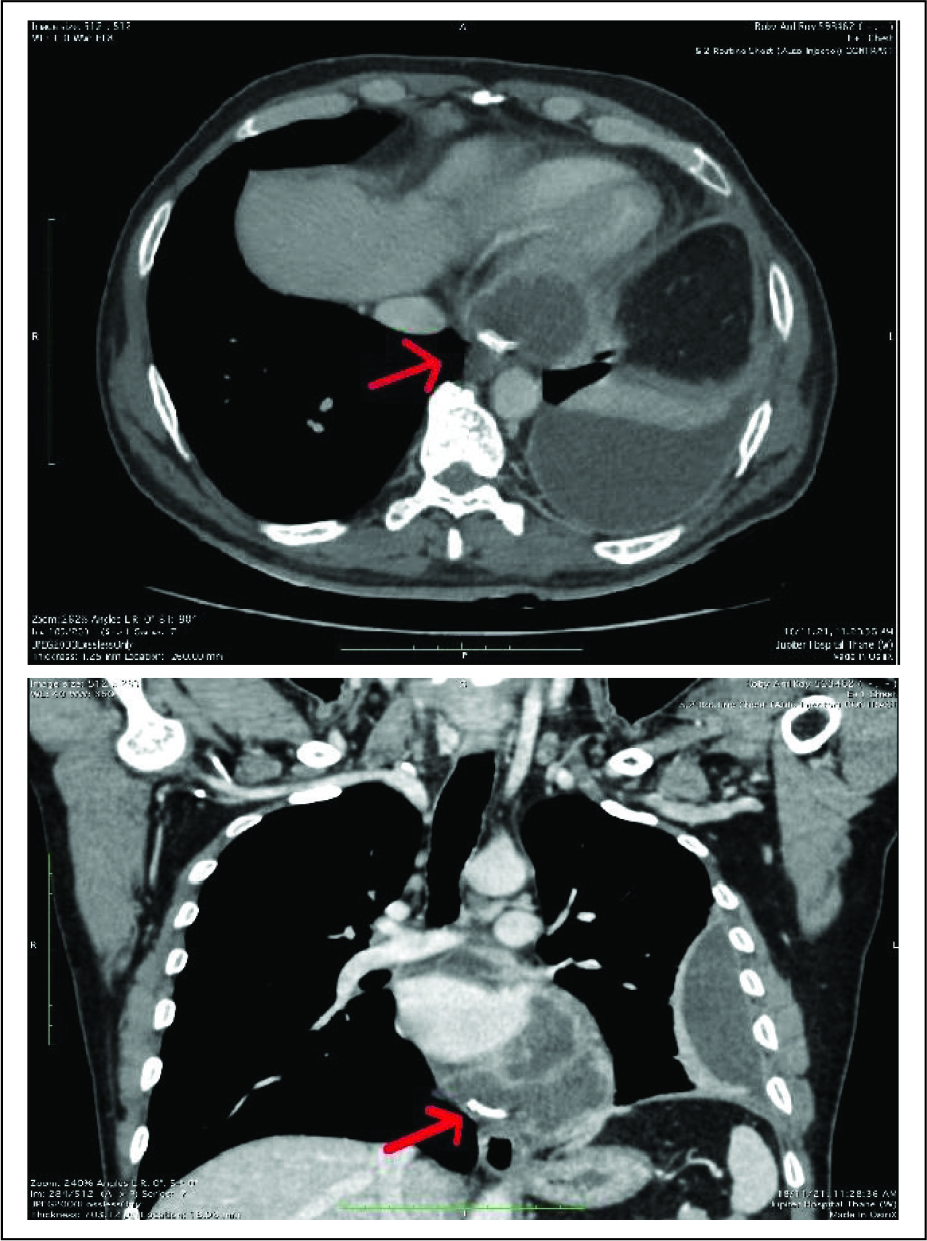
A 50-year-old male presented to chest outpatient department with persistent fever. He had prior medical history of coronary stent implantation in the left anterior descending artery (LAD) and left circumflex artery (LCX) in 2016. Chest X-ray revealed blunting of left costophrenic angle with loculated pleural effusion along the left lateral chest wall. On further investigation with contrast computerized tomography (CT) scan, loculated left-sided pleural effusion was confirmed (Figure 1A and B). In addition to this, pericardial collection was observed with peripheral post contrast enhancement. A linear hyperdense structure with adjacent streak artifacts was observed within this pericardial collection, consistent with stent.
