
Abstract
Background:
There is a paucity of contemporary Indian data about the prevalence of cardiac abnormalities in patients of connective tissue disorders (CTD) and their risk determinants.
Methods:
We prospectively recorded data from 35 consecutive CTD patients who presented to our out-patient department and had no significant cardiovascular risk factors at baseline. We also recorded data from their age- and sex-matched controls. All cases and controls were subjected to 12 lead electrocardiogram and echocardiography after routine investigations.
Results:
The CTD group comprised 19 (54.3%) patients of systemic lupus erythematosus, 12 (34.3%) patients of systemic sclerosis, 2 (5.7%) patients of mixed CTD, and 1 (2.9%) patient each of overlap syndrome and dermatomyositis. Cardiovascular involvement on echocardiography was documented in 71.4% of CTD patients despite majority of them having no cardiac symptom. Overt left ventricular (LV) systolic dysfunction was observed in 3 (8.6%) CTD patients, while subclinical LV systolic dysfunction was recorded in 13 (37.1%) patients. LV diastolic dysfunction was observed in 11.4% (n = 4) patients. RV systolic dysfunction was prevalent in 20% (n = 7) patients. Pulmonary hypertension was observed in 40% (n = 14) of CTD patients.
Conclusion:
The present study evaluated subclinical LV systolic dysfunction and pulmonary hypertension in about one third of CTD patients. It is imperative to screen for these abnormalities in CTD to ensure timely diagnosis and treatment.
Background
Connective tissue disorders (CTDs) represent a spectrum of systemic autoimmune diseases characterized by circulating autoantibodies and significant autoimmune-mediated organ damage. This heterogeneous group includes systemic lupus erythematosus (SLE), systemic sclerosis (SSc), Sjögren’s syndrome, mixed connective tissue disorder (MCTD), overlap syndrome, and inflammatory muscle diseases such as dermatomyositis (DM) and polymyositis (PM). 1 Specific or multiple organ systems targeted by the antibodies include pulmonary, renal, musculoskeletal, gastrointestinal, nervous, and hematological. One of the major causes of morbidity and mortality in patients of CTDs is the involvement of cardiovascular system. 2
Cardiac involvement in CTDs may be directed to all the components of the heart: pericardium, conduction system, myocardium, valves, and coronary arteries. 3 Libman-Sacks endocarditis is the most characteristic cardiac abnormality in SLE, seen in up to 50% of patients at necropsy in the past. 4 Pericarditis is a common cardiac manifestation of CTDs, seen in up to 39% of cases of SLE 5 and up to 43% cases in MCTD. 6 In the past, cardiac manifestations were severe at the time of diagnosis, often leading to death and frequently found in postmortem examinations. 4 But nowadays, because of diagnostic advancement, cardiac manifestations are often mild and asymptomatic as they can be recognized early by echocardiography and other noninvasive tests at initial stages of CTDs. 7 However, there is a paucity of contemporary Indian data about prevalence of structural and functional abnormalities of heart in patients of CTD and their risk determinants.
Methods
Study Design
This study was conducted as a case-control study in the department of dermatology and cardiology of our institute, which is a tertiary care hospital in a hilly northern Indian state.
Patient Selection
All consecutive patients of CTD diagnosed by using standard criteria reporting in the department of dermatology of our institute over one year with effect from 1 July 2018 to 30 June 2019 were screened for enrollment, and those willing were included. The patient’s attendants, relatives, friends, and the patients attending dermatology out-patient department for minor skin ailments such as fungal infections, common warts, acne patients, etc. constituted the control population and were screened to be enrolled as age- and sex-matched controls. Exclusion criteria consisted patients with congenital heart diseases, prior history of coronary artery disease, associated malignancies, chronic obstructive pulmonary diseases, pulmonary fibrosis secondary to infections, patients aged <10 years and >60 years, and patients having poor echo window and not willing to participate. Patients with other confounding factors such as diabetes, hypertension, and smoking were also excluded.
Data Collection
Self-reported data related to demographic characteristics and medical history were recorded as per the structured data recording format. This was followed by anthropometric and blood pressure measurement using validated tools and following standard guidelines. Body mass index (BMI) was calculated as a ratio of weight in kilograms divided by height in meters squared (kg/m2). The mucocutaneous examination was done as per the structured data format. Disease severity was assessed using Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) and modified Rodnan skin score for SLE and SSc, respectively. Around 10 cc of blood was withdrawn in fasting state and collected in separate container vials with appropriate reagents for biochemistry and hemogram. The Cockcroft-Gault equation was used to estimate creatinine clearance. Pulmonary status was also evaluated by using pulmonary function tests.
