
Abstract
Renal-artery stenosis/occlusion is the cause of ischemic nephropathy, which is associated with hypertension due to renovascular system involvement. Acute renal failure in patients with bilateral renal artery stenosis can occur for a variety of reasons, including administration of an angiotensin-converting enzyme inhibitor or spontaneous progression of renal-artery stenosis leading to bilateral total occlusion or high-grade stenosis. Rapid diagnosis and prompt treatment are the basis of kidney survival. The root cause of renal-artery occlusion must be elucidated in younger age patients after revascularization, such as Takayasu’s arteritis (TA) or fibromuscular dysplasia. We discuss the case of a preadolescent girl who had bilateral complete renal artery occlusion due to TA and acute kidney injury, needing renal replacement therapy. She had a bailout percutaneous renal intervention to the left renal artery, which resulted in remarkable clinical improvement.
Keywords
Introduction
Takayasu’s arteritis (TA) is a nonspecific vasculitis that mostly affects the aorta and its major branches. It is a not uncommon condition in Asia, with a relatively high prevalence in southeast countries. Takayasu’s arteritis-induced renal artery stenosis (TARAS) is the second-most common cause of all renal artery stenosis. This can lead to high blood pressure (BP), renal failure, heart disease, stroke, and premature death. 1
Patients with renal artery stenosis/occlusion should be examined for systemic vasculitis because only anti-inflammatory therapy can prevent or minimize additional vasculitis consequences. 2 To treat symptomatic TARAS, revascularization, including surgical and endovascular techniques, is employed, with percutaneous transluminal renal angioplasty (PTRA) being the most often used intervention. We describe a case of bilateral renal artery stenosis that was determined to be the etiology of anuria in a juvenile child with a lifesaving outcome after early unilateral renal artery revascularization.
Case Report
A 10-year-old girl child presented with complaints of sudden onset severe breathlessness with anuria. Vital parameters recorded sinus tachycardia (heart rate—132/min), BP in upper limbs was 210/130 mmHg (>99th percentile) with palpable peripheral pulses, and tachypnoea (respiratory rate—34/min). Echocardiography revealed normal left ventricular function with moderate concentric left ventricular hypertrophy. Laboratory parameters revealed leukocytosis with lymphocytic predominance and serum creatinine was 8.3 mg%. Arterial blood gas analysis showed metabolic acidosis with type I respiratory failure. The patient was ventilated and started on intravenous antihypertensive medications. Renal replacement therapy was started in the form of hemodialysis to correct the metabolic abnormalities.
Acute phase reactants like erythrocyte sedimentation rate and C-reactive proteins were elevated and had high plasma renin activity. Ultrasound abdomen suggested increased corticomedullary echotexture with the partially preserved subsegmental flow. Urinary tract obstruction was excluded from ultrasonography and the diagnosis of acute glomerulonephritis was unlikely due to normal urine sediment.
Computed tomography angiography of the abdominal aorta demonstrated the occlusions of bilateral renal arteries with mild stenosis of the suprarenal abdominal aorta (Figure 1A-C). Under the guidance of a nephrologist, a limited quantity of weight-adjusted dose of iso-osmolar contrast was employed in conjunction with an appropriate hydration protocol. Based on the findings, the patient was diagnosed with renovascular hypertension with acute kidney injury related to TA and bilateral renal artery occlusion. Furthermore, the thoracoabdominal aorta has been revealed to exhibit features of the middle aortic syndrome, with mild discrete stenosis of the suprarenal aorta and a measured gradient of 10 mm Hg.
