
Abstract
Simultaneous ST-segment elevation (SST-SE) in anterior and inferior leads in the setting of ST-segment elevation myocardial infarction is often confounding for a cardiologist and further more challenging is the angiographic localization of the culprit vessel. SST-SE can be fatal as it jeopardizes simultaneously a larger area of myocardium. This phenomenon could be due to “one lesion, one artery,” “two lesions, one artery,” “two lesions, two arteries,” or combinations in two different coronary arteries. We have discussed an index case where we encountered a phenomenon of SST-SE and coronary angiography demonstrated “two lesions, one artery” (proximal occlusion and distal critical diffuse stenoses of the wrap-around left anterior descending [LAD] artery) and “two lesions, two (different coronary) arteries” (previously mentioned stenoses of the LAD artery and critical stenosis of the posterolateral branch of the right coronary arteries). We have also described in brief the possible causes of this phenomena and their electroangiographic correlation of the culprit vessels.
Keywords
Introduction
ST-segment elevation (STE) of anterior leads is suggestive of occlusion of the left anterior descending artery (LAD) and that of right coronary artery (RCA) or left circumflex artery (LCX) leads to STE of inferior leads. The presence of simultaneous ST-segment elevation (SST-SE) in both anterior and inferior leads can be confusing. Simultaneous anterior and inferior STE makes it difficult for physicians to localize which vessel is the true infarct-related artery (culprit vessel) without angiography. 1 Despite the present era of primary percutaneous coronary intervention, coronary angiography still sometimes cannot easily identify the true infarct-related artery if more than one lesion is noted in one single coronary artery (“one lesion, one artery”, “two lesions, one artery”) or involvement of different coronary arteries (two lesions, two arteries).
Case Presentation
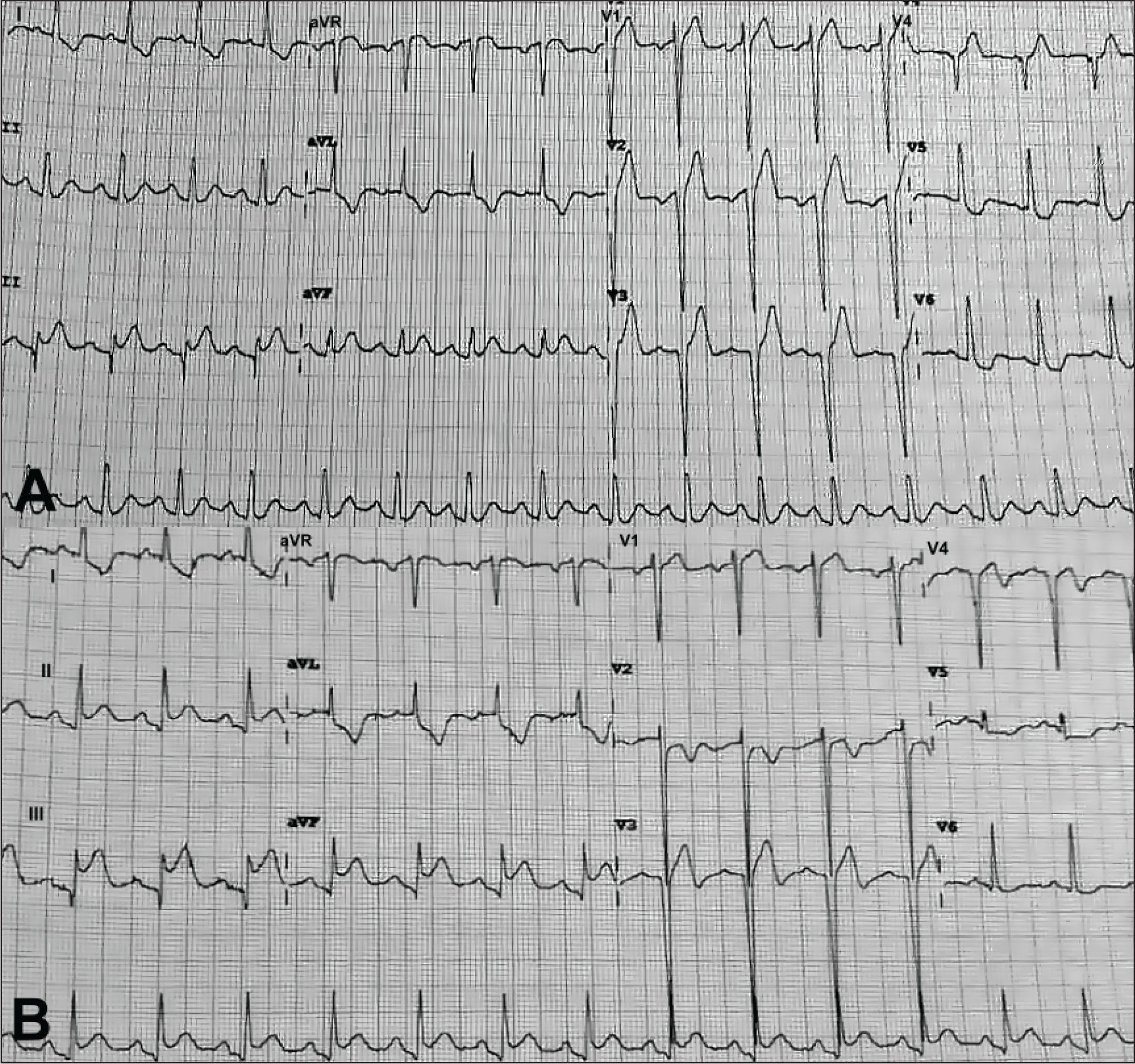
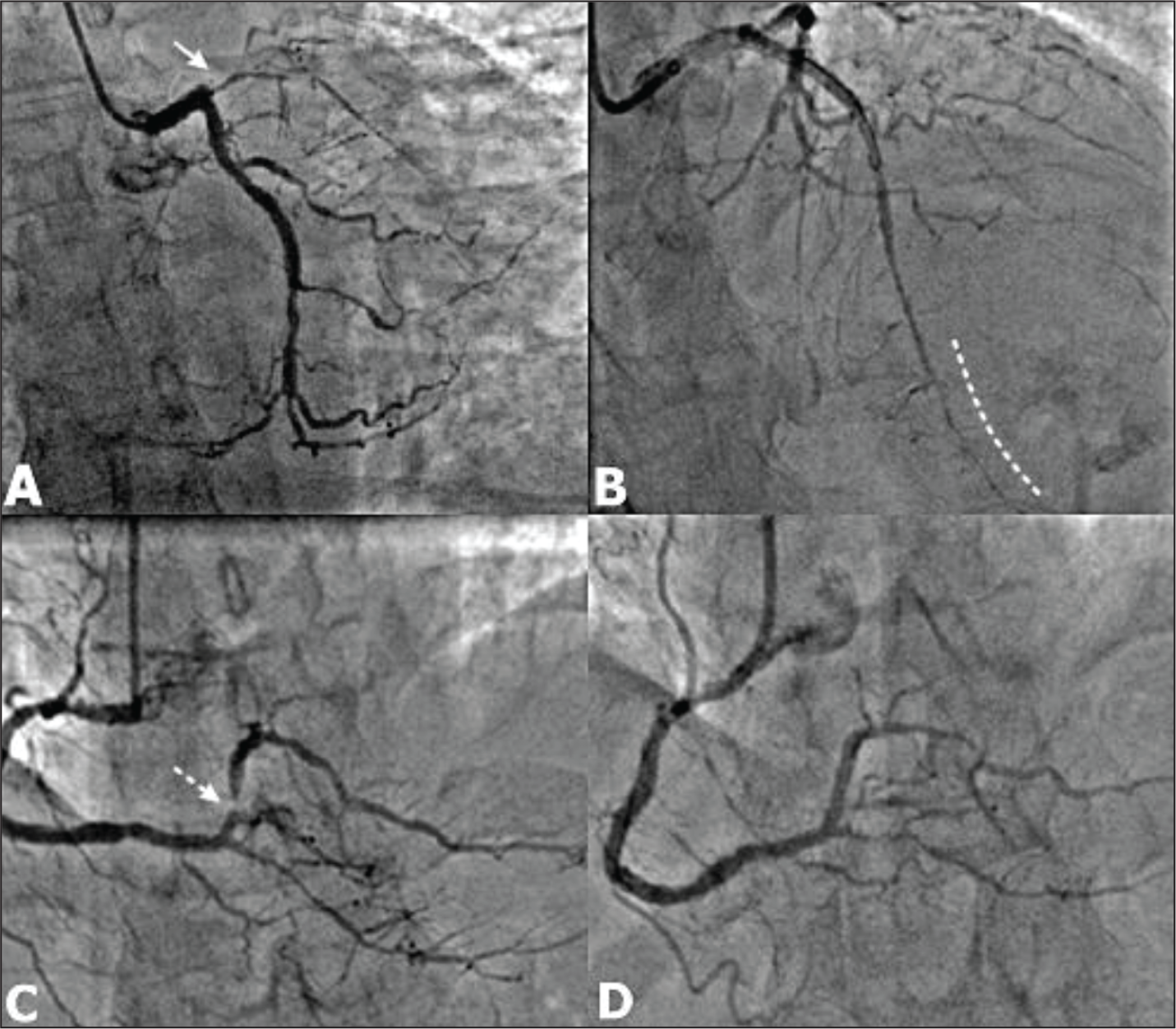
Let’s explain this phenomenon using a case study of 38-years-old male, smoker, and newly detected diabetic that presented with retrosternal chest pain for 6 h. Electrocardiography (ECG) showed hyperacute STE in leads V1 to V4, III, and aVF with reciprocal ST-segment depression in leads I, aVL, and V5 to V6 (Figure 1A). His troponin level was elevated, and echocardiography demonstrated presence of regional wall motion abnormality of anterior, mid, and distal interventricular septum and apex. Coronary angiography revealed thrombotic occlusion of the ostioproximal segment of the LAD and critical stenosis of the proximal segment of the posterolateral branch (PLB) of RCA. Also, there