(A) (Left) and (B) (Right). Axial and coronal sections of a contrast enhanced CT scan of chest showing left-sided loculated pleural effusion and a pericardial effusion. Red arrow points to the extraluminally migrated stent in the pericardial sac.
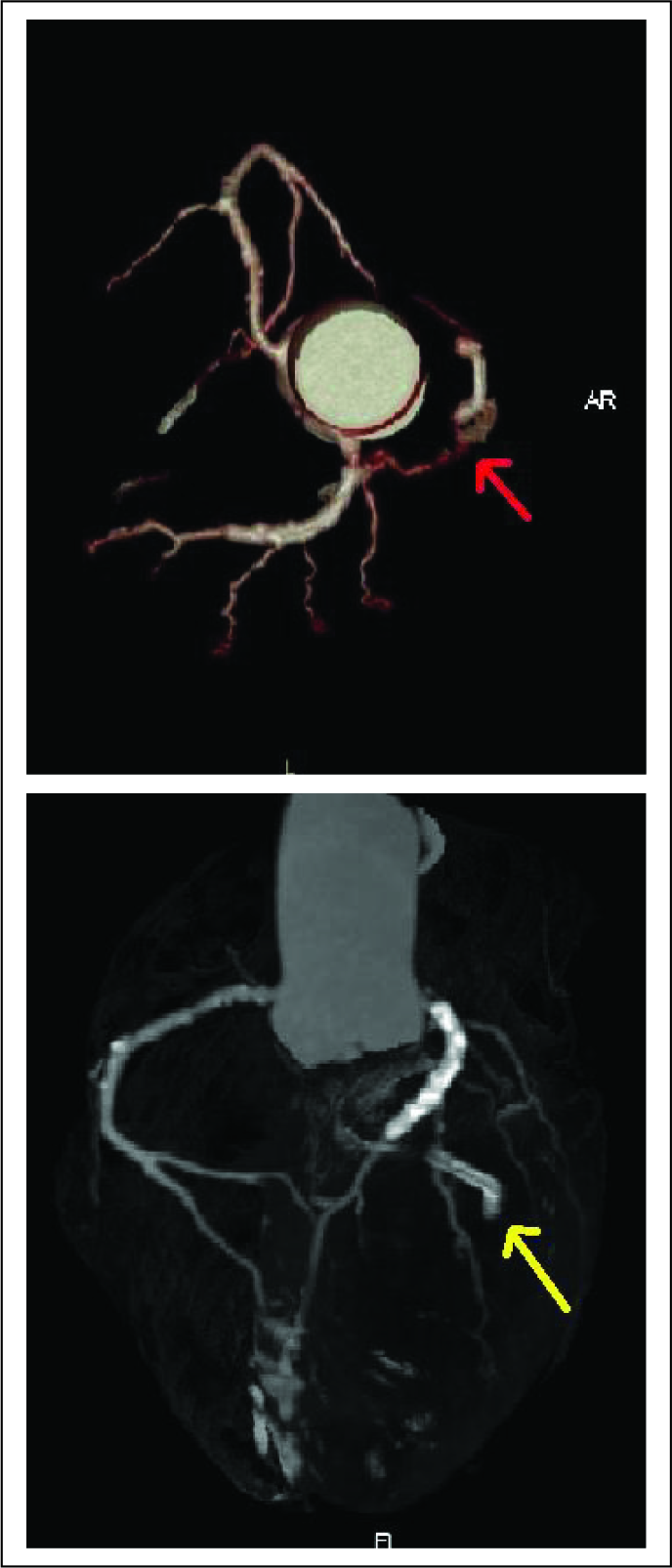
CT angiogram was then performed to ascertain the integrity of the coronary vessels. LAD stent was noted in situ with adequate intraluminal contrast opacification. There was no evidence of in stent restenosis. Moderate narrowing and irregularity of the left circumflex coronary artery was seen only in proximal segment (Figure 2A and B). Distal segment was not opacified. This LCX coronary stent was not seen along its expected course and was found to be located in the basal portion of the pericardial effusion.
