
Abstract

The global pandemic of COVID-19 grapples India, which has recorded over eight million cases, while the global cases are surging. Health care workers are at high risk of infection and the Indian Council of Medical Research has recommended prophylaxis with Hydroxychlrorquine (HCQ) for persons with a high risk of exposure. Experience with HCQ in other approved conditions shows that this medication is safe for most of the individuals. However, it can cause a few adverse cardiac effects like QT prolongation on electrocardiogram (ECG) and subsequent life-threatening ventricular arrhythmias.
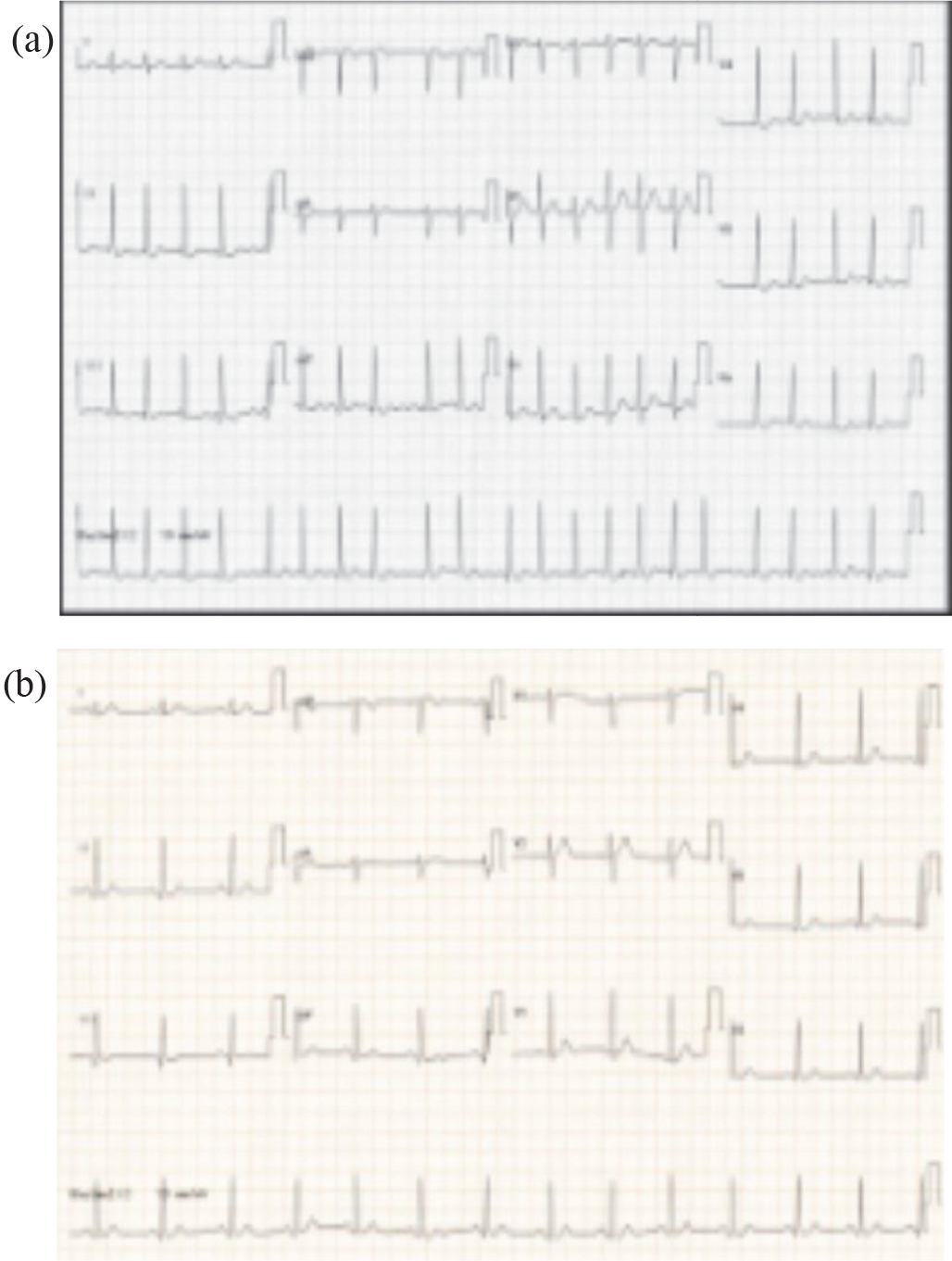
A 30-year-old surgeon, without any previous illness or risk factors, taking care of patients during the present pandemic, had taken 800 mg of HCQ as the first dose of prophylaxis. After 5 days, he had sudden onset palpitations for which he presented to the emergency. He did not have any previous symptoms. ECG was suggestive of atrial fibrillation with a high ventricular rate (Figure 1a). The echocardiogram ruled out a structural abnormality of the heart. The rhythm reverted to sinus spontaneously when the treatment was being contemplated; he was advised to stop further doses of HCQ and to be in close follow-up without any episodes after 2 months of the index event. The ECG in sinus rhythm was normal, with a corrected QT interval of 380 msec (Figure 1b).
(a) Electrocardiogram showing Atrial Fibrillation With a Ventricular Rate Around 126 bpm (b) Normal Electrocardiogram After Reversion to Sinus Rhythm
Scenario raises some interesting questions which we thought would interest the readers. HCQ, whether it is responsible for AF, is one of them. It is not a drug usually implicated in the causation of this arrhythmia, 1 but it can slow the atrial rate by modifying the If channel in the sinus node. 2 This bradycardia, in addition to vagal overactivity in young athletic individuals, may precipitate AF is not known. Another uncertainty is the acute management, as the drugs to treat AF may have unfavorable interactions with HCQ. For pharmacological cardioversion class 1A (procainamide and quinidine), class 1C (flecainide and propafenone), and class 3 (amiodarone, sotalol, and ibutilide) agents are used; all these can cause QT prolongation when coadministered with HCQ and should be avoided. Rate control should be the ideal approach with either beta-blockers (atenolol and metoprolol) or calcium channel blockers (diltiazem and verapamil), which do not interact with HCQ.
As more health care workers are receiving HCQ, the adverse effects of this drug are expected to be commonly encountered. We should keep a vigil on them and they should be promptly reported to the monitoring agencies.
Sincerely,
Sreekanth Yerram