was a diffuse long segment stenosis of posterior descending artery (PDA) (Figure 2A, C). He underwent primary percutaneous intervention using drug-eluting stent (DES) to the proximal segment of the LAD. After establishing flow to the LAD, final angiography demonstrated diffuse disease of the distal LAD extending beyond the left ventricular apex (Type III LAD) (Figure 2B). Also, percutaneous transluminal coronary angioplasty to the proximal segment of the PLB using DES was done (Figure 2D). Post procedure, ECG showed reduction of STEs with T-wave inversions in leads V2 to V4 but there was persistence of STE in leads II, III, and aVF with ST-segment depressions in leads I, aVL, V5 to V6 (Figure 1B). The similar pattern in ECG was observed on the next day and before discharge on the second day of procedure with further amelioration of ST-T changes. Patient has no symptoms after a 9-month follow-up on a protocol-based medical management.
(A, B) Electrocardiography done in emergency room showing simultaneous ST-segment elevation (STE) in anterior (V1-4) and inferior leads (III, aVF) with reciprocal changes in lateral leads (I, aVL, V5-6) (Panel A). After primary angioplasty, there was resolution of STE of anterior leads with T wave inversion but persistence of STE of inferior leads (II, III, aVF) and reciprocal changes in lateral leads (I, aVL, V5-6) (Panel B).
