
Abstract
A 31-year-old male was referred for a stress test due to worsening palpitations and chest pressure. His clinic 12-lead electrocardiogram was normal. At the time of his stress test, his pre-exercise electrocardiogram revealed an intermittent short PR interval with a delta wave. This pattern resolved during exercise, but in recovery he experienced paroxysms of supraventricular tachycardia. Imaging revealed low left ventricular ejection fraction. Given the diagnosis of Wolff-Parkinson-White Syndrome, he underwent radiofrequency ablation. His cardiomyopathy was presumed to be secondary to his Wolff-Parkinson-White, and an echocardiogram a few months later showed normalization of his left ventricular ejection fraction.
Case Presentation
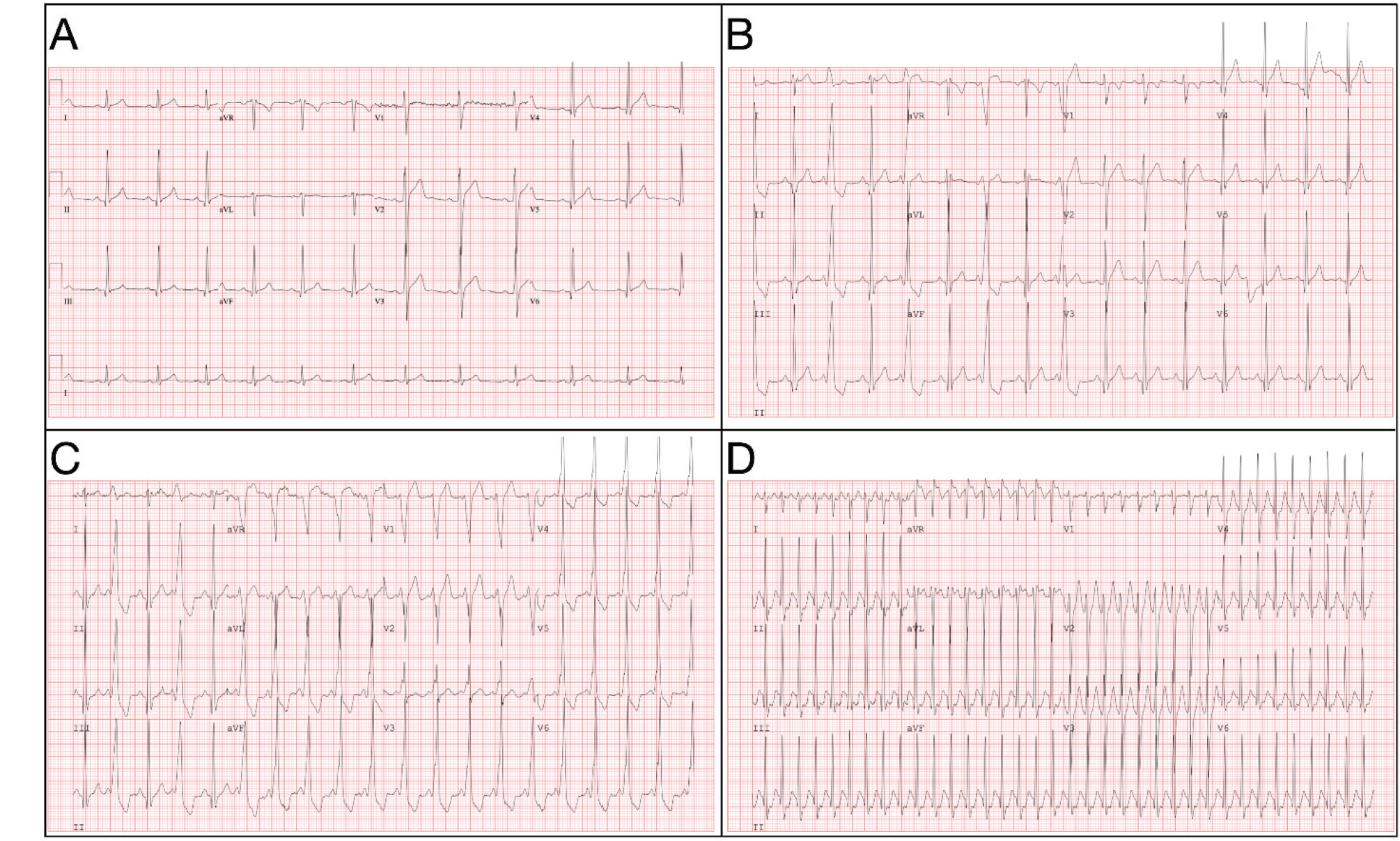
A 31-year-old male with no chronic medical problems or past history presented to a primary care clinic with worsening palpitations and chest pressure. He reported having had palpitations for several years but had never sought medical evaluation. In recent months, these had progressed to daily episodes lasting 20 to 30 min, often occurring as he was recovering from exertion. His work as a manual laborer often triggered his symptoms, which also included dyspnea and intense chest pressure (like “someone [was] pushing on his chest”) without radiation, and dizziness without syncope. In clinic, his electrocardiogram (ECG) was unremarkable (see Figure 1A).
