
Abstract
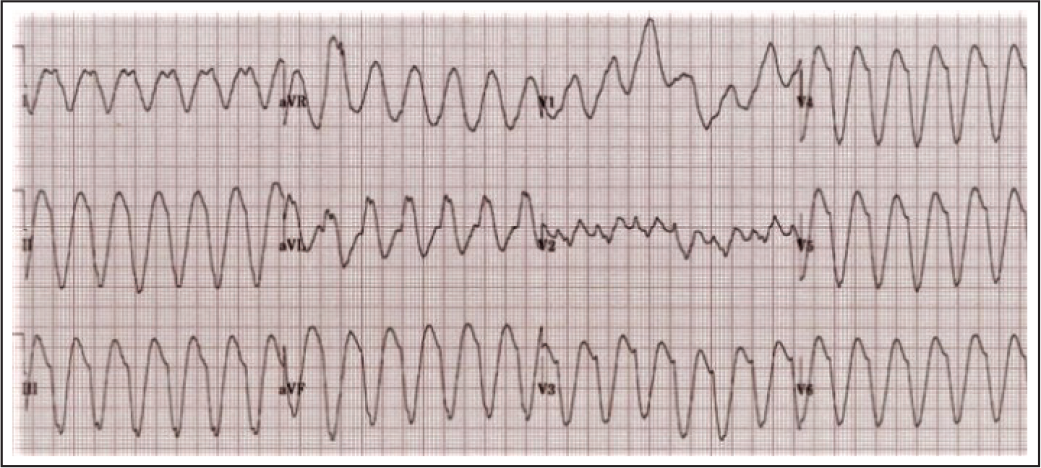
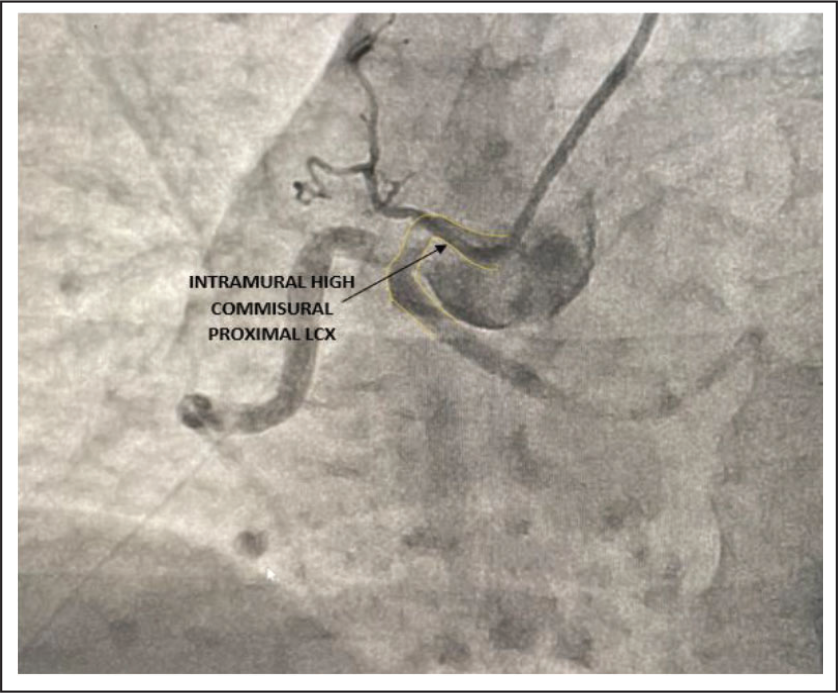
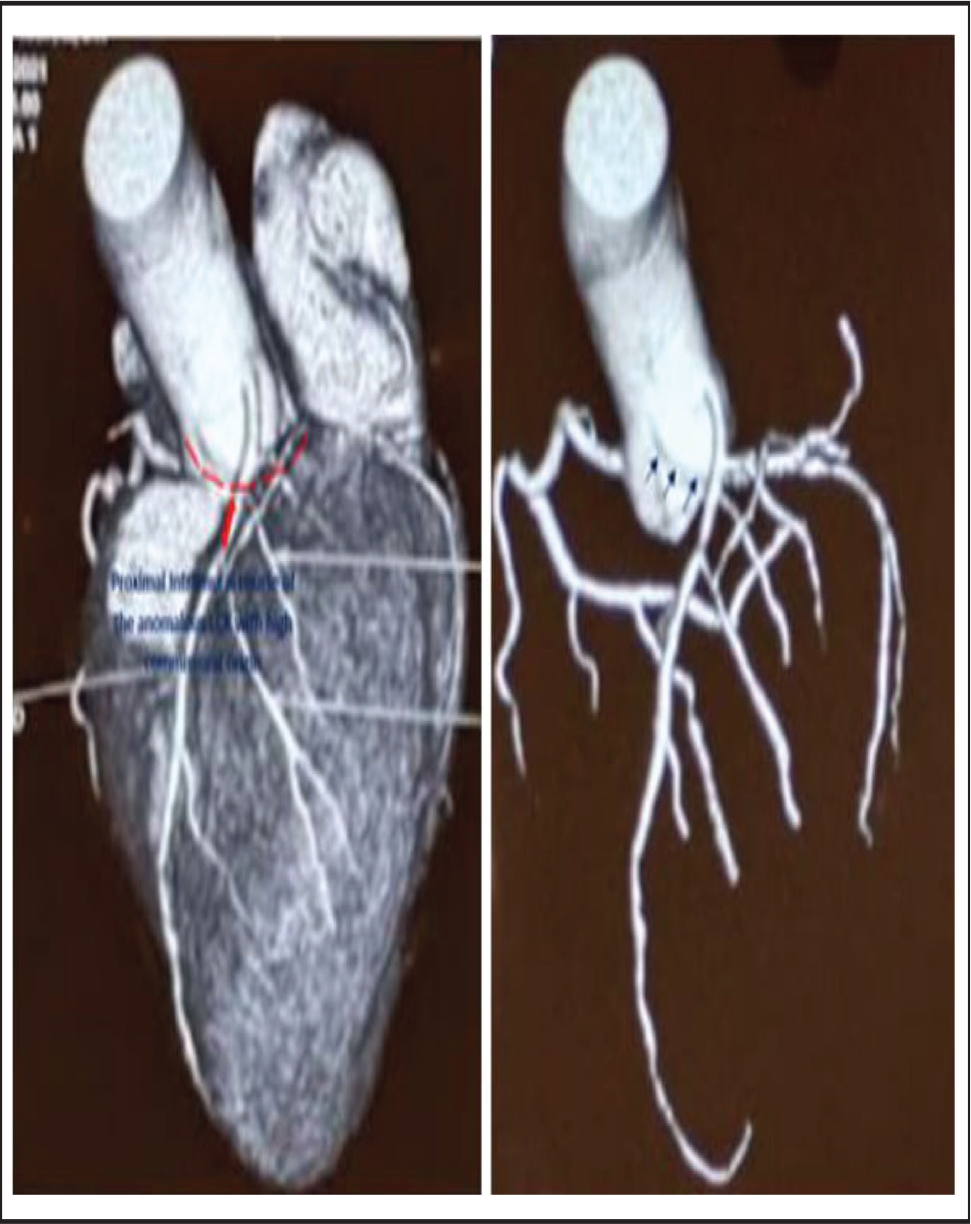
We report a rare case of monomorphic ventricular tachycardia in a 23-year-old male with hemodynamic collapse secondary to intramural aortic course of anomalous left circumflex coronary artery (LCX). The anomalous LCX had high commissural origin at the junction of the left and right coronary sinus. A 23-year-old male, an engineering graduate without conventional cardiac risk factors and negative family history, presented to the cardiac emergency department with hemodynamic collapse and syncope. He had blood pressure of 80/40 mm Hg with heart rate of 180 beats per minute. Electrocardiogram revealed monomorphic ventricular tachycardia (Figure 1) which was direct current (DC) verted with 180 J biphasic DC shock. Serum chemistries were within normal limit including serum electrolytes (Na+, K+, Ca++, Mg++). Echocardiography was within normal limit without the evidence of regional wall motion abnormality with normal biventricular systolic function. Cardiac troponin was negative. He was subjected to invasive coronary angiogram which revealed anomalous origin of the LCX from the junction between the left and right coronary artery high in the commissure without any atherosclerotic obstruction in any of the coronaries (Figure 2). Cardiac magnetic resonance imaging did not reveal any presence of delayed enhancement after Gadolinium suggestive of scar. Holter