(A-D) Coronary angiography in RAO caudal view showed osteal thrombotic occlusion of the left anterior descending artery (LAD) (white solid arrow, Panel A) with nonobstructive lesion of the left circumflex artery (LCX). After establishment of the flow in the LAD, there was a diffuse significant stenosis of the distal LAD (curved dashed white line, Panel B). Coronary angiography of the right coronary artery showed nonobstructive lesions of the proximal and distal segment of the right coronary artery (RCA), posterior descending artery, and critical stenosis of the PLB (dashed white arrow, Panel C). After angioplasty of the PLB, there was thrombolysis in myocardial infarction (TIMI) III flow (Panel D).
Discussion
One Lesion, One Artery
In our case, there were two significant stenoses/occlusion of the wrapped LAD (two lesions, one artery) and also a critical stenosis of PLB (two lesions, two arteries). If the patient has a wrap-around LAD and location of the occlusion is distal to first diagonal artery, ST-segment is elevated in anterior and inferior leads simultaneously. A “wrap-around LAD” is defined as a LAD from a post-reperfusion coronary angiogram that perfuses at least one-fourth of the inferior wall of the left ventricle in the right anterior oblique projection, also labelled as a type III LAD. 1
Wrapping around the left ventricular apex, according to Kobayashi et al, 2 reduces the risk of adverse outcomes in patients with anterior wall myocardial infarction (MI). New onset heart failure was lower in patients with wrap-around LAD at the end of a year in their INFUSE-AMI report.
Yip et al 3 evaluated the clinical features of this distinctive ECG manifestation of the simultaneous STE in the precordial and inferior leads and its impact on clinical outcome. A total of 4% of the patients presented with MIs had simultaneous STE in the precordial and inferior leads. Patients with nonwrap-around LAD (Group 2) had more STE of inferior leads [>2 mm] than those with wrap-around LAD (Group 1). Also, Group 2 patients had adverse clinical presentations like cardiogenic shock, acute left ventricular failure, and more mortality.
Another explanation for inferior STE is probably occlusion of the “super-dominant LAD” or type IV that also supplies the inferoposterior region by continuation as PDA. This anomaly is called as “anomalous origin of PDA from LAD or hyperdominant LAD”.4, 5
Also, an isolated right ventricular MI or with inferior wall involvement may produce SST-SE secondary to anteriorly oriented injury of current generated depending on the magnitude of the ratio of the coexisting electrical forces created by the concomitant inferior, lateral and right ventricular ischemia, the degree of horizontal rotation of the heart, and the configuration of the body. 6
Two Lesions, One Artery
The occlusion of distal segment of the LAD or its branches secondary to embolism, which supplies the inferior wall, can lead to SST-SE of inferior and anterior leads. 7 Sometimes, there can be diffuse or discrete atherosclerotic involvement of the distal segment of the LAD as in our case.
Two Lesions, Two Arteries
Ilia et al 8 reported a case where concomitant involvement of a RCA and the distal LAD resulted in simultaneous STE of antroinferior leads. Hsu et al 4 reported a case where patient had simultaneous inferolateral STE as an initial presentation of the LAD occlusion who had previous occlusion of the distal LCX. Authors speculated that old anteroseptal MI can make anterior wall isoelectric and new occlusion of LAD leads to this phenomenon.
Our case highlights that SST-SE could be due to critical stenosis/occlusion of two epicardial coronary arteries or presence of critical stenosis/occlusion of one or two different segments (proximal and distal) of a single major epicardial vessel (wrap-around LAD) associated with critical lesions of other vascular territory. In the context of acute coronary syndrome, the coexistence of two or more critical stenoses in the same or two separate coronary arteries affects the ischemia/infarction pattern in ECG.
Conclusion
The explanation for the simultaneous STE in anterior and inferior leads in our case despite restoration of flow to the LAD was the presence of diffuse disease of the distal LAD, which was wrapped LAD (1 artery, 2 lesions) and also the presence of the critical stenosis of the PLB branch of the RCA (2 artery, 2 lesions). Rarely, these combined features can lead to the phenomenon of simultaneous STE which otherwise could individually be responsible for the same.