
Abstract
Objective:
The study included patients with known or suspected coronary artery disease. It aimed to demonstrate the incremental value of the routine nitrate augmentation in stress-rest technetium-99m methoxyisobutylisonitrile (Tc-99m MIBI) myocardial perfusion scintigraphy (MPS).
Material and Methods:
Standard stress and rest MPS was performed, followed by a second rest study with isosorbide dinitrate intervention within 5 days. The redistribution of Tc-99m MIBI was compared between stress and rest images, and interpretation of the study done as normal, scarred, and ischemia ± mixed lesion groups. The rest studies were compared with the rest nitrate studies. Summed rest score (SRS) and summed rest nitrate score (SRNS) were calculated. The summed difference score (SDS) of SRS and SRNS was calculated for each group.
Results:
A total of 50 patients were included in the study. Based on the routine MPS, patients were divided into the scar (n = 20), ischemia (n = 18), and normal (n = 12) groups. After the administration of nitrate, a significant fall in the blood pressure (P < .001) and an increase in the heart rate (P < .001) were noted. SDS was not significant in the normal MPS group (0.17 ± 0.57, P = .19). In comparison, substantial SDS was found in the ischemia ± mixed lesion (4.33 ± 3.43) and scarred (3.5 ± 3.15), respectively (both P < .001). Percentage improvement in the SRS from SRNS was found less than 2% for normal MPS while 18% and 29% for scarred and mixed groups, respectively.
Conclusion:
Routine MPS (stress followed by rest) underestimate ischemia and viability, which can be significantly reduced by utilizing nitrate augmentation in all patients with abnormal stress MPS. This could lead to a significant change in the extent and severity of ischemia and viability.
Keywords
Introduction
Myocardial perfusion scintigraphy (MPS) is a commonly used noninvasive imaging modality for the diagnosis of coronary artery disease (CAD). Out of several MPS indications, the two leading questions to be answered are stress-induced ischemia and viability. Identifying ischemia and its extent is paramount for CAD patient management and risk stratification. 1 However, in a large subset of patients with myocardial infarction (MI), the relevant clinical question is evidence of myocardial viability in akinetic or hypokinetic regions. It holds even after coronary angiography as the success of revascularization depends upon the viable myocardium.
Many studies revealed that patients with residual akinetic viable myocardium, that is, nonfunctioning myocardium demonstrate better outcomes after revascularization than patients with an extensive myocardial scar.2, 3 Patients with viable myocardial segments experience a better regional and global contractile function after revascularization. They also demonstrate better exercise capacity, long-term event-free survival, and improved symptoms compared to medical therapy alone.4–6 However, if scarring is predominant, the risk of death remains intermediate and is not improved with revascularization. 7 MPS may be able to answer all clinical relevant questions of ischemia and viability in one study.
Technetium-99m methoxyisobutylisonitrile (Tc-99m MIBI) is one of the most commonly utilized radiopharmaceuticals for MPS. However, it is not a perfect marker for MPS. The standard stress-rest protocol may underestimate viability, shown by Thallium, PET or, post-revascularization recovery of that segment. 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) demonstrates viability in nearly one-third of the patients showing mild to moderate defect 99mTc MIBI MPS. 8 However, it not universally available. Nuclear medicine laboratories performing routine stress-rest perfusion imaging with PET radiopharmaceuticals are few.
To improve the sensitivity of MIBI, MPS use of nitroglycerine (NTG) has been tried. NTG causes relaxation of the vascular system and decreases pulmonary vascular pressure and intraventricular pressure. NTG improves myocardial perfusion by reducing wall tension and myocardial oxygen demand.9, 10 Few studies have shown that short-term administration of isosorbide dinitrate with 99m Tc-MIBI increases uptake in some chronically hypoperfused territories.11–13 However, authors have seen discrepant findings by NTG intervention. 14
The dual-tracer thallium-201 (201T1) chloride (rest) and 99mTc MIBI (stress) acquisition technique have shown superiority over the single-tracer MIBI protocol. 15 However, due to the physical characteristic of 201Tl, many studies compared nitrate Tc-99m MIBI MPS with 201Tl. The authors found that it is not less effective than rest-redistribution Tl-201 for evaluating viability, thus predicting post-revascularization recovery.16–19
Underestimation of ischemia and viability may change patient’s management from revascularization to medical therapy. It could lead to an increase in morbidity or mortality. Routine use of nitrate is still not recommended in the recent MPS guidelines. 20 We hypothesized that the regular use of the nitrate in all the patients might have incremental value. We compared the rest images with the rest nitrate images. We noted the standard stress-rest MPS findings, compared the value of nitrate images in the finding of standard MPS. We also evaluated the safety of nitrate.
