
Abstract
Background:
Inflammatory biomarkers are associated with adverse cardiovascular events during ST-elevation acute myocardial infarction (STEMI). We aimed to investigate the role of inflammatory biomarkers, high-sensitivity C-reactive protein (hs-CRP), and soluble ST-2 (sST2), for prediction of adverse cardiovascular events in STEMI.
Methods:
This was a prospective cohort study that consecutively enrolled patients with STEMI. Subjects were observed during hospitalization until discharge or fatal events happened. Adverse cardiovascular event was a compilation of cardiac mortality, acute heart failure, cardiogenic shock, reinfarction, and malignant ventricular arrhythmia. Blood samples were withdrawn on admission and inflammatory biomarkers (hs-CRP and sST2) were measured. The receiver operator characteristics curve and multivariable analysis were performed to determine which inflammatory biomarkers predict in-hospital adverse cardiovascular events and mortality.
Result:
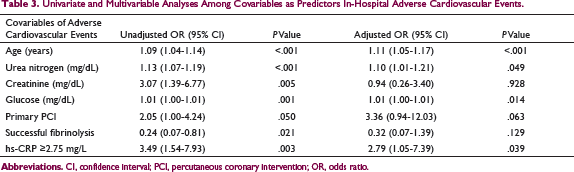
Of 166 subjects, the in-hospital adverse cardiovascular events occurred in 41 subjects (24.6%) and mortality occurred in 16 subjects (9.6%). Subjects with in-hospital adverse cardiovascular events and mortality had a significantly higher hs-CRP level, but comparable sST2 level than subjects without events. The hs-CRP level was the most precise biomarkers to predict in-hospital adverse cardiovascular events (hs-CRP cut-off ≥2.75 mg/L) and mortality (hs-CRP cut-off ≥7 mg/L). Multivariable analysis indicated hs-CRP ≥2.75 mg/L as an independent predictor for in-hospital adverse cardiovascular events (adjusted odds ratio [OR]: 2.79, 95% confidence interval [CI]: 1.05-7.39, P = .039) and hs-CRP ≥7 mg/L for mortality (adjusted OR: 5.45, 95% CI: 1.13-26.18, P = .034) in STEMI.
Conclusion:
On admission, hs-CRP level independently predicted in-hospital adverse cardiovascular events, at cut-off level ≥2.75 mg/L, and mortality, at cut-off level ≥7 mg/L, in STEMI patients.
Introduction
Ischemic heart disease (IHD) becomes a major mortality origin worldwide. The majority of IHD had fatality during episodes of ST-elevation acute myocardial infarction (STEMI). STEMI is one spectrum of IHD, which still has high mortality burden despite its improvement in therapeutic modalities. The predictors for in-hospital major adverse cardiovascular events in STEMI have been extensively studied, which led to the generation of risk prediction score and the development of treatment algorithm as earlier as possible. Several prediction scores have been constructed to predict in-hospital major adverse cardiovascular and mortality after STEMI. 1 Nevertheless, the inclusion of biomarkers in these prediction scores has not been well recommended despite many biomarkers have been evaluated in connection to a higher sudden death risk, reinfarction, and heart failure during STEMI episode.
Several studies have shown a correlation between increased inflammatory biomarker level with adverse cardiovascular outcomes in STEMI. Serum high-sensitivity C-reactive protein (hs-CRP) level had been proven to elevate the risk of major adverse cardiovascular events in acute myocardial infarction (AMI), both in hospitals and during longstanding observation.2, 3 Serum soluble suppression of tumorigenesis-2 (sST2), a member of an interleukin (IL)-1 receptor family, is an inflammatory biomarker which increased during AMI episode and is associated with adverse outcomes.4, 5 The acute inflammation changes, represented by increasing release of hs-CRP and sST2 in the circulation, reduce the cardiac function and homeostasis during AMI episodes which lead to the deterioration of clinical stability. In STEMI, the adverse cardiovascular outcomes commonly occur in the hospital during the acute phase, whereas in non-STEMI the long-term effect is much more prominent.
The inflammatory biomarkers have the discriminatory value to predict patients with adverse cardiovascular events in STEMI. Nevertheless, the determination of which inflammatory biomarkers showed consistency as a prognostic indicator in STEMI needs to be elucidated. Therefore, this study designs to compare and weigh the performance of 2 inflammatory biomarkers, namely hs-CRP and sST2, measured on admission to predict the in-hospital main adverse cardiovascular events and mortality among STEMI patients.