analysis did not reveal any premature ventricular complexes. CXR PA view, serum angiotensin-converting enzyme, and Serum Ca were all within the normal limit. Fluorodeoxyglucose-positron emission tomography scan did not reveal any uptake by perihilar lymph nodes suggestive of active sarcoid in the young. We did a 160 Slice computed tomography coronary angiogram which revealed complete intramural course of the anomalous proximal LCX (Figure 3). It was the culprit behind the ischemic ventricular tachycardia in this young secondary to long aortic intramural course of the anomalous coronary. We managed the patient with optimum betablocker, amiodarone, and automatic implantable cardioverter-defibrillator implantation. In the event of occurrence of recurrent or drug refractory ventricular tachycardia (VT) in future, revascularization with a graft to distal LCX was planned. Anomalous coronary artery can produce ventricular tachycardia and fibrillation secondary to ischemic scar present in the myocardium.1, 2 Our case is a unique and first demonstration of complete intramural course of the anomalous LCX with high commissural origin causing ischemic VT in a young without the presence of myocardial scar.
Run of Ventricular Tachycardia With Hemodynamic Collapse.
Invasive CAG Revealing Intramural High Commisural Proximal LCX.
160 Slice CT Coronary Angiogram Showing Long Proximal Intramural Course of the Anomalous LCX with High Commissural Origin.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.