Methods
Study Population
A single-center, prospective study was done in a tertiary care hospital between November 2005 and September 2006. Fifty consecutive patients were recruited who were referred to the department for MPS with various indications. All patients were known or suspected cases of CAD. All the patients gave informed consent. Exclusion criteria were those who did not provide consent for the study, hypersensitivity to nitrates, systolic blood pressure (SBP) less than 100 mmHg, or diastolic blood pressure (DBP) less than 70 mmHg.
Study Protocol
All patients had undergone MPS on 2 different days. Standard stress (exercise or adenosine) and rest MPS performed on the first day. Within 5 days of the first study, a second rest study with isosorbide dinitrate was done. In the case of cardiac event or new symptom in symptoms between 2 studies, the patient was excluded from the study group. All patients kept fasted for 4 h before Tc99m-MIBI injections. Relevant clinical history of the patients was taken. It included past illness, investigations, interventions, and medications.
Stress Study
All patients reported for stress testing after fasting for 6 h. Beta-blockers and nitrates were stopped 1 day before. Patients were advised to refrain from the caffeine-containing beverages for 24 h before the test. Patients were stressed on a bicycle ergometer using the Bruce protocol. Tc99m MIBI (296 MBq) was injected at the peak exercise, and the exercise continued for another min. Patients failing to attain a target heart rate (HR) on physical exercise underwent pharmacological stress. Intravenous adenosine (140 µg/kg/min for 6 min, injecting 296 MBq Tc99m MIBI after 3 min of adenosine infusion) was used. Bread and butter was given to all patients to aid hepatobiliary clearance of MIBI. Imaging commenced approximately 45 min after stress injection on dual-head SPECT (DST XL; SMV France). Images were acquired over 180° for 30 s in each of 64 projections using low-energy all-purpose collimators
Rest Study
In the rest study, patients were injected 888 MBq Tc-99m MIBI after 3 h of the stress study. Imaging was done approximately 45 min after injection. All acquisition parameters, such as time per projection, bed height, and arm positions, were kept identical with stress imaging for each patient.
Rest (Nitrate) Study
Patients were requested to come within 5 days without stopping any medication. Baseline blood pressure (BP) and HR were measured. Patients were given 5 mg of sublingual isosorbide dinitrate in lying down position. Pulse and BP measured every 10 min. A total of 296 MBq Tc-99m MIBI was injected when SBP was reduced by 10 mmHg or 20 min after the nitrate’s sublingual administration, whichever was earlier. The imaging protocol was the same as in an earlier rest study.
Processing
The processing is done on EMORY cardiac toolbox. Images were prefilter using Metz filter (FWHM 2.35 and order 3.25) and then reconstructed by filtered back-projection with a Ramp filter (quantitative). Reconstructed SPECT images were visually analyzed for change in tracer distribution, and quantitative analysis was done by a semiquantitative method.
Interpretation of the Images
The 2 experienced physicians individually analyzed all scans. They have experience of 5 and 15 years in the field of MPS imaging, respectively. Any discrepancy is resolved by mutual consensus. Image analysis was done for every patient using Emory cardiac toolbox. Images were analyzed using both visual and semiquantitative analysis. The conventional interpretation of stress-rest images were done. The amount of redistribution of MIBI compared between the rest image and nitrate augmented images. Summed rest score (SRS) and summed rest nitrate score (SRNS) were derived for all patients. For quantitation to see the difference between rest and rest nitrate image, rest image of the day 1 is considered as stress image and nitrate augmented image as rest. SRS and SNRS were obtained, and summed difference score (SDS) was calculated. The percentage of improvement in summed score was calculated as SDS divided by SRS. Ejection fraction at rest and nitrate augmented image calculated in gated images.
Statistical Analysis
The normality of continuous variables was established, and variable was normally distributed when Z value of the skewness was within ±3.29. The normality of the continuous variable was expressed as means ± standard deviation while categorical variables as frequencies (%). Independent samples t test was used to compare the means between two groups, while Chi-square tests (or Fisher exact test) were performed to test the association between two categorical variables. Pearson correlation was done between various clinical parameters. Statistical Package for Social Sciences, version 17 (SPSS-17; IBM, Chicago, USA) was used to analyze data.