(A) (Left) and (B) (Right). Red arrow points to the proximal segment of the LCX which shows narrowing and irregularity with no flow in distal segment. Yellow arrow points to a migrated stent away from the expected course of the LCX.
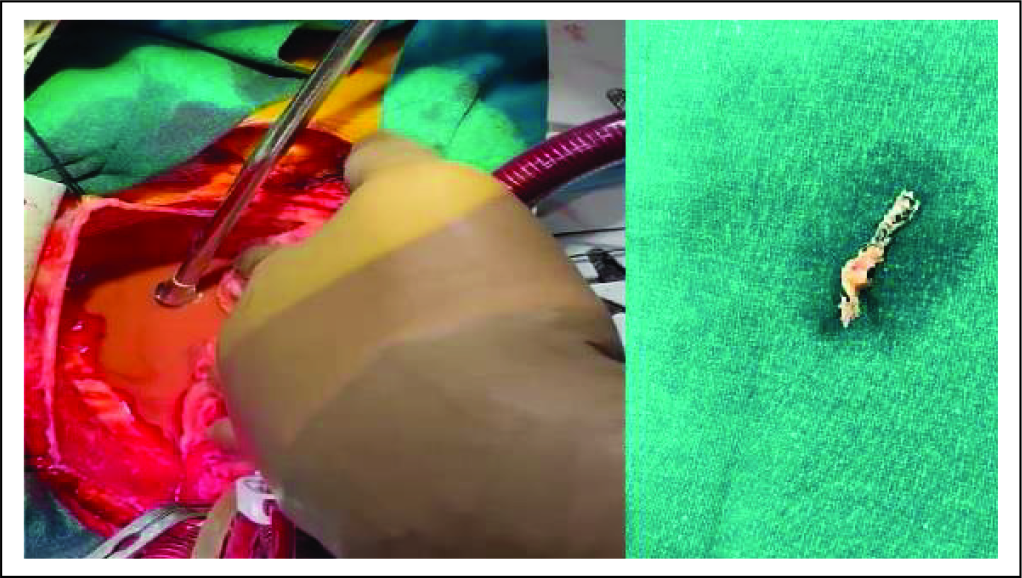
The patient was electively taken up for open surgery. Purulent pericardial collection was aspirated (Figure 3A and B). Migrated stent was retrieved from this pericardial collection. Patient had good recovery with adequate postoperative care.
(A) (left) and (B) (Right). Pus within the pericardial sac being drained as shown in (A). Migrated stent removed from the pericardial sac shown in (B).
Discussion
Extraluminal stent migration of coronary stent is rare complication and has not been frequently reported in literature. Complications of coronary stenting include stent occlusion, stenosis, stent migration, and fracture. Only few cases of extraluminal stent migration have been reported in literature. Presence of a coexisting coronary artery aneurysm has been described in a few case reports.
Extraluminal migration of a stent in right coronary artery with prior history of blunt trauma has been described. Stent fracture has also been attributed as a possible cause of stent migration.
However, unique finding in our case was the presence of delayed presentation and purulent pericardial collection. In our case, the coronary stent was found be extraluminally located in the pericardial sac. Intraoperatively, pus was found within the pericardial cavity suggestive of infective disease process.
The cause of stent migration is not clear in our case. The arterial wall damage with subclinical infection triggering the migration of the stent can be theorized. No other cause such as trauma or coexisting aneurysm could be identified in our case.
MDCT coronary angiography provides adequate visualization of the stent position. It provides wider field of view and helps in evaluation of other associated lung and pericardial pathologies. With advances in CT imaging technology, CT angiography is preferred and reliable tool in diagnostic workup and our case demonstrates the same!
Footnotes
Acknowledgement
The authors would like to acknowledge the guidance of Dr Priya Chudgar for the write-up of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.