
Abstract
The present case is unique and the first to describe the spiral nature of dissection in spontaneous coronary artery dissection in a young female which has not yet been described in the world literature.
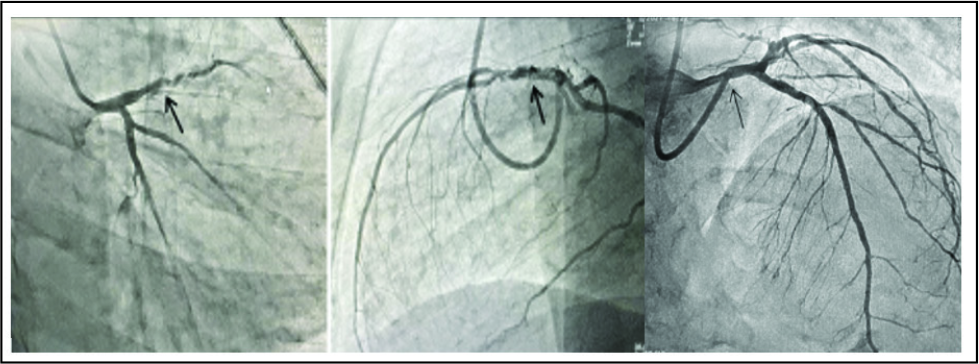
Although spontaneous coronary artery dissection (SCAD) is a well-known cause of myocardial infarction in young females, spiral spontaneous dissection of the coronary artery has not been described in the literature so far. We present a 34-year young female with 1 sibling of 8 years of age with retrosternal chest discomfort, diaphoresis, and shortness of breath for the last 2 h. She was nondiabetic, nonhypertensive, normolipidemic, without any family history of coronary artery disease. Electrocardiogram revealed acute anterior wall ST-elevation myocardial infarction (STEMI) and echocardiography revealed regional wall motion abnormality in left anterior descending (LAD) coronary artery territory with mild left ventricular systolic dysfunction (EF-40%). She was COVID-19 negative. She was subjected to primary percutaneous intervention and right transradial coronary angiogram revealed long segment spiral dissection of LAD beginning from the osteoproximal to the distal segment (Figure 1). The lesion was revascularized with a drug-eluting stent (2.75 × 34 mm) at 14 atm pressure with postprocedure TIMI III flow. Technical challenges during the percutaneous transluminal coronary intervention of a spiral coronary artery dissection include avoiding deep engagement of the guide catheter due to the fragile nature of the coronary artery, gentle contrast injection to prevent dissection propagation, and wiring the true lumen as an inadvertent entry of the wire into the false lumen extends the dissection with side branch occlusion. 1 Based on intracoronary imaging, Saw et al 2 classified SCAD into the following 3 types:
RAO 30 View, Lateral View Showing Spiral Dissection and Postrevascularization Status.
Type 1: Double-lumen appearance with a longitudinal filling defect.
Type 2: Long tubular lesion >;30 mm with intramural hematoma.
Type 3: Multiple tubular lesions with intramural hematoma.
The present case does not fit into any of the morphologic types of SCAD as double lumen, tubular, or multiple tubular and is unique and the first to describe the spiral nature of dissection in SCAD which has not yet been described in the world literature.