
Abstract
Objective:
To assess knowledges, attitudes, and practices of health personnel in Bujumbura hospitals with regard to hypertension during pregnancy.
Methodology:
This study has been conducted on health personnel of gynecology and obstetrics department of three national referral hospitals in Bujumbura. It is a descriptive cross-sectional study to assess knowledge, attitudes, and practices. Data were collected by a questionnaire and analyzed by Epi Info 7.2.
Results:
In a total of ninety-seven health workers participated in our study and 78.3% were paramedics with 53.6% of nurses and 24.7% of midwives. Medical doctors represented 21.6% of the participants. The sex ratio was 1.4 in favor of women. The professional experience was more than 5 years for 64.9% of participants. Concerning knowledge about hypertension; 74.2% of participants correctly defined hypertension during pregnancy. Despite this, only 48.4% respected conditions about its measurement. concerning attitude toword hypertension; 94.8% of participants informed their patients about the risks linked to hypertension in pregnancy before any therapeutic strategy. The antihypertensive drugs contraindicated during pregnancy were known by 54.6% of participants. To prevent preeclampsia, low doses of aspirin and calcium were prescribed by 42.2% of participants.
Conclusion:
Hypertension during pregnancy is a worrying situation for health personnel, which still has many theoretical and practical gaps.
Introduction
Burundi, like other countries, is committed to the policy to improving maternal and child health. According to the 2016-2017 Demographic Health Survey in Burundi, 1 maternal mortality is estimated at 334 deaths per 100,000 live births; whereas in Tunisia in 2005, the mortality rate was estimated at 48 per 100,000 live births. 2 Pregnancy is a physiological condition of the pregnant woman which can be accompanied with behavior change and modification of maternal organism from conception to childbirth.1, 3-5 Despite in normal condition, pregnancy sometimes involves a vital maternal and fetal prognosis, especially if the woman does not respect some rules of hygiene in case the pregnancy is associated with certain pathologies including hypertension.4, 5 Hypertension is a common situation during pregnancy as it affects 6% to 10% of pregnant women; it is also the first marker of maternal and infant morbidity and mortality.6, 7
One of strategies to reduce maternal complications from hypertension in pregnancy is to improve the quality of preventive care, which necessarily involves better knowledges of pregnancy hygiene and associated pathologies. The objective of this work was to assess knowledges and behavior of health personnel with regard to hypertension in pregnancy.
Methodology
It was a descriptive cross-sectional study of health personnel directly taking care of pregnant women (medical and paramedical) working in gynecology-obstetrics department. The study targeted all active health personnel of the three hospitals among the national referral hospitals in Bujumbura such as the University Hospital Center of Kamenge (UHCK), the Prince Regent Charles Hospital (PRCH), and the Military Hospital of Kamenge (MHK). Those hospital were chosen due to their large number of deliveries. From July 1, 2019 to September 30, 2019, we recorded 1,317 deliveries at UHCK, 954 at PRCH, and 699 at MHK.
This study was conducted under the authorization from the hospital-university committee of ethics and after freely agreement of duly explained participants about the survey importance. We included all pregnant women, in this study, except those who didn’t want to answer the survey questionnaire. A written anonymous questionnaire was used to collect data from participant who had agreed to participate voluntarily in the study. Anonymity and confidentiality were essential from the time of collection until the results dissemination. Investigator found participants at their usual place of work, and an appointment to complete the full questionnaire was fixed. The questionnaire was made up in 2 sections. The first section was used to collect demographic data such as age, sex, place of investigation, and qualification of participant. The second section used for the assessment of health professional’s knowledge, attitude, and practices toward high blood pressure (HBP) in pregnant women; it contains questions related to conditions for measuring blood pressure, clinical manifestations, diagnostic tests, prevention and treatment; and attitudes and practices face up a HBP in pregnant woman.
Data collection was manual. Data entry, processing, and analysis were done using Microsoft Word and Epi Info 7.2 software. The descriptive statistical tests applied with 95% confidence intervals, a P value < .05 was considered as significant.
Results
Among 128 health personnel working in the gynecology-obstetrics department of the three hospitals, 97 had completed the questionnaire, representing a participation rate of 75.7%. There were three groups: nurses (53.6%), midwives (24.7%), and physicians (21.6%). The sex ratio was estimated at 1.4 in favor of female. The professional experience of participants was greater than 5 years for 64.9%.
Knowledges of Hypertension During Pregnancy
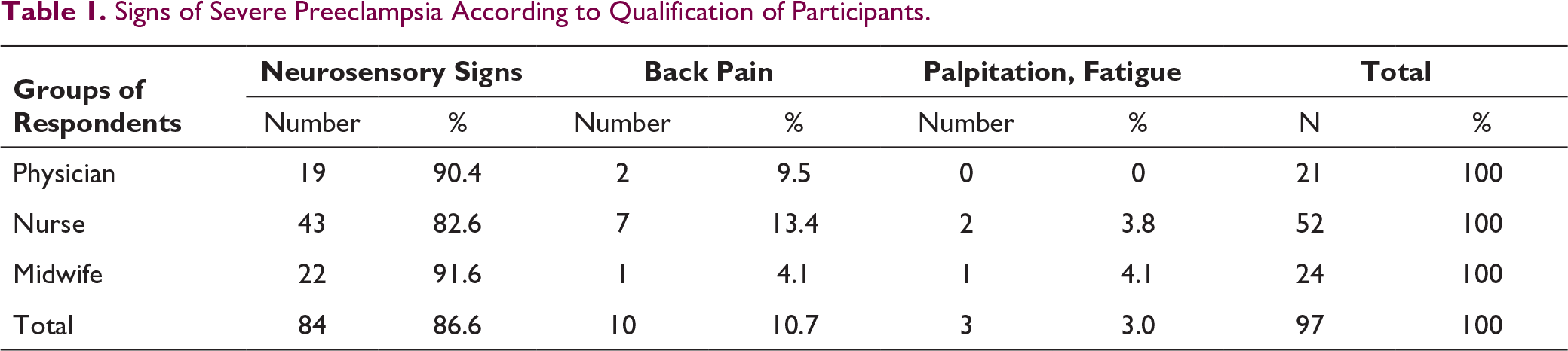
Signs of Severe Preeclampsia According to Qualification of Participants.
