
Abstract
One-third of all deaths globally are caused by cardiovascular disease (CVD), and this percentage is predicted to climb as CVD risk factors become more widespread. Primary prevention of risk factors is the most fundamental duty in dealing with the CVD epidemic. The link between atherogenic index of plasma (AIP) and other CVD risks among university workers was investigated among study participants in order to demonstrate that AIP, not lipid profile, is a better predictor of CVDs. They discovered a link between AIP and CVD risk variables (body mass index, visceral fat, body fat, total cholesterol, low density lipoprotein cholesterol, triglyceride, glucose, and high density lipoprotein cholesterol) in people with type 2 diabetes. This comparative study was carried out in Cardiology Department, Zagazig University Hospitals. This study included 140 type 2 diabetes mellitus patients. They were classified into 2 main groups:
Group 1: 70 patients with type 2 diabetes who had coronary artery disease (CAD).
Group (2): 70 type 2 diabetes individuals with no indicators of CAD (admitted complaining of symptoms of angina or CA showing no significant stenotic lesions).
Regarding study explained it has showed that AIP outperforms standard lipid indicators in predicting the likelihood ofdeveloping CADs in people with type 2 diabetes. In addition, the value of AIP in diabetic and prediabetic patients for predicting future CVD is being investigated. They came to the conclusion that AIP is an excellent predictor of future CVD in those with diabetes and those who are prediabetic.
Introduction
Cardiovascular disease (CVD) is a major public health concern around the world. Diabetic people have a two- to fourfold increased risk of developing coronary artery disease (CAD) and myocardial infarction (MI), proving that type 2 diabetes is an unique risk factor for stroke and heart disease. 1
In the past, CAD was thought to be a simple inexorable process of artery narrowing, eventually resulting in complete vessel blockage; however, in recent years, the explanatory paradigm has changed because it was realized that a wide range of diseases can result from atheromatous changes in coronary vessels varying from coronary plaques stable (lipid-poor) to unstable (lipid-rich). 2
Diabetes mellitus (DM) and CAD are closely related where DM is an important risk factor for CAD, and even is also considered as equivalent to established CAD. 3
The term “coronary risk equivalence” has recently been applied to type 2 diabetes. Diabetic dyslipidemia is an issue with lipoprotein metabolism in type 2 diabetics. Dyslipidemia plays a substantial influence in cardiovascular morbidity and mortality in diabetes individuals. Diabetes patients had higher triglyceride (TG) levels, lower high-density lipoprotein cholesterol (HDL-C), and similar serum readings for low-density lipoprotein cholesterol (LDL-C) than non-diabetics (LDL-C). Diabetes patients, on the other hand, have a greater proportion of smaller, denser LDL particles, which have been related to an increased risk of CAD. 4
DM is linked to a higher risk of developing atherosclerotic CAD early in life. In clinical trials, intensive glycemic management has often done nothing to improve cardiovascular outcomes. Diabetes causes dyslipidemia, and there is considerable evidence that decreasing cholesterol improves cardiovascular outcomes, even in people with seemingly normal lipid profiles. 5
Total cholesterol <5.2 mmol/L (200 mg/dL), LDL <3.4 mmol/L (130 mg/dL), HDL 0.9 mmol/L (35 mg/dL), or TGs <1.7 mmol/L (150 mg/dL), or a combination thereof, was defined as dyslipidemia according to the American Heart Association classification corresponding to the 95th percentile in an American population. 6
Atherogenic index of plasma (AIP), the logarithm of the molar ratio of TG to HDL-C, was first described by Dobiášová and Frohlichin. 7 AIP is based on 2 important parameters, serum TG, and serum HDLc. The concurrent use of TGs and HDLc in this ratio reflects the multiple interactions among the metabolism of different lipoproteins and can be useful for predicting plasma atherogenicity. 8
Based on the study by Dobiasova, suggested that AIP values of 0.10 to 0.24 are associated with low, and above 0.24 with high cardiovascular risk.
