
Abstract
Objective:
Assessment of right ventricular (RV) diastolic function in postoperative Tetralogy of Fallot (TOF) patients is not routinely done during intermediate follow-up. We have done this study to assess the incidence and type of RV diastolic dysfunction in these patients.
Method:
Ninety patients who were less than 18 years and underwent total correction for TOF were analyzed in this study. The incidence and type of RV diastolic dysfunction was measured and the effect of degree of pulmonary regurgitation on RV diastolic function was also seen.
Results:
The total number of patients with RV diastolic dysfunction was 46 (51.1%). Restrictive RV physiology was seen in 8 patients (8.8%) and the most common type of RV diastolic dysfunction seen was pseudonormal filling, seen in 23 (25.6%) patients.
Conclusion:
Subclinical RV diastolic dysfunction is present in almost half of the postoperative TOF patients of pediatric age group. The most prevalent form of diastolic dysfunction was pseudonormal filling during intermediate follow-up.
Introduction
Tetralogy of Fallot (TOF) is one of the most common cyanotic congenital heart diseases. The perioperative mortality has reduced significantly in the current era (<4%) 1 but the long-term survival is still not equal to the general population. This is because of the presence of a slowly evolving postoperative pathophysiology. 2 Thus, it is necessary for them to be under follow-up throughout their life to monitor for the adverse outcomes. Echocardiography is one of the most important tools in the follow-up of postoperative TOF patients. But the focus mainly remains on right ventricular (RV) systolic function and RV diastolic function is often not assessed. Thus, the exact incidence of RV diastolic dysfunction is not clearly known, especially during the intermediate follow-up. RV restrictive physiology is a well-known phenomenon seen in the immediate postoperative period and during long-term follow-up in postoperative TOF patients but the incidence of impaired relaxation and pseudonormal filling is not known in the pediatric age group, especially during intermediate follow-up. Thus, the purpose of this study is to assess the incidence and type of RV diastolic function in postoperative TOF patients of pediatric age group.
Material and Methods
Design of Study and Participants
It was a single-center prospective, observational study in which eligible patients were included from the outpatient department.
Aims and Objectives
To study the incidence and type of RV diastolic dysfunction in postoperative TOF patients.
To see the effect of time since total correction on RV diastolic function.
To see the effect of pulmonary regurgitation (PR) on RV diastolic function.
Inclusion Criteria
Postoperative TOF patients less than 18 years old who underwent total correction surgery and were at least 6 months postoperative.
Exclusion Criteria
TOF patients with associated significant atrioventricular valve regurgitation or any systemic condition which can affect the cardiac function.
Echocardiographic Evaluation
Clinical variables were recorded (patient’s age, weight, height, and duration of the postoperative follow-up).
Depending on the origin of the diastolic flow reversal, PR was graded in the parasternal short axis view. PR was taken as mild if the diastolic flow reversal originated from the main pulmonary artery, moderate PR if it started from the bifurcation of the pulmonary artery, and severe PR if it was from the distal pulmonary artery branches. 3
TV inflow: Pulse wave doppler of tricuspid valve (TV) inflow was taken to measure the E and A velocity.
TV-TDI derived e’ and a’ velocity were taken by measuring the Tissue Doppler imaging (TDI) velocity at the lateral tricuspid valve annulus.
E/e’ and E/A ratio was calculated.
E wave deceleration time (DT): This was measured if the E/A was more than 2.1.
Pulse wave doppler in the pulmonary artery: Late diastolic antegrade flow in the pulmonary artery seen during both inspiration and expiration or seen in ≥5 consecutive beats was taken as evidence of restrictive RV physiology.
All of the transtricuspid doppler velocities were measured at end-expiration and/or the average of ≥5 consecutive beats were taken.
Grading of RV diastolic dysfunction was done as follows
4
:
Impaired relaxation: Tricuspid E/A ratio <0.8 Pseudonormal filling: Tricuspid E/A ratio of 0.8 to 2.1 with an E/e’ ratio >6. Restrictive RV physiology: Tricuspid E/A ratio >2.1 with a DT <120 ms and/or presence of late diastolic antegrade flow in the pulmonary artery.
All the patients were divided into 3 groups based on the duration since total correction for analysis of outcomes and RV diastolic function are as follows:
Group A: 6 months to 5 years Group B: 6 to 10 years Group C: >10 years
To study the effect of degree of PR on RV diastolic function, the patients were divided into 2 groups, that is, those with severe PR and those with mild to moderate PR.