Attitudes Face Up Hypertension During Pregnancy
Ninety-four, which make up 96.9% of participants, claimed to systematically measure the blood pressure. However, the blood pressure measurement conditions were respected by 48.4% of participants. Around 93.8% of participants agreed that it is important to determine the basic blood pressure in the first trimester of pregnancy and 91.7% of participants considered that edema localized at the feet and ankles was the main sign of severe preeclampsia depending on the pregnancy stage.
Practices Toward Hypertension During Pregnancy
In our study, 94.8% of participants said that they informed patients about different aspects of hypertension during pregnancy before any therapeutic strategy. Forty-one, which make up a mean 42.2% of participants, namely 71.4% of physicians, 32.6% of nurses, and 37.5% of nurses, thought that the use of small doses of aspirin and calcium allowed the prevention of preeclampsia. To improve uteroplacental blood flow, a mean of 72.1% of participants including 95.2% of physicians, 65.3% of nurses, and 66.6% midwives recommended bed rest for all hypertensive pregnant women. Fifty-three, which make up 54.6% of participants, indicated that drugs belonging to the class of angiotensin receptor (AR) II antagonists, angiotensin converting enzymes (ACE) inhibitors, and diuretics are contraindicated during pregnancy.
Discussion
The objective of this work was to assess the knowledges, attitudes, and practices of health personnel regarding hypertension in pregnancy. According to Madika et al, 8 knowing the categories of hypertension in pregnancy is essential for its management. Hypertension during pregnancy is defined by SAP greater than or equal to 140 mm Hg or DAP greater than or equal to 90 mm Hg. The same authors 8 argued that gestational hypertension occurs during or after the 20th week of amenorrhea. In our study, 74.2% of participants correctly defined hypertension during pregnancy, namely 85.7% of physicians, 83.3% of midwives, and 65.3% of nurses. Preeclampsia is defined by the development of hypertension and proteinuria after 20 weeks of amenorrhea (>300 mg/L).8-10 In our study, preeclampsia was correctly defined by 95.2% of participants. Eclampsia, one of the deadliest complications of hypertension in pregnancy, it is defined by onset of seizures in woman who already has preeclampsia. 11 In our study, 95.8% of participants correctly defined eclampsia.
Most of the surveyed participants (96.9%) claimed to systematically measure blood pressure. Knowing that HBP is usually discovered incidentally, 12 blood pressure should be taken systematically for any patient. The conditions for measuring blood pressure are such that patients must be at rest in a quiet place for some moment, in a sitting position with an arm located at heart level, and an appropriately sized cuff (corresponding to 1.5 times the circumference of the arm) should be used.5, 13 The blood pressure measurement conditions, in our study, were met by an average of 48.4% of participants, including 71.4% of physicians, 42.3% of nurses and 41.6% of midwives. In addition, 93.8% of surveyed participants said that it was important to determine baseline blood pressure in the first trimester of pregnancy. According to Madika et al, 8 mild to moderate uncomplicated hypertension (absence of proteinuria, for example) does not require specialized care. When a clinical sign of severity (proteinuria, severe hypertension) appears, follow-up will be specifically coordinated by an obstetric and cardiologist team with immediate initial hospitalization.
In our study, 94.8% of participants said that they informed patients about different aspects of their pathology before any therapeutic strategy. In practice, pregnant women should be reassured by explaining that their pregnancy can progress normally.8, 14 In fact, informing and explaining pregnant women on the normal progress of pregnancy will make possible to control the risk factors of preeclampsia, to evaluate the control of hypertension, to replace teratogenic treatments, and to check the etiological balance.8, 14 To improve uteroplacental blood flow, 72.1% of participants recommended bed rest for any hypertensive pregnant woman. According to Madika et al, 8 a rest should be enforced quickly if the blood pressure figures worsen. A low-fat diet is not recommended but patient almost always benefits from smoking cessation assistance, knowing that Nicopatch can be prescribed without restriction with pregnancy.
In regard to prevention, aspirin does not prevent the onset of preeclampsia.8, 14 In our study, 42.2% of participants thought that the use of small doses of aspirin can help to prevent preeclampsia. For the drug management of hypertension in pregnancy, four first-line molecules (methyldopa, nicardipine, nifedipine, labetalol) are prescribed.8, 15 Thiazides are hypovolemic, ACE inhibitors and AR II antagonist are fetotoxic, and aldosterone antagonist are teratogenic.8, 15 In our study, only 54.6% of participants indicated that molecules belonging to the classes of AR II antagonists, diuretics, and ACE inhibitors are contraindicated during pregnancy.
Conclusion
Hypertension during pregnancy is a worrying situation for health workers, who still have many theoretical and practical gaps in our context. These gap toward knowledge, attitude, and practices of HBP during pregnancy were greater for low-level instructed health workers, except for the measurement of blood pressure. Facing up this problem, we recommend regular on-the-job training and up-to-date practical guide should also be provided.
Footnotes
Author Contributions
EN conceptualized the study and the paper and EB supervised the study conduct, reporting, and the write-up of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The study was approved by the Ethics Review Committee of the Faculty of Medicine, University of Burundi (certificate NO. FM/CE/27/05/2019).