It is calculated according to the following formula:
AIP = Log (serum TG/serum HDLc) 7
AIP has a stronger sensitivity that reflects the interaction between atherogenic and protective lipoprotein. In recent years, a growing body of evidence has indicated that AIP is a strong marker to determine the risk of CAD. 7
Based on these data, the goal of this study is to see if AIP has any significance as a risk factor for CAD in type 2 diabetics (Table 1-7).
Patients and Methods
This comparative study was carried out in Cardiology Department, Zagazig University Hospital. It included 140 DM patients. Patients were selected from those who have type 2 DM. Subjects included in the study: patients having DM type 2 (non-insulin dependent DM), estimated by the glycemic variability, and free of complications, referred to coronary angiography in patients with a history of CAD due to chest pain. Coronary angiography was performed via the femoral or radial approach and assessed using Gensini score, which is the simplest way to assess severity of CAD.
Subjects excluded in the study: patients with any of the following were excluded: diabetic subjects with smoking, alcoholism, hypertension, liver disease, and kidney disease, patients who did not undergo coronary angiography, type 1 DM patients, patients with hypothyroidism or nephrotic syndrome, and patients taking lipid-lowering medications or antioxidants for more than 6 months.
We performed the following operations on each patient after receiving written informed consent:
A thorough medical history is taken, as well as a thorough clinical examination. Perform a 12-lead electrocardiogram as per usual procedure. Echocardiography: to assess left ventricular systolic and diastolic functions. Transthoracic echocardiography was done within 2 to 3 days of admission using a Phillips HD7 machine and VIVD 8 with a probe S4. LV Systolic function was assessed using Modified Simpson’s method. The American Society of Echocardiography’s recommendations for recording and calculating various parameters were followed.
9
Laboratory tests: Lipid profile (total cholesterol, LDL-C, HDL-C, triglycerides, and non-HDL-C), glycosylated hemoglobin (HbA1c) test, fasting, and 2-h postprandial blood glucose level and finally AIP calculation according this formula: log (TG/HDL-C).
10
Coronary angiography: Judkins conducted, without nitroglycerin using 6-French right and left heart catheters to assess condition of epicardial arteries and their lesions.
Results and Discussion
By careful attention and analysis of the patient data collected regarding diabetic patients with history of CADs and risk factor analysis to help compare AIP could be a good standpoint for prediction of CADs, the studied group were classified into two main groups:
Group (1): 70 type 2 DM patients with an evidence of CADs.
Risk Factors Distribution Between Studied Groups.
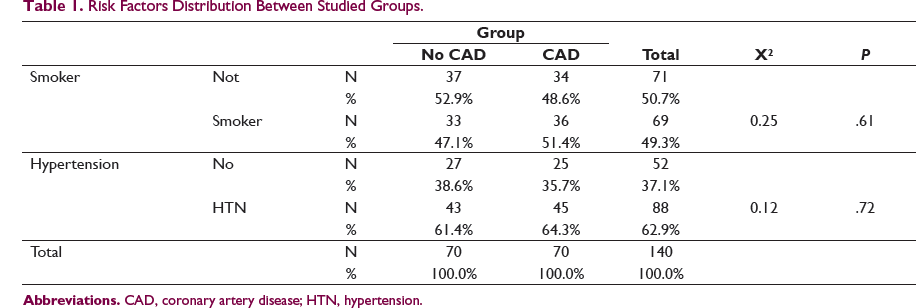
Regarding smoking in our study, 71 patients (50.7%) were non-smokers and 69 patients (49.3%) were smokers, with significant correlation between smoking and CAD. In agreement, cigarette smoking has been demonstrated to be significant factor in the developmental process of CVD (atherosclerosis, CAD, and peripheral vascular disorders) by alteration of plasma lipoprotein levels. 11 This study observed dyslipidemia and statistically raised atherogenic indices according to average cigarette sticks smoked per day. Our finding was further supported by the observation of a positive correlation of proatherogenic lipids and atherogenic indices with average cigarette sticks smoked per day.