After his initial visit he was referred for an exercise Single Photon Emission Computed Tomography (SPECT) stress test, and his pre-exercise ECG was notable for an intermittently short PR-interval with a delta wave (pre-excitation pattern; see Figure 1B). At about a minute of exercise, his ECG became fully pre-excited (see Figure 1C) which continued until 11 min 29 s (heart rate 176 bpm) when he abruptly lost his delta wave. About a minute into recovery, he evidenced a narrow complex tachycardia (164 to 250 bpm; see Figure 1D). His SPECT images revealed left ventricular systolic dysfunction with a left ventricular ejection fraction (LVEF) of 34% and global hypokinesis. Final SPECT imaging showed no inducible ischemia. An echocardiogram confirmed reduced LVEF.
Given that his stress test was negative for ischemic heart disease, and that screening labs regarding nonischemic causes of cardiomyopathy (iron studies (hemochromatosis), SPEP/UPEP (amyloidosis), HIV, TSH) were unremarkable, it was suspected that the patient had a Wolff-Parkinson-White (WPW)-mediated cardiomyopathy, he was referred to electrophysiology and ablation was recommended. At the time of his ablation, his atrioventricular reentrant tachycardia was easily induced with isoproterenol, and the accessory pathway was ablated successfully with radiofrequency energy. His postablation echocardiogram performed a few months after ablation showed that his LVEF had normalized.
(A) Clinic ECG, (B) pre-exercise ECG, intermittent pre-excitation, (C) 1 min exercise ECG, fully pre-excited, (D) 1 min recovery ECG; orthodromic AVRT.
Discussion
We report a case of tachycardia-mediated cardiomyopathy in a patient with WPW syndrome with low EF that was normalized with ablation. As predicted by the analysis of his ECG, his accessory pathway was localized to the right free wall. Given the location of the pathway, the cardiomyopathy may have resulted from the dyssynchrony of ventricular activation similar to a left-bundle-bunch-block-induced cardiomyopathy. 1 This condition is very similar to the cardiomyopathy that can result from traditional right ventricular pacing. 2 As such, right wall ablation is useful to negate the dyssynchrony. Additionally, the tachyarrhythmia itself, assuming a significant burden, could result in a tachycardia-mediated cardiomyopathy (TMC).
Of the many causes of cardiomyopathies resulting in systolic dysfunction such as ischemic heart disease, hypertension, and valvular dysfunction, TMC is less widely known. It has been associated with several tachycardias, including atrial tachycardia, and atrial fibrillation with poor rate control is the most common. In fact, this condition is a possible indication for AV nodal ablation and pacemaker placement or atrial fibrillation ablation.
TMC has not been systemically studied with relation to atrioventricular reentrant tachycardia, but some research has been performed. One prospective study of 30 adults (aged 40 ± 12 years) diagnosed with WPW revealed impaired LVEFs. These patients underwent radiofrequency ablation (RFA) and experienced improvements in ejection fraction, torsion, and dyssynchrony. 3
Other data suggest a relationship between WPW pattern on ECG and cardiomyopathy “without” arrhythmia. For example, in a study of 4 children with LV systolic dysfunction and WPW pattern on ECG, only 1 had documented tachycardia. In this setting, 2 of the 4 patients had a resolution of their cardiomyopathies following the resolution of preexcitation via ablation. 4 Another study of 34 patients (aged 14.2 ± 2.5 years) found that WPW with a right septal or posteroseptal accessory pathway was associated with impaired LVEF, which improved after RFA. No participants were noted to have arrhythmia before RFA and the authors felt it was unlikely that TMC had caused the LV dysfunction. 5
Thus, there may be multiple mechanisms that underlie the association between WPW and cardiomyopathy. These include TMC- and dyssychrony-related cardiomyopathy without a significant arrhythmia burden, although there may also be a genetic relationship between WPW pattern and dysfunctional cardiomyocytes in some cases. Of course, it may be multifactorial as well. In the case presented here, ablation was associated with both a resolution of symptoms (and likely arrhythmia) and the functional cardiomyopathy, and thus provides an example of a case of WPW-related cardiomyopathy “cured” with RFA.
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.