Cardiovascular Evaluation
All subjects underwent 12 lead “electrocardiogram” (ECG
Definitions
CTD was defined as the presence of any one of the disorders such as SLE, SSc, MCTD, undifferentiated connective tissue disorders (UCTD), DM, and PM diagnosed by the standard criteria. Controls were age- and sex-matched healthy asymptomatic individuals free of skin and systemic lesions suggestive of CTDs. “LV systolic dysfunction” (LVSD) was defined as the presence of any one of the following parameters: (a) LVEF <54% (females) and <52% (males), 8 (b) peak global strain in longitudinal plane > –20% (ie, <20% in absolute value), 8 (c) peak global strain in circumferential plane > –20% (ie, <20% in absolute value). “LV diastolic dysfunction” (LVDD) was defined if more than 2 of the available variables met the following abnormal cut off values 9 : (a) Septal e’ velocity < 7 cm/s, (b) lateral e’ < 10 cm/s, (c) average E/e’ ratio > 14. RV systolic dysfunction (RVSD) 8 was defined as any of the following: (a) TAPSE < 17 mm, (b) MPI > 0.43. “Pulmonary hypertension” 10 was defined as MPAP > 25 mm Hg. Deranged lipid profile 11 was defined as any of the following: S. cholesterol > 240 mg/dL , S. triglycerides > 150 mg/dL, S. LDL > 130 mg/dL, or S. HDL < 50 mg/dL. “Deranged LFT” was defined as values above the reference range in our institute’s pathology laboratory.
Ethical Clearance
The institutional review board approved the study protocol. The study was conducted with the patient’s understanding and consent.
Statistical Analysis
Categorical variables and continuous variable were reported as absolute frequency, relative frequency, and mean ± SD (standard deviation), respectively, and/or median and interquartile range for not normally distributed continuous variables. The difference between case and control groups of continuous variables and categorical variables was analyzed using unpaired t test and chi-square test, respectively. Variables found to have significant association with outcomes in univariate analysis were modeled in multivariable logistic regression to determine the independent association of the clinical characteristics. Data were analyzed using Epi-info software, version 3.4.3. A P value of <.05 was taken as statistically significant.
Results
Patient Characteristics
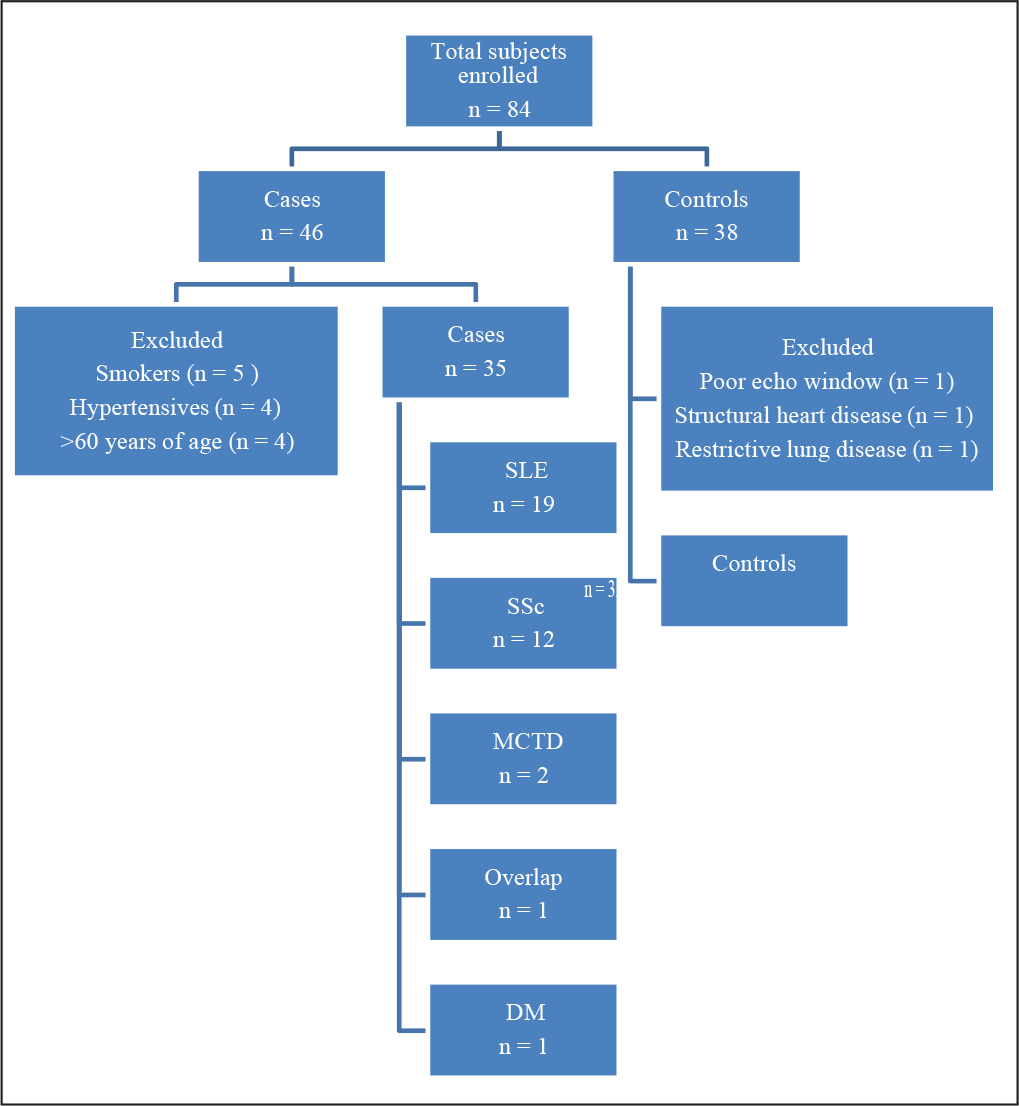
A total of 46 consecutive CTD patients were considered for enrollment in this study, out of which 11 met the exclusion criteria leaving 35 CTD patients for final analysis. Equal number (n = 35) of age- and sex-matched controls were also included in the study. There were 19 (54.3%) patients of SLE, 12 (34.3%) patients of SSc, 2 (5.7%) patients of MCTD, and 1 (2.9%) patient each of overlap syndrome and DM (Figure 1).