Materials and Methods
The research design was a prospective cohort study. We consecutively enrolled patients with STEMI, who were admitted to the emergency unit and treated at the intensive cardiac care unit (ICCU) of our hospital from 2014 to 2016. The subjects were observed from admission, during in-hospital intensive cardiac care at ICCU until discharge. The outcome was the adverse cardiovascular events and death occurring during in-hospital intensive cardiac care. The exposure of this study was the excess of inflammation, reflected by increased level of inflammatory biomarkers, namely hs-CRP and sST2, on admission.
The subjects of this research fulfilled the inclusion criteria: (a) the diagnosis of STEMI, (b) the age from 35 to 75 years old, (c) the beginning of anginal pain ≤24 h, and (d) the patients without prior fibrinolytic or anticoagulants. The exclusion criteria were: (a) the patients with NYHA class >II chronic heart failure, stage >III chronic kidney disease, and hepatic cirrhosis, (b) the patient with a history of malignancy, (c) the concomitant acute infection and sepsis, (d) the concomitant acute stroke, and (e) the patient with a history of chronic inflammatory diseases (chronic arthritis, colitis, or autoimmune diseases). All subjects or their relatives agreed to participate in the research and retained an informed consent form. The protocol had been accepted by the ethics committee of our institution (No: KE/FK/719/EC).
The diagnosis of STEMI was verified based on a national guideline. 6 The initial managements during emergency stage were at the discretion of attending cardiologists. After stabilizing at emergency stage, the subjects were transported to ICCU for intensive managements. The observation of subjects was performed in ICCU until discharged from ICCU or fatal event/mortality. The adverse cardiovascular event was a compilation of cardiac mortality, acute heart failure, cardiogenic shock, reinfarction, and ventricular tachycardia/ventricular fibrillation (VT/VF). Cardiac mortality was cardiac-induced death. Acute heart failure was the clinical symptoms and signs of congestion and the use of intravenous diuretics. Cardiogenic shock was a systolic blood pressure <90 mmHg with symptoms and signs of low perfusion and the use of inotropics or/and vasopressor drugs. Reinfarction was newly developed continuous anginal pain, resumed ST-elevation, and elevated hs-troponin I in formerly unchanging patients. Resuscitated VT/VF was the reoccurrence of spontaneous circulation after cardiopulmonary resuscitation and defibrillation. These major adverse cardiovascular events were recorded as previously published. 5
For laboratory examination, the blood samples from antecubital veins were withdrawn on admission while subjects were in a supine position. Blood samples were collected before performing fibrinolysis or primary percutaneous coronary intervention (PCI). The blood cell counts were conducted by hemocytometer reading. Cardiac enzymes were measured as a routine procedure, that is, troponin I by enzyme-linked fluorescent assay method with MINI VIDAS (Biomerieux). An aliquot of serum was separated from blood samples and preserved at −80°C freezer pending further analysis for hs-CRP and sST2 examination. The hs-CRP level was determined with the immunoturbidimetric method. The Roche Cobas c501 (Roche Diagnostic) analyzer was used to measure hs-CRP level. The sST2 level was measured by ELISA methods using Quantikine Human ST2/IL-1 R4Kit (R&D Systems) and read in plate reader according to manufacturer instruction.
The onset was the duration calculated from the beginnings of chest pain/anginal pain until the patient got diagnosed with STEMI in our hospital. Thereby, the time of hs-CRP and sST2 measurement from the start of STEMI can be assumed from the onset data.
For statistical analysis, the subjects were partitioned into 2 groups according to the occurrence of in-hospital adverse cardiovascular events and in-hospital mortality. The comparison between continuous data was statistically analyzed with the Student T-test (normal-distributed data) or Mann-Whitney test (non-normal-distributed data) and between categorical data was analyzed with chi-square test or Fisher exact test, where applicable. Normality analysis for continuous data was conducted with the Kolmogorov-Smirnov test and logarithmic transformation was conducted if needed. The receiver operator characteristics (ROC) curve was designed to compare the accuracy of hs-CRP level and sST2 level to predict the episode of in-hospital adverse cardiovascular events and in-hospital mortality, as well as to clarify the cut-off value. The univariate and multivariable analyses, by logistic regression test, were completed to clarify the predictors for in-hospital adverse cardiovascular events and in-hospital mortality among covariables. A statistically significance was established at a P value <.05.
Result
The Comparison of Variables Between Subjects With In-Hospital Adverse Cardiovascular Events (n = 41) and Subjects Without In-Hospital Adverse Cardiovascular Events (n = 125).