Results
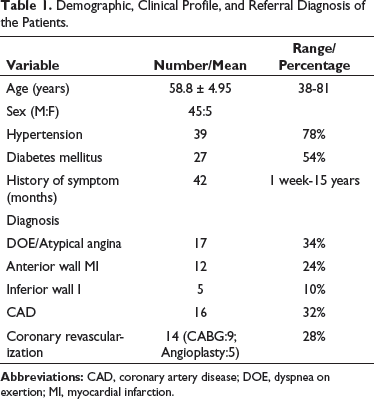
Patient Demography
Demographic, Clinical Profile, and Referral Diagnosis of the Patients.
Interpretation of Standard Stress-Rest MPS
The patients were divided into 3 groups (normal, ischemia or mixed lesion, and scarred) based on the stress-rest scan findings. The highest number of the patients were in scar group (n = 20, 40%) followed by ischemia (n = 18, 36%) and normal MPS (n = 12, 24%) group.
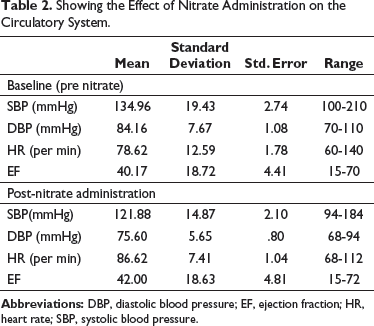
Interpretation of the Rest-Rest Nitrate MPS
Showing the Effect of Nitrate Administration on the Circulatory System.
Paired Sample t Test Between Various Parameters Between Rest and Rest Nitrate Study.
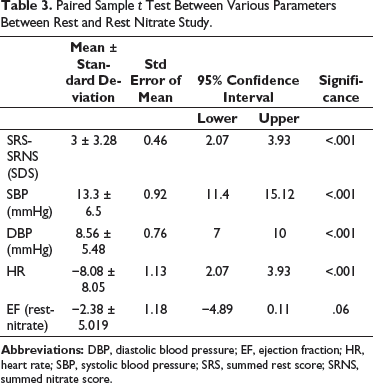
We found SRS, SRNS, and SDS as 16.53 ± 16.62 (median 18.0), 13.47 ± 10.66 (median 13.0), and 3.06 ± 3.281 (median 2.0), respectively. A significant difference was noted between SRS and SRNS (SDS) (P < .001). No significant difference noted between left ventricle ejection fraction between the two studies (P = .06) (Table 3).
Performance of the Test Between Different Patient Groups
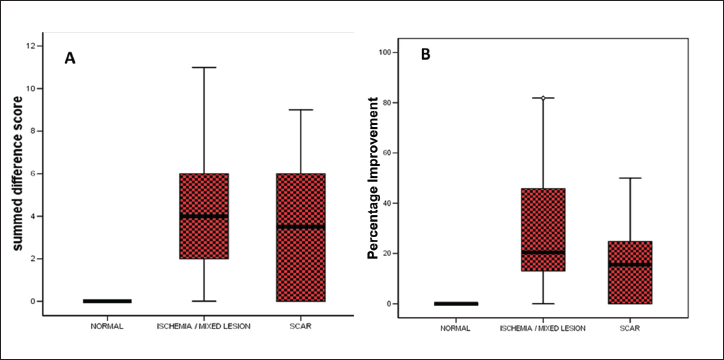
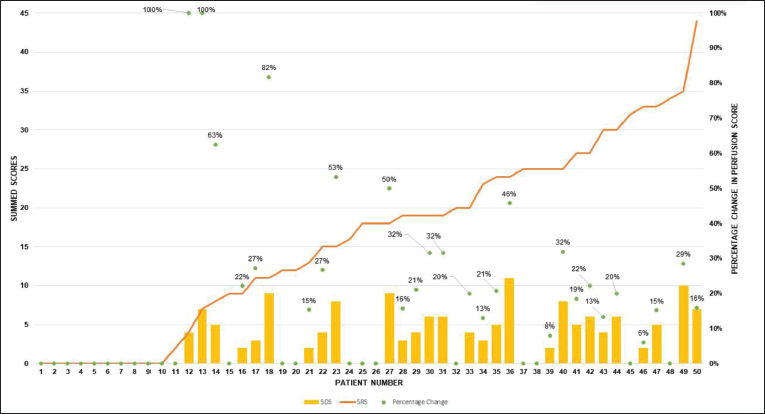
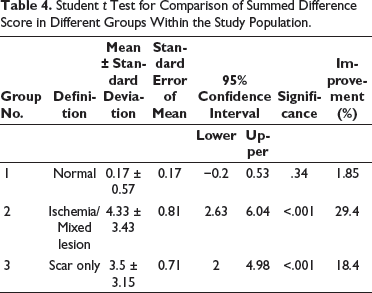
The effect of rest-nitrate study was noted between groups. There was no significant difference in SDS in the first group, that is, normal MPS group (0.17 ± 0.57, P = .19), while the improvement was found in the rest of the two groups, that is, ischemia only or mixed lesion (4.33 ± 3.43) and scar (3.5 ± 3.15) only, respectively (both P < .001). It indicates a significant improvement in SRNS following nitrate intervention (Figure 1A). Percentage improvement in the summed rest images was calculated for all the groups (Figure 1B). It was found less than 2% for normal MPS while 18.4% and 29.4% for scarred and mixed groups, respectively. In 21 patients, the SDS was 4 or more than 4 (Table 4, Figure 2–3).