Demographic Characteristics
The mean age of CTD patients and control group was 36.9
Details of Enrolled Patient
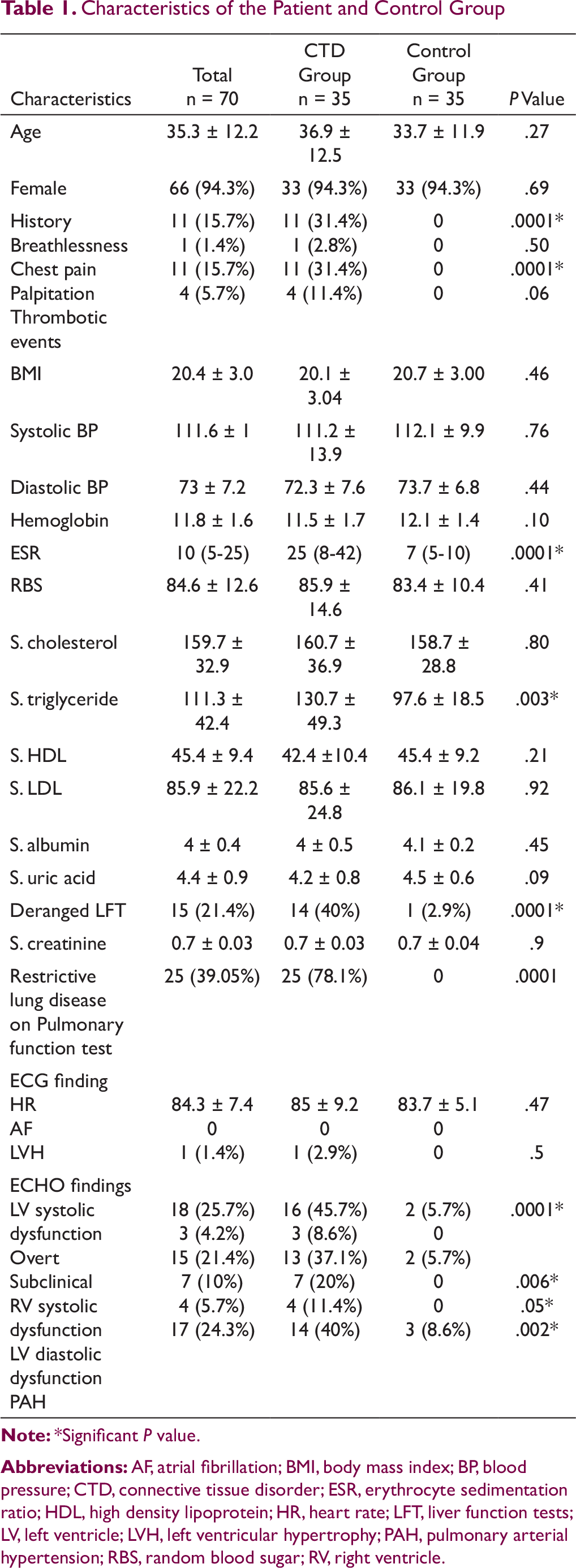
Characteristics of the Patient and Control Group
Medical History
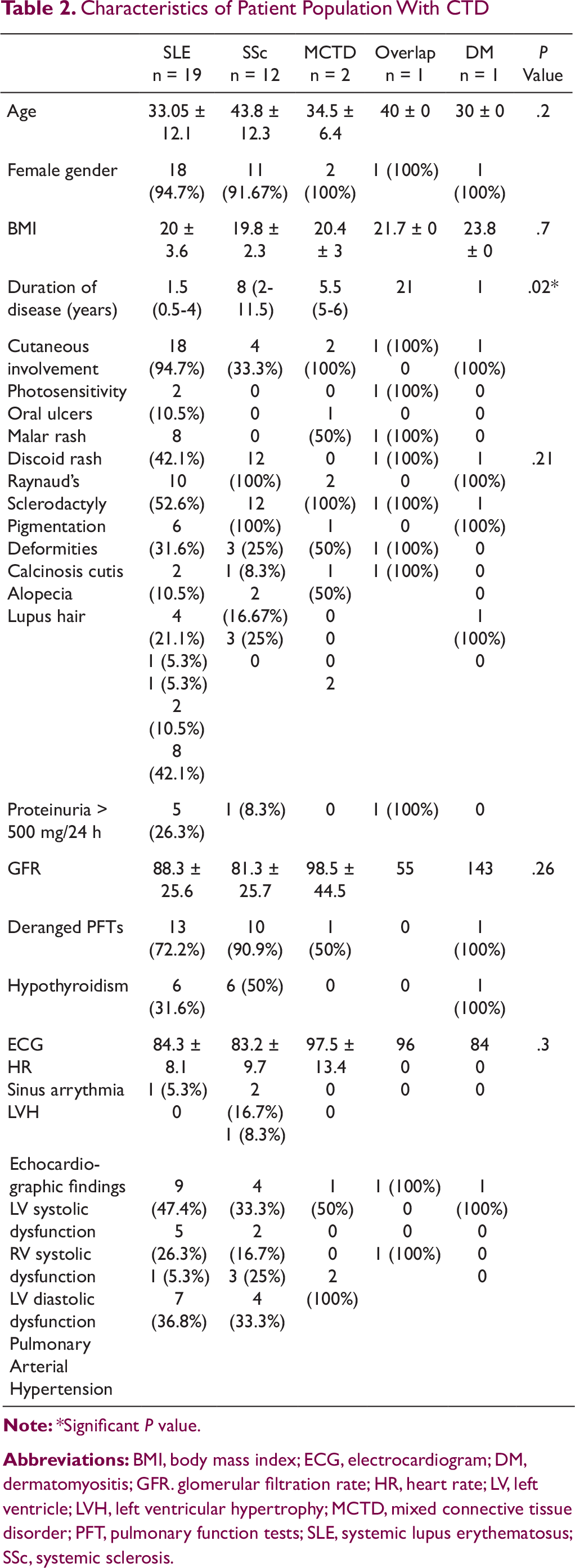
Characteristics of Patient Population With CTD
Pulmonary involvement was assessed by pulmonary function testing which revealed restrictive pattern in 25 (78.1%) patients (Table 1). Laboratory parameters were comparable between CTD group and the control group except for acute phase reactant like erythrocyte sedimentation ratio (ESR), which was significantly higher in the CTD group (P = .0001). The lipid profile was comparable in both the groups except serum triglyceride level, which was observed to be higher in