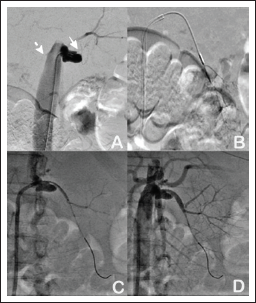
Selective renal angiography of the right renal artery showed ostioproximal flush total occlusion. The left renal artery had a juxtaostial aneurysmal dilatation followed by total occlusion (Figure 2A; Video 1). PTRA using the Gaia-2 guidewire with the support of the microcatheter proved successful after previous attempts with hydrophilic guide wires failed. Contrast injection through the microcatheter confirmed the true lumen (Figure 2B, Video 2). The occluded segment was serially predilated using 1.5 × 10 mm, 2.0 x 10 mm balloons. A 2.5 x 15 mm Resolute Onyx drug-eluting stent (Medtronic Inc) was deployed across the aneurysm to the ostioproximal segment as per the angiographic diameter of the vessel (Figure 2C; Video 3). The ostial segment of the stent was flared using a 2.5 x 12 mm noncompliant balloon at 18 atm. Angiography revealed restoration of brisk flow to the left kidney (Figure 2D; Video 4). The “confienza pro 12” guidewire failed despite the use of a microcatheter due to the hard fibrotic nature of the ostial flush occlusion, which did not give enough support to the guide catheter.
Computed tomography angiography of the thoracoabdominal aorta in maximum intensity projection (MIP) in anteroposterior view (Panel A) and 3D reconstructed volume-rendered images (noncolored, Panel B; colored, Panel C) showed the occlusion of both the renal arteries (dashed arrow—right renal artery; solid arrow—left renal artery). It reveals tapered stenosis of the suprarenal aorta giving a “Rat-tail appearance.” This is also called “Middle aortic syndrome” (Vertical dashed line, Panel C).

Percutaneous trans-luminal renal angioplasty with chronic complete occlusion with left renal artery adjacent to small ostial aneurysm (solid white arrow, Panel A). It also reveals the ostial flush of the right renal artery (Dashed white arrow). Gaia-2 guidewire with help of the microcatheter was able to cross the occlusion and injection through the microcatheter demonstrating the distal renal vasculature that confirmed the true lumen (Panel B). The drug-eluting stent was deployed after predilatation across the occluded ostioproximal segment of the left renal artery (Panel C). Final angiography revealed a brisk flow to the left renal artery and its distal segmental branches (Panel D).
Urine flow started the next day and serum creatinine dropped to 4.3 mg%. Renal replacement therapy stopped after 1 week as the baseline serum creatinine was 2.2 mg%. The patient was discharged on the 12th-day postprocedure requiring 2 antihypertensive drugs (amlodipine and clonidine) and dual antiplatelet therapy (aspirin and clopidogrel).
The patient had a 12-months follow-up with normal vital parameters and renal parameters with adequate urine output. A patent left renal artery stent with a normal flow pattern was found using abdominal duplex ultrasonography and renal Doppler. We began medical treatment to control disease activity and made plans for a kidney transplant and aortic procedure in the future.
Discussion
TA is a granulomatous inflammation of unknown etiological conditions, which leads to stenosis and occlusion of large arteries. TA affects young patients and demonstrates recurrence and advancement across their lives. 3 The diagnosis of TA was performed based on the 1990 American College of Rheumatology guidelines and was thus assessed by the presence of age <40 years, the disparity in BP >10 mmHg between the limbs, aortic murmur, and modification of the arteriogram. 4
TA primarily affects women from 10 to 40 years of age (90 % of cases). In addition to being associated with other causes, such as infectious agents and genetic predisposition, its pathogenesis is not yet fully known and is currently thought to be the result of chronic autoimmune inflammation of large arteries. A 2-stage process has been described, with a “pre-pulseless” period characterized by nonspecific inflammatory abnormalities, succeeded by a chronic phase with the establishment of vascular insufficiency, in some cases supplemented by periodic flares, albeit this trend does not apply to all individuals. 5
Chen et al 6 studied 411 patients diagnosed with TA in their center retrospectively to investigate the clinical features affecting the renal arteries. 6 The prevalence of renal artery involvement in TA patients ranges from 11.5% to 62% and tends to be strongly related to ethnicity.6, 7 Renal artery stenosis and occlusion account for 75% to 85% and 13% to 20%, respectively. An aneurysm of the renal artery, as found in our case, accounts for just 5% to 8% of renal artery involvement. The onset of the disease in patients with TARAS was at a younger age and had hypertension in 74.6% of patients. Both congestive heart failure (22.4 %) and pulmonary hypertension (20%) were slightly more common in patients with TARAS.