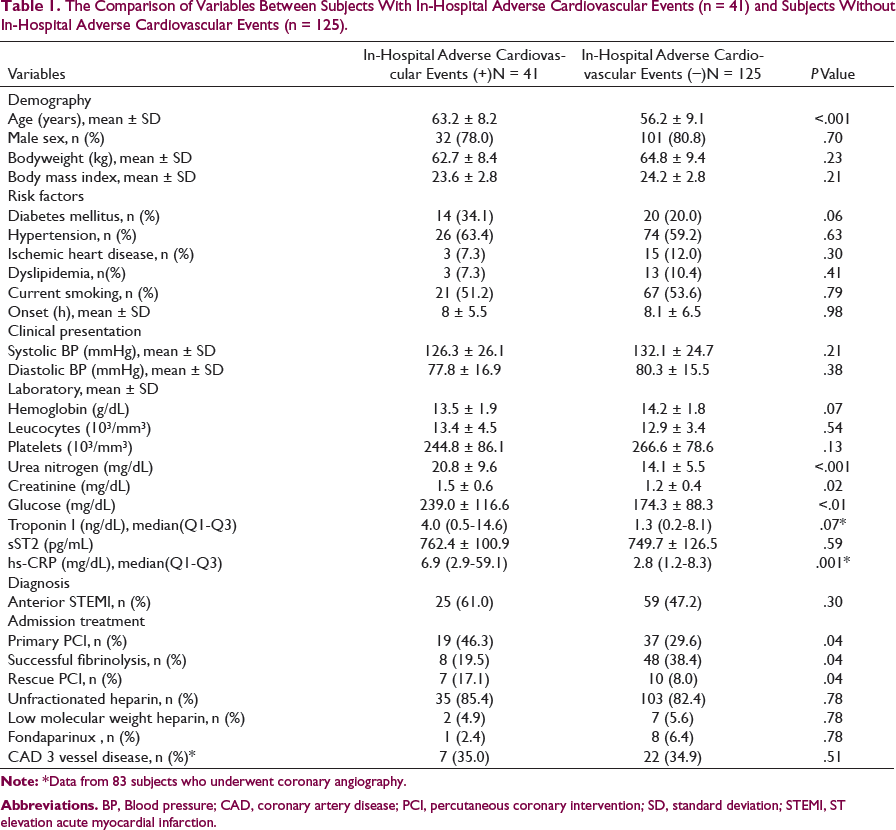
Abbreviations. BP, Blood pressure; CAD, coronary artery disease; PCI, percutaneous coronary intervention; SD, standard deviation; STEMI, ST elevation acute myocardial infarction.
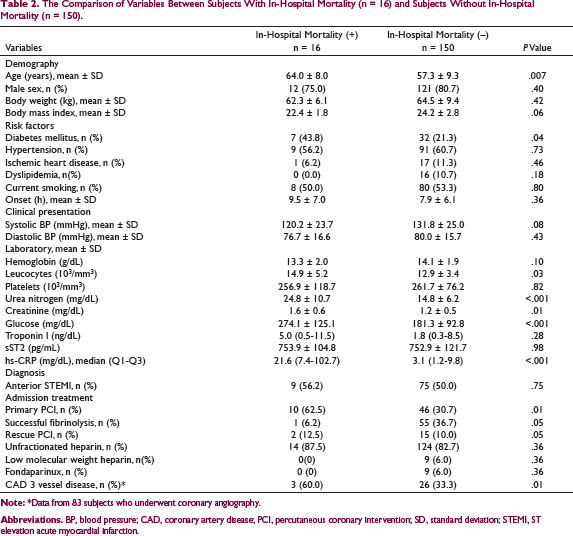
The Comparison of Variables Between Subjects With In-Hospital Mortality (n = 16) and Subjects Without In-Hospital Mortality (n = 150).
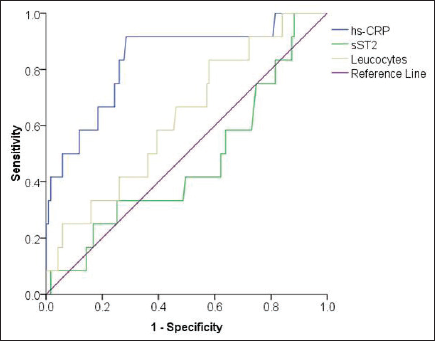
The ROC curve indicated that hs-CRP level had higher area under the curve (AUC = 0.677, 95% confidence interval [CI]: 0.573-0.780, P = .02) as compared with other inflammatory biomarkers namely sST2 (AUC = 0.501, 95% CI: 0.393-0.609, P = .98) and leucocyte count (AUC = 0.470, 95% CI: 0.355-0.585, P = 0.60) to precisely predict in-hospital adverse cardiovascular events (Figure 1). Based on this ROC curve, the hs-CRP cut-off point to predict in-hospital adverse cardiovascular events was determined at level ≥2.75 mg/L (sensitivity 78%, specificity 49.6%).