the CTD group as compared to controls (P = .003). Deranged LFTs were more commonly observed in the CTD group (40% vs 2.9%, P < .0001).
Cardiac Abnormalities
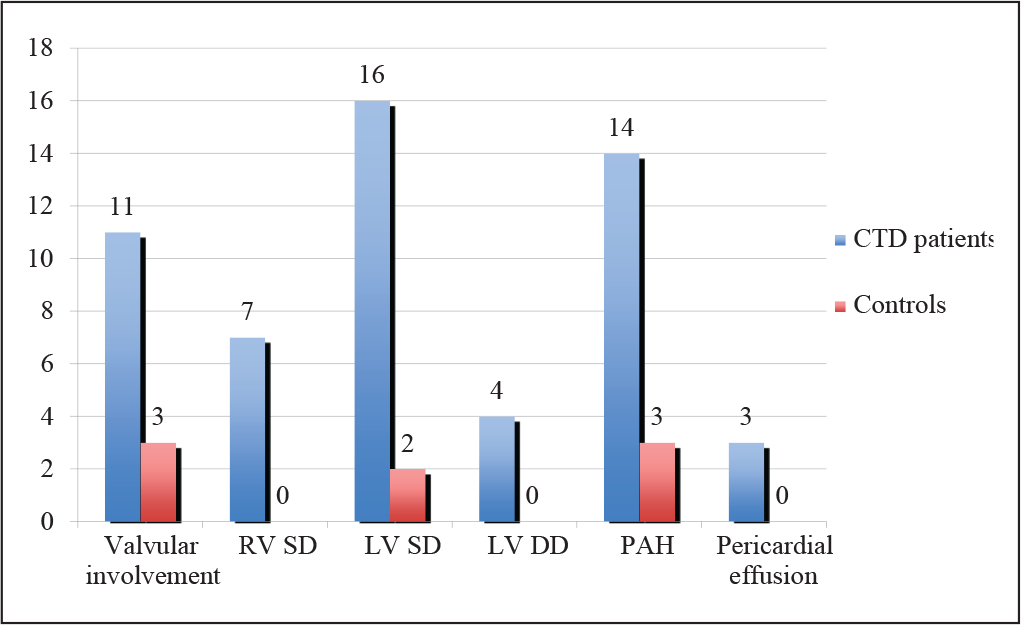
Cardiac involvement was seen in 25 (71.4%) patients in one or the other form (Figure 2).
Overall Cardiac Involvement in Cases and Controls
ECG Abnormalities
12 lead ECG was found to be normal in almost all the patients. The heart rate was observed to be more in the CTD group with a mean (+standard deviation) of 85 ± 9.2 as compared to 83.7 ± 5.1 in the control group (P = .47). LV hypertrophy was observed in only 1 patient.
Echocardiographic Abnormalities
Echocardiographic evaluation revealed abnormalities in overall 25 (71.4%) patients and 5 (14.2%) controls (P = .0001).