(A) Showing summed difference scores in different groups within the study population. (B) Percentage improvement in the perfusion after administering the nitrate in each group.
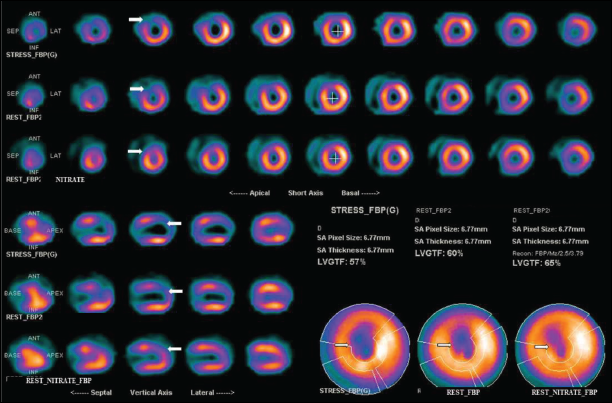
This figure shows stress, rest, and nitrate rest technetium-99m methoxyisobutylisonitrile (Tc-99m MIBI) image of a patient. The upper 3 rows are short-axis images of the stress, rest, and rest nitrate, respectively. The lower 3 rows are the vertical long-axis images of these. The stress image shows a severe perfusion defect in the apex, apicoanterior, and apicoseptal walls. Rest images show similar defects with minimal improvement in the perfusion. Myocardial perfusion scintigraphy (MPS) findings are suggested of fixed perfusion defects in the MPS correspond to scarring. Rest nitrate images show near-normal perfusion in these segments. MPS findings after comparing stress and rest nitrate images are severe perfusion defects in the involved region.
This figure shows findings from all the patients in the study based on increasing summed rest score (SRS; orange line). Summed difference score (SDS, yellow bars) for the same patient is seen. The percentage improvement in perfusion is shown as a green dot (parenthesis %) for an individual patient.
Student t Test for Comparison of Summed Difference Score in Different Groups Within the Study Population.
Performance of the Rest-Rest Nitrate Augmentation Based on the Coronary Artery Involvement
Out of all patients, details of coronary angiography was available in the 25 patients. Left anterior descending (LAD), left circumflex (LCX), and right coronary artery (RCA) showed significant lesion (>70% luminal narrowing on the visual analysis) in 20, 13, and 10 vessels, respectively. We applied the Pearson’s correlation between the vessels and the SRNS, and we found a low positive correlation for LAD (P = .431), RCA (P = .545), and LCX (P = .03) arteries.
Discussion
In this study, we investigated the relative insensitivity of MIBI if used as routine stress rest imaging. Significant underestimation of viability in rest imaging may lead to misinterpretation or underestimation of ischemia and viability. Our data suggest that isosorbide dinitrate administration in such patients enhances hypoperfused but still viable myocardium detection. It leads to a change in the management of significant numbers of patients.
In CAD patients, 99mTc-MIBI uptake underestimates myocardial viability in comparison to 18 FDG-PET. Complete or partial viability may be noted in the significant proportion of the patients showing mild to moderate perfusion defects.8, 21 Altehoefer et al 8 compared the degree of 99mTc-MIBI uptake reduction (in the percentage of peak activity) to 18 FDG uptake. Nonviability on FDG noted in 80% of severe (≤30% of peak uptake), 48% of moderate (31%–50% of peak uptake), and 31% of mild (>50% of peak uptake) defects on MIBI MPS. The authors also showed that complete viability was found in none of the severe defects compared to 29% and 35 % of the moderate and mild perfusion defects, respectively. We found a similar result that nearly 20% of patients showed improvement in perfusion.