The ROC Curve for Accuracy of hs-CRP Level (AUC 0.677, 95% CI: 0.573-0.780, P = .02), sST2 Level (AUC 0.501, 95% CI: 0.393-0.609, P = .98), and Leucocyte Count (AUC = 0.470, 95% CI: 0.355-0.585, P = .60) to Predict In-Hospital Adverse Cardiac Events.
Univariate and Multivariable Analyses Among Covariables as Predictors In-Hospital Adverse Cardiovascular Events.
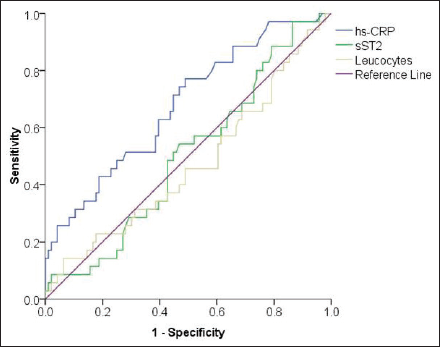
The ROC curve indicated that hs-CRP level had highest area under the curve (AUC = 0.835, 95% CI: 0.705-0.965, P < .01) as compared with other inflammatory biomarkers namely sST2 (AUC = 0.468, 95% CI: 0.292-0.644, P = .717) and leucocyte counts (AUC = 0.629, 95% CI: 0.470-0.788, P = .141) to accurately predict in-hospital mortality (Figure 2). Based on this ROC curve, the hs-CRP cut-off point to predict in-hospital mortality was determined at level ≥7 mg/L (sensitivity 81%, specificity 71.3%).
The ROC Curve for Accuracy of hs-CRP Level (AUC 0.835, 95% CI: 0.705-0.965, P < .01), sST2 Level (AUC 0.468, 95% CI: 0.292-0.644, P = .717), and Leucocyte Count (AUC 0.629, 95% CI: 0.470-0.788, P = .141) to Predict In-Hospital Mortality.
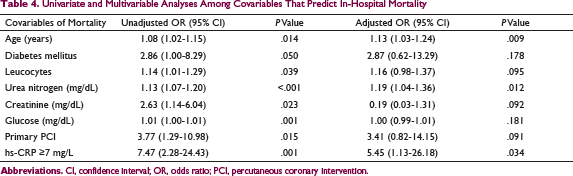
Univariate and Multivariable Analyses Among Covariables That Predict In-Hospital Mortality
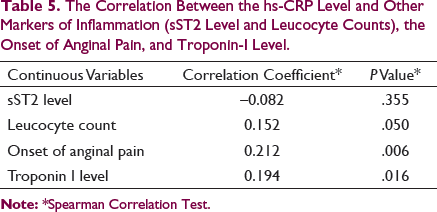
The Correlation Between the hs-CRP Level and Other Markers of Inflammation (sST2 Level and Leucocyte Counts), the Onset of Anginal Pain, and Troponin-I Level.
Discussion
Our study finding confirmed that among inflammatory biomarkers assessed, higher hs-CRP level, measured on admission, was an independent predictor of in-hospital adverse cardiovascular events and mortality among patients with STEMI. Our study did not confirm the discriminative value of sST2 level, measured on admission, in the prediction of in-hospital adverse cardiovascular events and mortality among patients with STEMI. Selected inflammatory biomarkers should be prudently chosen as potential biomarkers in inclusion for risk prediction score for STEMI. In this study, on-admission hs-CRP level ≥2.75 mg/L independently predicted an almost 3-fold increase in adverse cardiovascular events during the acute phase, and hs-CRP level ≥7 mg/L independently predicted in-hospital mortality.
Several studies have shown a correlation between increased serum hs-CRP level and an increased risk of cardiovascular adverse events STEMI. The relationship between hs-CRP levels and cardiovascular adverse events during STEMI is associated with the no-reflow phenomenon, excess inflammation response of myocardial injury, and ongoing prothrombotic state. 7 This is because they induce activation of the complement system thereby increasing the inflammatory response and formation of the occlusive thrombus in coronary arteries.7, 8 Furthermore, serum hs-CRP level exponentially increases and reaches a peak at 72 h after STEMI onset, at which time is a manifestation of the grave reaction of injurious tissue. 9 Our study examined the level of hs-CRP on admission, which reflects the early tissue injury due to coronary insufficiency.