Left Ventricular Systolic Dysfunction
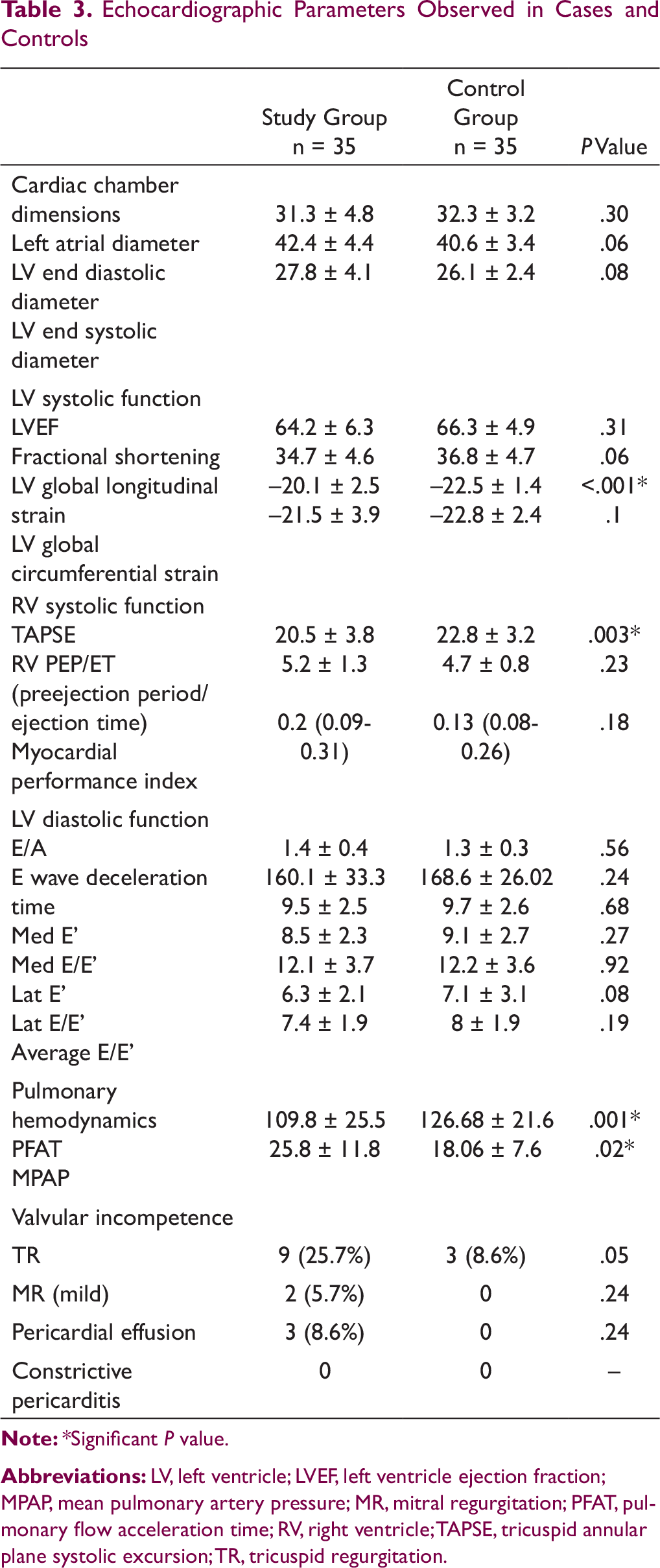
Echocardiographic Parameters Observed in Cases and Controls
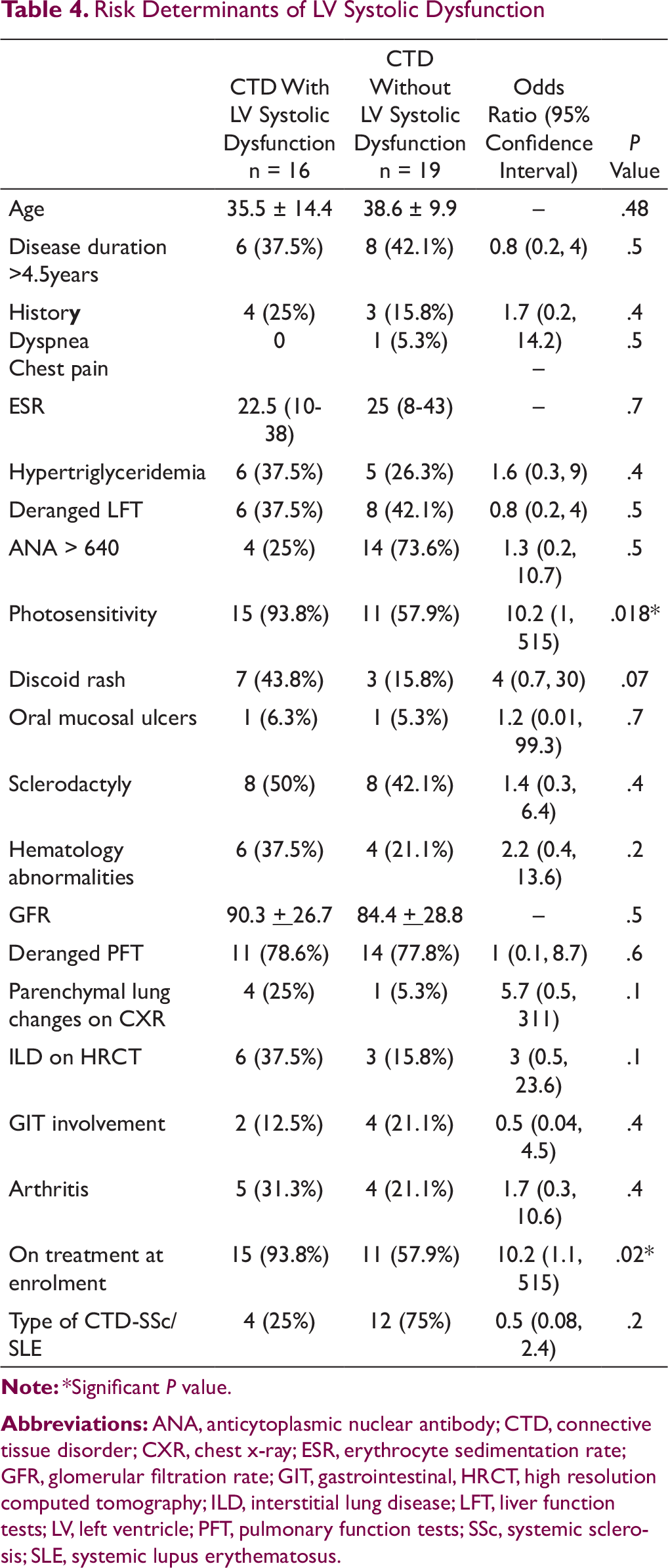
Risk Determinants of LV Systolic Dysfunction
Left Ventricular Diastolic Dysfunction
The mean value of medial E’ was 9.5 ± 2.5 in CTD patients and 9.7 ± 2.6 in control group (P = .68). Abnormal values of medial E’ were seen in 6 (17.1%) patients. Lateral E’ had a mean of 12.1 ± 3.7 in patients and 12.2 ± 3.6 in controls (P = .9). Abnormal lateral E’ values were seen in 7 (20%) patients. Average E/E’ ratio had a mean of 7.4 ± 1.9 in CTD patients and 8 ± 1.9 in controls (P = .2). The prevalence of LVDD was estimated to be 11.4% (n = 4) in the present study as per the standard guidelines followed. These included 3 patients of SSc and 1 patient of SLE, but because of the small sample size, risk determinants were not assessed.
Right Ventricular Systolic Dysfunction
The abnormal values for TAPSE and MPI were seen in 5 (14.3%) and 2 (5.7%) patients respectively. Presence of any of the above constituted RVSD. Hence, a prevalence of 20% (n = 7) was observed in the present study. The mean values of TAPSE were lower in CTD patients (mean of 20.5 ± 3.8) as compared to 22.8 ± 3.2 in controls (P = .0079). RV PEP was also observed to be significantly lower in cases as compared to controls (60 ± 11.5 vs 66.2 ± 9.1, P = .01). There was a trend of low values of ET with a mean of 297.3 ± 37.2 among CTD patients as compared to controls (306.3 ± 26.2) but the difference was not statistically significant (P = .07). MPI was more in CTD patients as compared to controls [0.2 (0.09, 0.31 vs 0.13 (0.08, 0.26)], but the difference was statistically insignificant (P = .18).