Nitrate Tl-201 imaging is widely used to determine stress-induced ischemia as well as hibernating myocardium. Thallium retention requires blood flow, intact, and functioning cell membranes, therefore, signifies cell viability. Studies have found that MIBI may underestimate viability in comparison to 201-thallium. Studies have compared nitrate augmented MIBI imaging with various protocols of Tl-201.9, 16, 19 The dual-tracer TI-MIBI acquisition technique appears superior to the single-tracer MIBI protocol. 15 As the physical characteristic of 2 radionuclides is quite different, it results in a different count density. It may affect evaluating the degree of defect reversibility, especially in patients with prior MI. 22 Because of these findings, authors have suggested that baseline-nitrate Tc-99m MIBI MPS is equivalent to rest-redistribution Tl-201 in predicting-post revascularization recovery.10, 16-19 We used 99mTc-MIBI for the study due to the kit’s excellent imaging characteristics, wide availability, and long shelf life.
Several authors have found that isosorbide dinitrate’s administration immediately before Tc99m sestamibi increases tracer uptake in some chronically hypoperfused asynergic territories. This finding correlates with the observation of post-revascularization functional recovery.11-13 In a similar study, Thorley et al 23 found that glyceryl trinitrate given before the rest injection appears to improve the detection of ischemic hypoperfused myocardium. 23 Our study found a similar result that some of the nonperfused/hypoperfused segment showed increased perfusion after nitrate administration. Galli et al 24 demonstrated that after NTG, the mean perfusion defect significantly decreased (29 ± 4%, range: 7-74). 24 We observed a similar trend and found 18.4% (0%-24%) and 29.4% (16%-45%) improvement in the scarred and mixed groups’ perfusion.
Pre-CABG nitrate augmented study predicts post-CABG improvement in cardiac function. Several authors have shown that ejection fraction levels and reversibility score increased significantly after nitrate administration.25, 26 However, we did not follow-up with our patients, so post-revascularization change in perfusion and function is not available. We did not find any significant changes in cardiac volumes and ejection fraction, as seen by other authors. 27 It may be due to the small study population. Other studies have noted most discordance (MIBI nonviable/FDG viable segments) in the inferior walls. 21 However, we demonstrated only a weak correlation between arterial involvement and SRNS.
Tl-201, Tc-99m MIBI, and Tc-99m tetrofosmin all performed equally well in clinical terms, with high sensitivity and specificity for angiographic stenosis. 28 A study by Siebelink et al 29 showed no difference in patient management or cardiac event-free survival based on 13N-ammonia/18 FDG PET or stress/rest 99mTc-sestamibi MPS. Although PET is considered the best predictor of hibernation, a combination of technique with a high PPV (echocardiography) and a high NPV (PET/MIBI MPS) may represent the optimal clinical choice. 30 Tc-99m tetrofosmin G-SPECT shows excellent (κ = 0.85) agreement with FDG PET. FDG PET could change management only in 13% of the patients. 31 So, the tracer of choice for MPS remains the radiopharmaceutical, which is widely available and cost-effective. MPS is widely available and technologically less demanding than PET, thus widely utilized. Among the SPECT tracer, the main competitors are Tl-201 and Tc-99m pharmaceuticals. There are various technical differences between the tracers. One of the significant limitations of Tl-201 MPS is low image quality, especially in obese patients, and problems distinguishing attenuation artifacts from defects.
Our study could demonstrate the reversibility of the MIBI MPS defects after nitrate intervention in many patients. It raises doubt on a conventional rest sestamibi study’s ability to quantify the real extent of the scarred area and ischemia reliably. Our results suggest that sestamibi scans’ accuracy for detecting dysfunctioning but viable myocardium is low, which could be easily improved by isosorbide dinitrate. This improvement is observed in scarred myocardium and the mixed lesions, as reported on routine stress-rest imaging. It may have high prognostic and management applications, such as guiding treatment from medical to revascularization.
However, our study has a few significant limitations. Our study was a single-center study. Attenuation correction could not be done. Most of the patients were male. Angiography information was not available in all patients. Patients with no or mild abnormality on the MPS did not undergo angiography. Follow-up information is not available as the study was cross-sectional in design.
Conclusion
Nitrate augmented leads to change in perfusion for both ischemic as well as infarct group. Based on our study, we suggest that routine 99mTc-MIBI with stress and nitrate augmented rest MPS is safe and straightforward. A busy nuclear medicine department can efficiently conduct this protocol without additional time. It may lead to a change in management in a significant number of patients compared to conventional 99mTc MIBI stress-rest MPS. One of the main advantages of this approach is the low cost and wide availability, which would enhance widespread adoption.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.