Acute phase hs-CRP, measured after 24 h of onset but not on admission, predicted the risk of long-term left ventricle systolic dysfunction and heart failure in STEMI patients. 10 In STEMI, both treated invasively or by fibrinolytic, the hs-CRP levels at appearance denote an independent predictor for fatal and nonfatal cardiovascular events throughout short- and long-term follow-up.2, 3, 11 The cut-off value of hs-CRP to predict adverse cardiovascular outcome in STEMI was varied. There is a need to confirm the cut-off value of hs-CRP which has a prognostic value for predicting the worst outcome. Our study provided this cut-off value for both nonfatal and fatal short-term cardiovascular events.
A higher hs-CRP level predicts the more severe form of coronary artery disease among patients with STEMI. 12 The predictive value of the hs-CRP level encompassed the whole spectrum of acute coronary syndrome, which is indicative that hs-CRP is ubiquitous as a response to acute cardiac injury and inflammation. The higher hs-CRP level reflects an intracardiac inflammatory response due to acute myocardial cell injury and death. 13 Patients with STEMI and increased hs-CRP represent an exaggerated and hyperresponsiveness of the inflammatory system, acute-phase reaction, and immune system overactivation, which facilitate myocardial damage and cardiac dysfunction. 13 Based on the body amount of evidence, the hs-CRP level should be incorporated into the risk prediction score in STEMI. The only challenge is the rapidity of the assay to get the hs-CRP level result timely, before the decision-making in the management of STEMI, in which the faster myocardial salvage the better.
Our previous study indicated that on admission, sST2 level is linked with adverse outcomes in patients with STEMI. 5 During acute inflammation, sST2 is a marker of acute inflammation because it can be produced by leucocytes, endothelial cells, and immune cells. 14 In addition to acute inflammation, sST2 is released by myocardia as a biomarker of myocardial strain and fibrosis. 15 In circulation, sST2 can present as a freely soluble form or bound form with IL-33, a proinflammatory IL-1 family cytokines. Both sST2 and IL-33 are increased in the acute inflammatory state including STEMI. In this study, we used the ELISA kit which detects both free-form sST2 and IL-33-bound sST2. Unlike our previous study using a point-of-care test, 5 we cannot detect sST2 level differences between subjects with adverse cardiac events and those without.
Our study had several limitations which should be mentioned, (a) the sample size should be increased to be able to increase to power of the study, (b) the inclusion of established risk prediction scores should be incorporated in the analysis, (c) the other conditions that influence the rise of hs-CRP other than stated in the exclusion criteria of this study need to be broadened, (d) the serial measurement of hs-CRP during STEMI episode will produce a more accurate result on the pathophysiological process, and (e) the inclusion of all spectra of acute coronary syndromes, (STEMI, non-STEMI, and unstable angina), should be considered to elucidate the inflammatory biomarkers prediction role in all spectra of disease.
Conclusion
In conclusion, a higher hs-CRP level on admission was an independent predictor for in-hospital adverse cardiovascular events and mortality in patients with STEMI. The hs-CRP cut-off level for predicting adverse cardiovascular events was ≥2.75 mg/L and for mortality was ≥7 mg/L. The sST2 did not influence the in-hospital adverse cardiovascular events and mortality among patients with STEMI.
Footnotes
Acknowledgements
The authors would like to thank Mr Farid Abdullah from the Department of Clinical Pathology and Laboratory Medicine Faculty of Medicine, Public Health and Nursing Universitas Gadjah Mada, Yogyakarta for his technical assistance on blood sample handling and ELISA analysis. Authors also thank Laboratorium Klinik Pramita, Yogyakarta for its assistance on performing hs-CRP measurement.
Author Contributions
Conceptualization: ABH and IP; methodology: ABH, IS, MPI, TR, and SGVH; formal analysis: ABH, IS, MPI, TR, and SGVH; investigation: ABH, IS, and IP; writing original draft preparation: ABH; writing review and editing: ABH, IS, MPI, TR, SGVH, RR, IP; funding acquisition: ABH. All authors have read and agreed to the published version of the manuscript. All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Dana Masyarakat Faculty of Medicine, Public Health and Nursing Universitas Gadjah Mada, Yogyakarta, Indonesia Fiscal Year 2014 and 2015 to Principal Investigator (ABH).