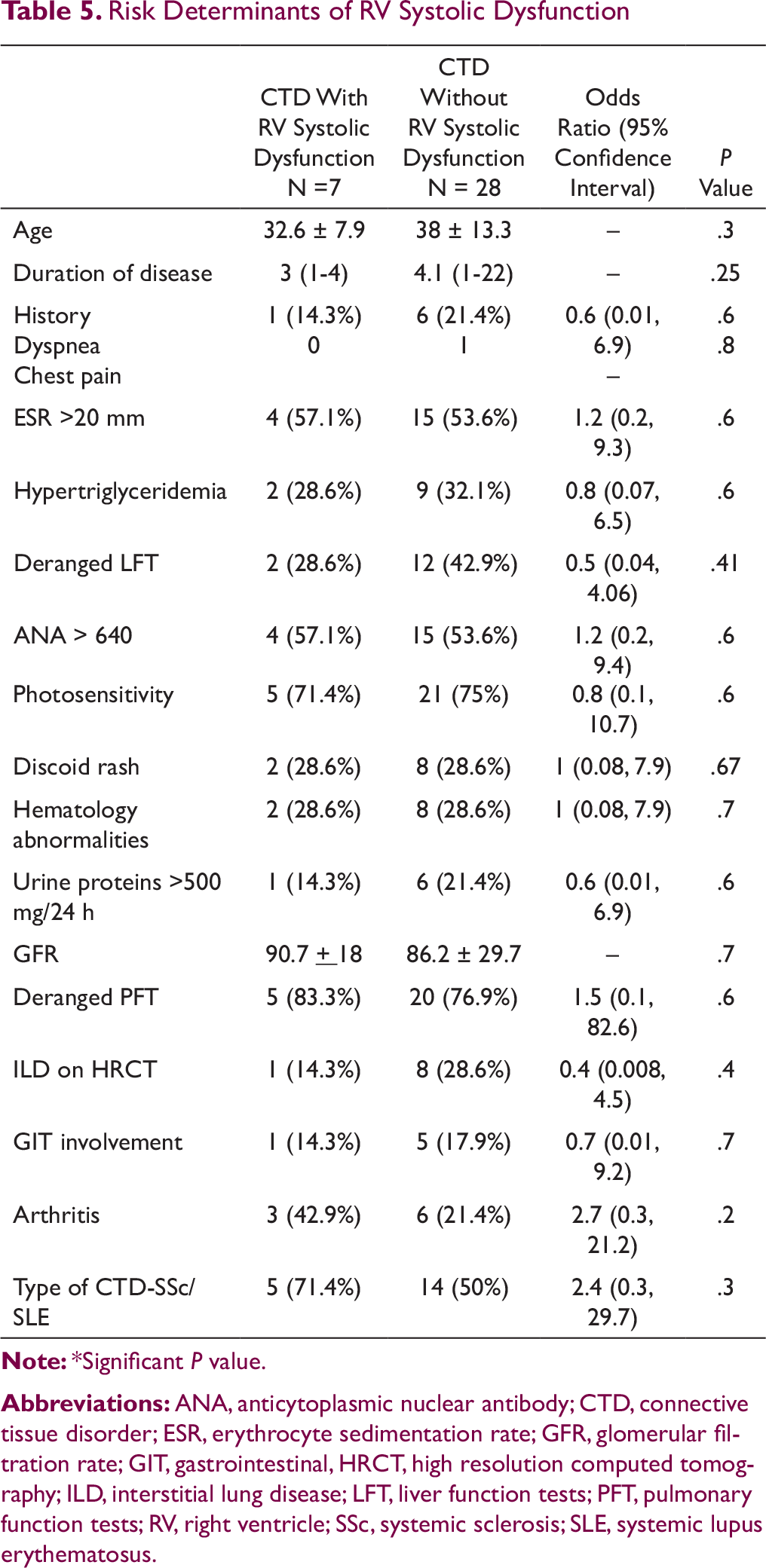
Risk Determinants of RV Systolic Dysfunction
Other Cardiovascular Involvement
Pulmonary hypertension was found in 14 (40%) patients of CTD. MPAP values were significantly higher in patients with a mean of 25.8 ± 11.76 mm Hg as compared to controls with a P value of .015. Pulmonary flow acceleration time also showed statistically significant lower values than controls with a P value of .0038 (Table 3). Valvular abnormalities were seen in 11 (31.4%) patients. Quantifying, 8 of them had trivial tricuspid regurgitation (TR) and 1 had mild TR. Even 3 controls manifested trivial TR and difference was not found to be statistically significant with a P value of .05. 2 (5.7%) patients had mild mitral regurgitation. There was no aortic valve involvement or Libman-Sacks vegetations. Pericardial effusion was found in 3 (8.6%) patients, but it was mild. All patients were asymptomatic with no evidence of chest pain, hemodynamic compromise, and pericarditis or cardiac tamponade.
Discussion
The structural damage of myocardium, pericardium, and valves can be mediated by immunoinflammatory injury as an autoimmune response. Therefore, patients with CTD with evidence of systemic inflammatory state are likely to have involvement of the cardiovascular system.13, 14 However, there are no case control prospective studies from an Indian population demonstrating the same.