Statistical Methods
Descriptive statistics for categorical variables were reported as frequency and percentage, whereas continuous variables were reported as mean and standard deviations. For the statistical comparison between the 3 groups, ANOVA test was applied. For the comparison of RV diastolic function between patients with severe PR and mild to moderate PR, unpaired t-test was applied. P value of <.05 was taken as statistically significant.
Ethics
The study was undertaken after ethical clearance from the institute’s ethical committee. The purpose and design of the study was explained to the patients or the consenting family members. The parents or consenting family members were informed that they can ask to withdraw from the study at any time without having reasons for the same. The confidentiality of information obtained was maintained and revealed only to doctor/auditor involved in study and to regulatory authorities. The study was conducted on ethical guidelines for biomedical research on human subjects given by Central Ethical Committee on Human Research, New Delhi, in addition to principles enunciated in the “Declaration of Helsinki.”
Results
Patient Characteristics
In this study, a total of 90 patients were enrolled who underwent total correction for TOF and met the inclusion criteria. Out of these 90 patients, 71 were males (78.8%) and 19 (21.2%) were females. The mean age at total correction was 3.06 ± 2.94 years. Total correction in all patients was done by the same surgeon using trans atrial-trans pulmonary approach. Fifty-seven patients (63.3%) needed transannular patch (TAP).
Follow-up
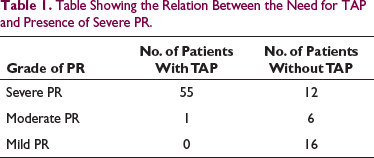
The mean time was since total correction was 6.55 ± 4.30 years (median = 6 years). PR was severe in 67 (74.44%) patients. As seen in Table 1, those patients with TAP had more likelihood of having severe PR as compared to those who did not undergo a TAP.
Table Showing the Relation Between the Need for TAP and Presence of Severe PR.
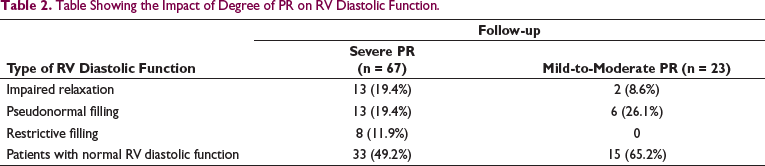
Impact of the degree of PR on RV diastolic function:
The number of patients with RV diastolic dysfunction was 34 (50.7%) in those with severe PR and 8 (34.7%) patients with mild-to-moderate PR (Table 2).
Table Showing the Impact of Degree of PR on RV Diastolic Function.
Group-Wise Analysis of Patients
Group A comprised of patients whose time since total correction is 6 months to 5 years, which amounted to 34 (37.99%) patients. The mean age was 4.92 ± 4.0 years and mean time since total correction was 1.83 ± 0.85 years. RV diastolic function was normal in 22 (64.7%) patients. Impaired relaxation was seen in 4 (11.76%) patients and 6 (17.64%) patients had pseudonormal pattern. Two (5.88%) patients had features of restrictive filling as shown in Table 3.
Table Showing the RV Diastolic Function Group Wise.

Group B included patients whose time since total correction is 6 to 10 years, which amounted to 26 (28.88%) patients. The mean age was 8.05 ± 1.34 years and mean time since total correction was 6.55 ± 0.98 years. As seen in Table 3, 15 (57.6%) patients had normal RV diastolic function, 4 (15.38%) had impaired relaxation, 6 (23.07%) had pseudonormal filling, and 1 (3.84%) patient had restrictive filling.
Group C included patients whose time since total correction is more than 10 years and included a total of 30 (33.33%) patients. The mean age was 14.4 ± 1.88 years and mean time since total correction was 11.9 ± 1.05 years. Seven (23.33%) patients had normal RV diastolic function, 7 (23.33%) had impaired relaxation, 11 (36.66%) had pseudonormal filling, and 5 patients (16.6%) had findings suggestive of restrictive filling as shown in Table 3.
