
Abstract
A case is presented of a patient requiring percutaneous mitral balloon commissurotomy. During positioning of the transseptal needle, an unusual needle position on the lateral projection prompted the physician to abandon the puncture and do an angiogram of the inferior vena cava. This revealed an azygous vein continuation. The valve was treated at a later date under general anesthesia with transesophageal echo guidance. This case illustrates how reliance on the posterior-anterior projection to find the optimal point for transseptal puncture can be very misleading and how crucial the lateral projection is.
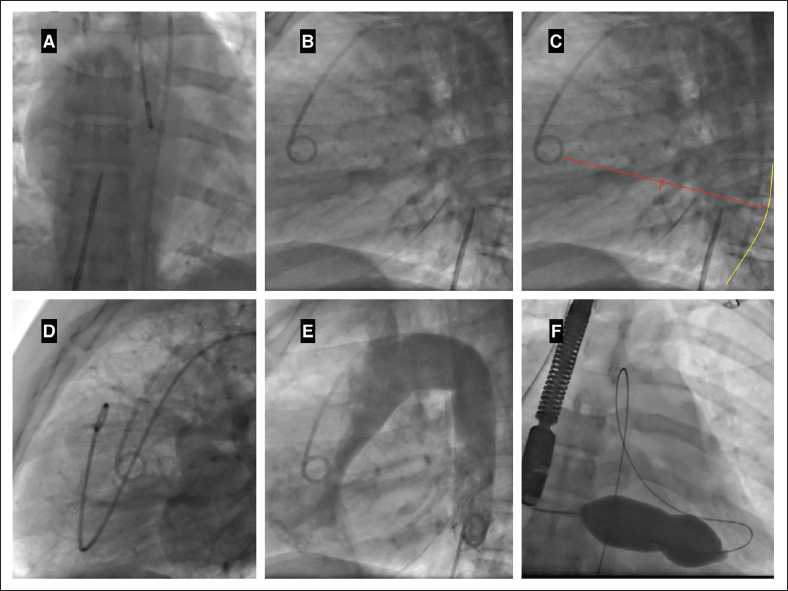
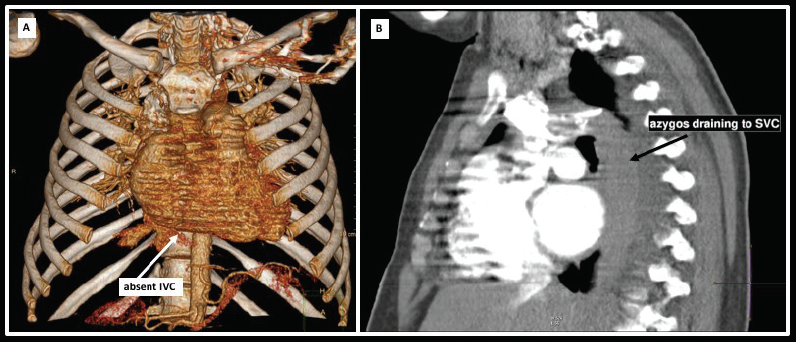
A 36-year-old female patient presented with limiting dyspnea due to severe rheumatic mitral stenosis and a valve suitable for percutaneous transseptal mitral commissurotomy. As per our standard practice, a pigtail catheter was placed into the pulmonary artery (using [posterior-anterior] PA projection) and an arteriogram was performed to delineate the left atrial anatomy. A Mullins sheath (St. Jude Medical) was then advanced over a wire into the superior vena cava (SVC) and withdrawn into the right atrium in a PA projection (Supplemental Video 1). Prior to transseptal puncture, the relation of the Mullins sheath and transseptal needle assembly was viewed in the PA (Figure 1 Panel A) and lateral (Figure 1 Panel B) projections. The needle appeared to be too posterior on the lateral projection (Figure 1 Panel C: diagram showing the ideal puncture point on the lateral projection—halfway to two-thirds between the pigtail catheter in the aorta and the spine—yellow line; Figure 1 Panel D shows the left atrial border during a prolonged pulmonary artery injection) and an angiogram of the inferior vena cava (IVC) was done. This showed an azygous continuation of the IVC that drained into the SVC (Figure 1 Panel E, Supplemental Video 2). This was confirmed on subsequent computed tomography imaging which demonstrated an interrupted IVC (Figure 2 Panel A) and the azygous vein draining into the SVC (Figure 2 Panel B). The procedure was abandoned and performed at a later date under general anesthesia using transesophageal echocardiography guidance. A jugular approach with an over-the-wire technique was used and the valve successfully dilated with a 28-mm NuCLEUS-X balloon (Numed) (Figure 1 Panel F).
This case illustrates how reliance on the PA projection to find the optimal point for transseptal puncture can be very misleading and how crucial the lateral projection is.
Postero-anterior (Panel A) and lateral (Panel B) projection at the time of initial planned transseptal puncture. (PANEL C) - ideal puncture point for transseptal puncture on lateral projection. (PANEL D) - prolonged pulmonary artery injection demonstrating left atrial border. (PANEL E) - Angiogram of the inferior vena cava demonstrating azygous continuation. (PANEL F) - Successful mitral balloon commisurotomy.
(PANEL A) Computed tomography reconstruction demonstrating the absent inferior vena cava; (PANEL B) - Computed tomography demonstrating the azygous vein draining into the superior vena cava.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.