In the present study involving 35 CTD patients and their age- and sex-matched controls, we have investigated the cardiac involvement in patients with CTDs primarily constituted by SLE and SSc patients who presented mainly with cutaneous manifestations. In the present study population of CTD, there were no patients of RhA, Sjögren’s syndrome, and PM. In brief, overall 25 (71.4%) patients had cardiac involvement in the form of structural and functional abnormalities. The systolic dysfunction (overt and/or subclinical) of LV and RV was observed in 16 (45.7%) and 7 (20%) patients, respectively, and diastolic dysfunction of left ventricle in 4 (11.4%) patients. The valvular incompetence of tricuspid and mitral valves was recorded in 9 (25.7%) and 2 (5.7%) patients, respectively.
Overall, both traditional and nontraditional risk factors for cardiovascular involvement have been associated with CTD. Traditional risk factors include hypertension, diabetes mellitus, dyslipidemia, male gender, metabolic syndrome, obesity, smoking, advanced age, menopausal status, family history of cardiovascular disease, hormone replacement therapy, and hyperhomocysteinemia. 15 Nontraditional factors include polyautoimmunity, increased ESR and C-reactive protein, higher disease activity, organ damage, longer duration of disease, medication, long-term steroid therapy, and renal involvement. 15 In the present study, we had excluded all patients who were smokers, had hypertension and diabetes, and who were aged >60 years, and we had predominantly female patients (94.6%), so as to evaluate the unerring prevalence of cardiac involvement among CTD patients. Among different subsets of CTD population, we observed higher prevalence of ventricular dysfunction among patients of SLE, but this association of CTD subtype with ventricular dysfunction could not be established statistically.