Comparison of RV Function Between the Three Groups
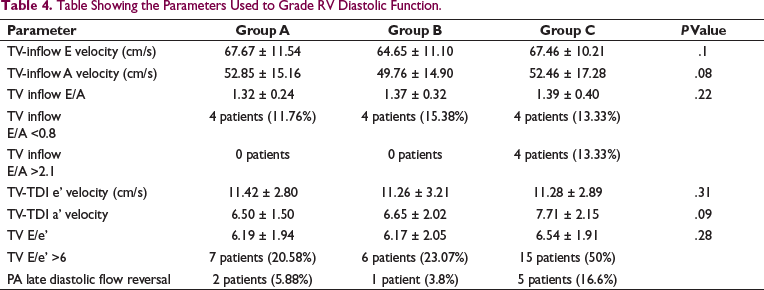
Table 3 shows the number of patients with RV diastolic function group wise. It is seen that the most common type of RV diastolic dysfunction was pseudonormal filling seen in 23 (25.5%) patients. It is also seen that group C had the maximum number of patients with RV diastolic dysfunction. Table 4 shows the individual parameters used for assessment of RV diastolic function. It was seen that there was no statistically significant difference in the mean tricuspid valve inflow velocity E and A, mean tissue doppler velocity of lateral tricuspid valve e’ and a’ inflow E velocity between the 3 groups. Also, the mean E/A and E/e’ ratio were not statistically different as shown in Table 4. But the number of patients with E/A ratio of more than 2.1 and E/e’ more than 6 were more in group C patients.
Table Showing the Parameters Used to Grade RV Diastolic Function.
Discussion
Number of Patients With RV Diastolic Dysfunction
The total number of patients with RV diastolic dysfunction was 46 (51.1%) in this study. In a recent study, 62.5% TOF patients had echocardiographic evidence of RV diastolic dysfunction in the postoperative period. 5 In our study, 15 (16.7%) patients had impaired relaxation. Pseudonormal filling was seen in 23 (25.6%) patients. Restrictive filling was seen in 8 (8.8%) patients (Table 3). Of the 8 patients with restrictive physiology, all had TAP and severe PR. All these patients had E/A ratio >2.1, except for 2 patients. And all had DT <120 ms except for 1 patient. Similar finding was seen in a study done by Dilorenzo et al, 6 where they assessed diastolic function in postoperative TOF patients with mean age of 8.9 years. It was seen that 20 patients (21.2%) had impaired relaxation, 36 patients (39.5%) had pseudonormal filling, and only 3 patients (3.2%) had restrictive physiology. Most of the studies on RV diastolic function have a prevalence of restrictive physiology in the range of 50 to 70%. 7 The reason for such a variable number is the different methods used to measure RV diastolic function, and the time when it was measured. Restrictive RV physiology is seen at 2 time periods, 1 in the immediate postoperative period and 1 at long-term follow-up. In the immediate postoperative period, it seems to normalize by 2 weeks in most of the patients. 8 In our study, the mean time since total correction was 6.55 ± 4.30 years for the whole group, and it was 11.9 ± 1.05 years in group C patients. In our study, the most frequent form of RV dysfunction was pseudonormal filling which was most prevalent in group C patients. Thus, we hypothesise that during intermediate follow-up period, the most frequent type of RV diastolic dysfunction is pseudonormal filling.
Comparison of RV Diastolic Function Group-Wise
There was an increase in the number of patients with RV diastolic dysfunction as the postoperative time since total correction increased as shown in Table 3. This can be explained by the fact that the process of endomyocardial fibrosis of RV intrinsic to TOF intensifies as the postoperative time increases. Also, the impact of cardioplegia and hypothermia on the RV myocardium increases over time. 5
Impact of Degree of Pulmonary Regurgitation on RV Diastolic Function
It was seen that the number of patients with RV diastolic dysfunction was more in patients with severe PR (50%) as compared to those with mild-to-moderate PR (34%) (Table 2). In a study done by Norgård et al, 9 95 patients were studied for 4.3 years after repair. RV diastolic dysfunction in the form of restrictive RV physiology was more common in patients with TAP repair compared with non-TAP repair (P <.05). As most patients with TAP have severe PR, it is seen that RV diastolic dysfunction is more prevalent in those patients who have severe PR. This is seen because the presence of severe PR causes increased RV end diastolic volume which over a period of time stiffens (noncompliant) the already hypertrophied RV and ultimately leads to diastolic dysfunction. 10
Limitations
This is a single-center study and surgical techniques may differ from center to center which may impact postoperative RV function. Also, a larger sample size could have been used to increase the statistical significance of the study.
Conclusion
Subclinical RV diastolic dysfunction is present in almost half of the postoperative TOF patients of pediatric age group. Severe PR and time since total correction negatively impact RV diastolic function. The most prevalent form of diastolic dysfunction during intermediate follow-up period (average of 10 years post total correction) was pseudonormal filling in our study. Further follow-up of such patients need to be done to see whether they develop restrictive RV physiology later on.
What Is Already Known
Restrictive RV physiology is the predominant form of RV diastolic dysfunction seen in the immediate postoperative period and in long-term follow-up in TOF patients.
What This Study Adds
Pseudonormal filling pattern is the most common type of RV diastolic dysfunction seen in postoperative Tetralogy of Fallot patients in the intermediate follow-up period.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.