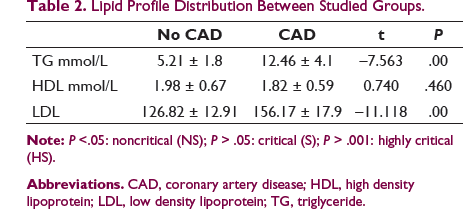
Lipid Profile Distribution Between Studied Groups.
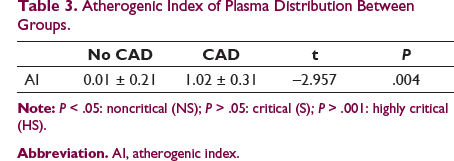
Atherogenic Index of Plasma Distribution Between Groups.
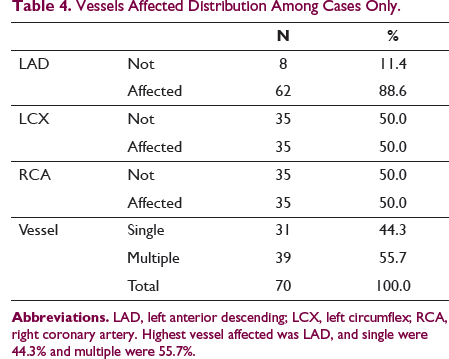
Vessels Affected Distribution Among Cases Only.
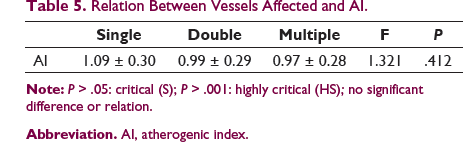
Relation Between Vessels Affected and AI.
HBA1c Values in Patients with CAD and Non CAD.

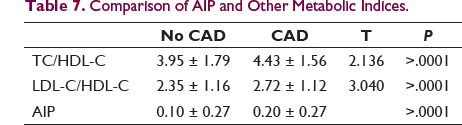
Comparison of AIP and Other Metabolic Indices.
Statins are considered the first line of treatment for lowering LDL-C levels, patients included in the study used statins, patients with had their statin dosage increased frequently 3 month after follow up to help achieve target LDL ,TG and HDL levels ,on the other hand regarding other subjects treated with statin had good control over dyslipidemia. The treatment of statin therapy for 6 months considerably lowered levels of LDL-C (by 29%) and TG (by 40%), but the rise in HDL-C (by 3%) was not significant. It worked reasonably well and was well tolerated. It resulted in a 50% reduction in AIP as a proxy of CV risk linked with mixed dyslipidemia and insulin resistance (relative to baseline in both groups).
Limitation
In this study, it was AIP that has been discovered to be a valuable method for diagnosing CAD in T2DM patients. Cultural differences, gender, diet, lifestyle, demographic parameters, laboratory testing, and metabolic condition, among other things, may impact AIP readings. The impact of nutraceuticals on lipid plasma levels is particularly noteworthy. Nutraceuticals are often not effective in reducing the burden of atherosclerosis, the development of coronary heart disease, fatality, and morbidity associated with CAD. Also, medications that are known to impact lipid metabolism should be avoided (lipid-lowering drugs, fish oil capsules, Beta-blockers, or diuretics) should be considered. We made a propensity score matching case-control study to make the data between the case-control group that can be compared and try our best to realize the integrity of data and eliminate the incomplete data in the process of data collection, and reflect objective as much facts as feasible. Dyslipidemia is a condition that affects many people in the diabetic patients specifically T2DM. Because their vulnerability to atherosclerosis and other cardiovascular problems is linked to their AIP, larger, community-based, and well-designed studies are needed to better understand the link between AIP and CVD risk in T2DM patients.
Conclusion
From these results, we found high-risk susceptibility to develop CVD and unstable angina with high level of AIP in type 2 diabetic subjects, compared to other patients with low level of AIP. So, AIP is an atherogenic factor to assess cardiovascular events. Therefore, AIP may be a good marker. Early intervention programs including exercise, food modification, and AIP assessment should be conducted on a regular basis to reduce the risk of CVD, specifically for individuals who are in the high-risk category.
Footnotes
Acknowledgments
The authors would like to express gratitude to the staff of employees of Cardiology Department, Faculty of Medicine, Zagazig University.
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.