Wang et al 2 reported LV systolic dysfunction in a retrospective case control study of 436 patients of CTD and 436 controls, in 42.4% of patients. However, the criteria used for defining myocardial function limitation were based on the presence of ventricular dilatation, regional wall motion abnormalities and depressed LVEF. Strain imaging was not used. Similarly many other investigators16, 17 have evaluated LVSD in heterogeneous population of CTD and reported depressed systolic function compared to healthy controls. However, they have not reported the prevalent clinical and subclinical systolic dysfunctions. In the present study, overt LV systolic dysfunction was observed in only 3 (8.6%) CTD patients, while subclinical LV systolic dysfunction was recorded in 13 (37.1%) patients by strain imaging. Previously, Spethmann et al 18 also detected subclinical LV systolic dysfunction using strain imaging in a case-control study of 22 patients of SSc and reported a prevalence of 40.9%. Our data demonstrate the utility of strain imaging in early detection of LV dysfunction (before it is clinically evident) in patients with CTD.
In the present study, we found statistically significant association of photosensitivity and treatment status, ie, high dose of long duration steroid therapy at the time of enrollment with LVSD. Discoid rash was also significant on univariate analysis. Previous studies have observed disease duration as a determinant for LVSD, 14 but none of the previous studies have reported photosensitivity and discoid rash as significant determinants of cardiac involvement in CTD. This generates curiosity but there is need for further larger studies to validate and find the possible explanation behind this association.
Systolic functions of the right ventricle are also affected in CTD patients. Karna et al 19 have reported significantly raised MPI values in the patient group in comparison to controls (0.54 + 0.26 vs 0.35 + 0.07, P < .001), suggesting overall diminished right ventricular performance in the patient group. The present study also recorded higher values of MPI among patients of CTD. Buss et al 14 reported significantly lower values of TAPSE among CTD population similar to our study. RVSD was prevalent in 20% (n = 7) of the CTD patients in the present study, but no statistically significant determinant of RVSD was recorded, possibly because of the small sample size of CTD patients with RV dysfunction. Thus, future studies with large sample size are required to evaluate the risk determinants.
Various case-control studies have observed deranged diastolic functions in patients with CTD as compared to controls;2, 14, 16 hence, diastolic dysfunction is a known cardiac manifestation of CTD. LV diastolic dysfunction was observed in 11.4% cases in the present study, which was comparable to the prevalence of 12% reported by Kini et al. 20 However, methods for evaluating dysfunction were not described, and hence, the data of these 2 studies cannot be compared. Previous studies have reported association of aging and disease duration with type 1 and type 2 diastolic dysfunction, respectively, 21 whereas in the present study, because of very small sample of patients (n = 4) with LVDD, determinants were not assessed.
Pericardial disorders occurring in CTDs are not uncommon and may present as pericarditis with or without effusion. Cardiac tamponade and constrictive pericarditis are possible but rare complications. Pericardial effusion was documented in only 3 (8.6%) patients in the present study, but was of mild nature. Wang et al 2 reported 12.5% prevalence in a large heterogeneous sample of CTD population whereas many other investigators4, 5, 20 have reported higher prevalence of pericardial effusion ranging from 18.5% to 39%. However, all these studies included exclusively SLE patients with larger sample size and active disease.
Limitations
Because of the single center setting, potential center-specific bias cannot be ruled out. However, our center is a tertiary care unit and caters to patients referred from different parts of the state. The overall CTD group and in particular MCTD, DM, and overlap subgroups are small. There were no patients of RhA, primary Sjögren’s syndrome, and PM, and hence, our results cannot be extrapolated to whole CTD population. We enrolled all patients coming to the dermatology department with primarily cutaneous involvement; hence, patients with severe systemic features presenting to medical out-patient department may have been missed leading to an inherent selection bias. The small sample size of study population is the major limitation of this study; however, the results can be helpful in generating new hypothesis and can pave way for future studies with larger sample size and longer follow-up duration. Another important limitation of the present study was the use of a cut-off value of <–20% for global longitudinal strain (GLS), although the current practice is to take a cut-off value of <–15%.22, 23 The normal values for GLS depend on the definition of the measurement position in the myocardium, the vendor, and the version of the analysis software, resulting in considerable heterogeneity in the published literature.8, 23 Various authors have previously suggested that the expected value of LV GLS in a healthy individual is around –20% and any value of LV GLS less negative than –20% could be considered pathological. 23
Conclusion
Cardiovascular involvement occurs in a substantial number of CTD patients (71.4%), most of them being asymptomatic. The subclinical LV systolic dysfunction was the commonest manifestation, which was detected using strain imaging. Patients with photosensitivity and long duration of steroid therapy had higher prevalence of LV systolic dysfunction. Pulmonary hypertension was found in nearly one-third patients of CTD. Significant cardiac involvement in the form of overt LV systolic dysfunction and mild valvular incompetence was documented in very few CTD patients. Furthermore, long-term studies enrolling higher number of CTD patients are needed to validate these findings. Such data are needed to device screening strategies against cardiovascular complications in CTD patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.