Zhao et al 8 identified PTRA with a technical success rate of 93.9% in a meta-analysis that comprised 17 noncontrolled observational studies including 384 patients with renovascular hypertension of varied etiologies. The BP improvement rate was 68.4%, with 25.5% of patients requiring a repeat procedure because of lesion restenosis. 8 Zhu et al 9 reported comparable PTRA findings utilizing balloon dilatation, with restenosis observed in 40.9% of patients after an average interval of 11.8 months. 9 Both the above studies did not recommend the use of stents with a high risk of restenosis of 25% to 40%.
When PTA alone failed to cure TARAS, selective stenting reduced BP. Selective stenting was used when PTA alone was ineffective in treating TARAS. Primary patency rates were 75.6% with traditional bare-metal stent implantation, but occlusion rates were greater, and the likelihood of repeat intervention was higher. 1 As a result, we decided to employ a drug-eluting stent in our case, despite the fact that there is no large evidence on its usage in TARAS patients.
For percutaneous renal artery recanalization, there is relatively little clinical evidence for its scientific feasibility and therapeutic effect, with just a few case reports and series indicating positive outcomes in the pediatric age range. 10 Vijayvergiya et al 11 reported 6 cases of renovascular hypertension in children who underwent complex aortorenal intervention. The mean age of the patient was 10.6 ± 2.5 years. Six children with TA had successfully treated the abdominal aorta and its main branches with complex percutaneous interventions including PTRA. Balloon dilatation and stent placement are the cornerstones of TA management with large vessel stenosis.
Yang et al 12 retrospectively studied 15 consecutive patients with chronic occlusion of the renal artery who had successful PTRA/stenting only for unilateral recurrent occlusion of the renal artery. The restenosis incidence was 20% at a median follow-up of 1.5 years. Renal function increased or remained unchanged in 26.7% and 53.3% of patients, respectively, and reduced or increased BP in 13.3% and 40.0% of patients, respectively. Young patients with TA have been shown to benefit most from revascularization as in our case. 12
Petrov et al 10 studied 7 hypertension individuals aged 15 or older who were on 3 antihypertensive drugs. Similar to our situation, they had an obstructed renal artery with partly sustained subsegmental flow. A year later, clinical and duplex ultrasonography showed 85.7% procedural success. All successful revascularization patients had reduced BP. All patients had normal renin levels at 6 months and 1 year after the intervention.
Recanalizing complete renal artery occlusions are feasible and have a beneficial impact on lowering the level of plasma renin and regulation of BP. This technique should only be extended to a small group of resistant hypertension patients and evidence of retained subsegmental flow. The utilization of a Gaia-2 guidewire and a Resolute Onyx drug-eluting stent was the highlight of our case. Because the artery enlarges (positive remodeling) after the PTRA, this current generation coronary stent platform may be post-dilated up to 3.5 mm in diameter in the near future, if needed. As a result, bigger multicenter studies are needed to identify the precise indications and results before bringing this strategy to ordinary clinical practice.
However, this intervention may not have long-term benefits, although it does play a role in lowering hypertensive crises related to renal artery occlusion.
Conclusion
Renal artery involvement is a common symptom of TA in Indian patients. The prevalence of hypertension, cardiac, and renal dysfunction is higher in patients with renal artery involvement, implying that the condition may progress to a more serious and complicated form. We have also found a correlation between renal dysfunction and the severity of renal artery stenosis. Our case report indicates early intervention for occluded renal arteries can be helpful to avoid permanent damage to the kidney.
Supplemental Material
Below mentioned supplemental material for this article is available online.
Supplemental Material, sj-vid-1-occ-10.1177_26324636221079442 for Bail-Out Percutaneous Intervention for Chronic Total Occlusion of the Left Renal Artery Secondary to Takayasu’s Arteritis in a Pediatric Patient Using Drug-Eluting Stent by Pankaj Jariwala, Kartik Jadhav, Dilip Babu Madhawar and Suresh Giragani, in Indian Journal of Clinical Cardiology
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.