
Abstract
Nocardia farcinia endocarditis is an extremely rare phenomenon. It is an opportunistic ubiquitously present pathogen in the environment. Here, we present an unusual case of septic embolism with infective endocarditis due to Nocardia spp. in a 55-year-old chronic alcoholic male. Radiological imaging techniques and microbiological investigations helped in the timely diagnosis. Timely institution of treatment based on sensitivity results resulted in favorable outcome in the patient.
Introduction
Infective endocarditis (IE) is a common pathology usually presenting with fever and a new or changing cardiac murmur. Diagnosis is usually based on the presence of continuous bacteremia and the presence of vegetation on gross examination or echocardiography or histological examination of the removed valve. According to the Duke’s modified criteria, for the diagnosis of IE is definite (a) when a micro organism is demonstrated by culture or histologic testing in vegetation, an embolism, or an intracardiac abscess; (b) when active endocarditis is confirmed by histologic examination of the vegetation or intracardiac abscess; or (c) in the presence of two major clinical criteria, one major and three minor criteria, or five minor criteria. 1
Nocardia is a soil-borne ubiquitous aerobic actinomycete. It is a Gram-positive branching filamentous bacillus which is weakly acid fast. 2 Nocardiosis mainly affects immunocompromised patients and very rarely immunocompetent ones. 3 N. asteroides complex and N. brasiliensis are the most common species causing majority of the cases. Mycetoma is the most common cutaneous and lymphocutaneous manifestation caused by N. brasiliensis in the tropical climate. Pulmonary infections are also prevalent in the temperate climate caused by N. asteroides. 3 The former N. asteroides complex has been separated into six susceptibility patterns: N. abscessus (formerly N. asteroides type I), N. brevicatena/paucivorans complex (type II), N. cyriacigeorgica (type VI), Nocardia farcinica (type V), N. nova complex that includes N. africana, N. kruczakiae, N. nova, and N. veterana (type III), and N. wallacei (type IV). 4 N. farcinica is particularly important to distinguish since it has increased virulence and differs in its antimicrobial susceptibility test results and its epidemiology. Cases of infective endocarditis due to these organisms are an extremely rare phenomenon.
This case report highlights the importance of this very rare opportunistic pathogen in causing infective endocarditis in today’s changing scenario.
Case Report
A 54-year-old male working as a daily wage worker presented to our outpatient department with bilateral lower limb weakness and pain since last one month. The pain radiated from the thighs to lower down the legs. He also complained of a severe intermittent frontal headache for last 15 days, which was nonradiating in nature and not relieved by normally available over the counter pain killers. The episodes of headache were occasionally accompanied by diplopia and photophobia with mild neck stiffness. Other chief complaints were nausea, vomiting, and a low-grade intermittent fever The condition became worse 7 days ago when he felt weakness in his both upper limbs too and was not able to walk or stand by himself. At the time of presentation, he was on stretcher and could barely lift his hands. He was a chronic alcoholic since last 10 years and was diagnosed with liver cirrhosis 8 months back. Liver transplant was advised to the patient at that time. He had no other medical problems and no previous surgical interventions. He had no significant travel history.
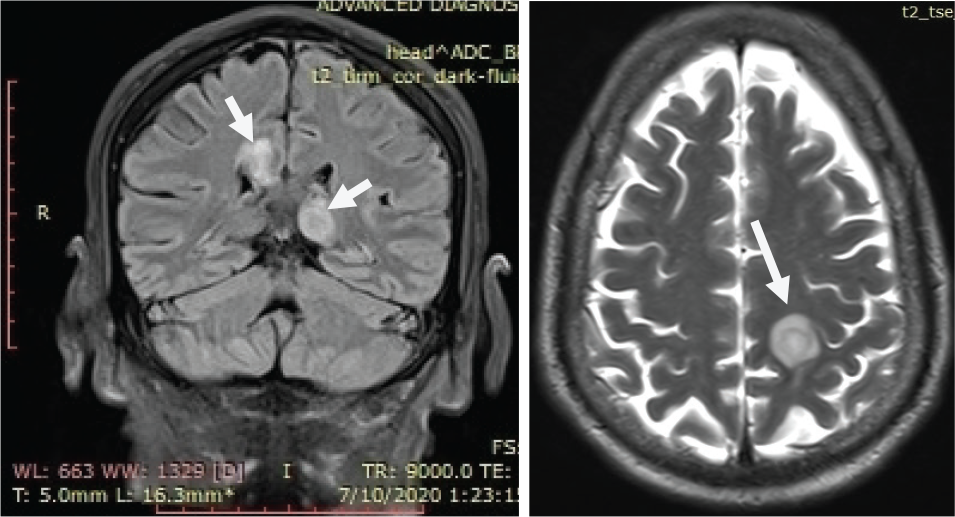
Routine blood examinations were normal except mild elevation of liver transaminases and hyperbilirubinemia. Rest of the serological investigations including Hepatitis, HIV, and EBV were negative. Chest X-ray on admission was unremarkable. Computer tomography (CT) of the brain was planned for further evaluation. It (Figures 1 and 2) revealed multiple intra axial hyperdense lesions with surrounding vasogenic edema in the frontal, parietal, and temporal lobes. Presence of several lesions at the junction of gray and white matter suggested hematogenous spread. Transthoracic echocardiography also revealed a mass on the anterior leaflet of the mitral valve, 1.6 × 0.82 cm in size. Mild mitral valve regurgitation was noted.
(Left) MRI of Brain and (Right) MRI of Brain with Contrast: Showing Multiple Intracranial Rim Enhancing Lesions with Central Restricted Diffusion and Surrounding Vasogenic Edema in the Brain
(Left) Zeihl-Neelsen Stain and (Right) Gram Stain: Showing Multiple Filamentous Bacteria with Branching at Right Angles Resembling Nocardia spp.
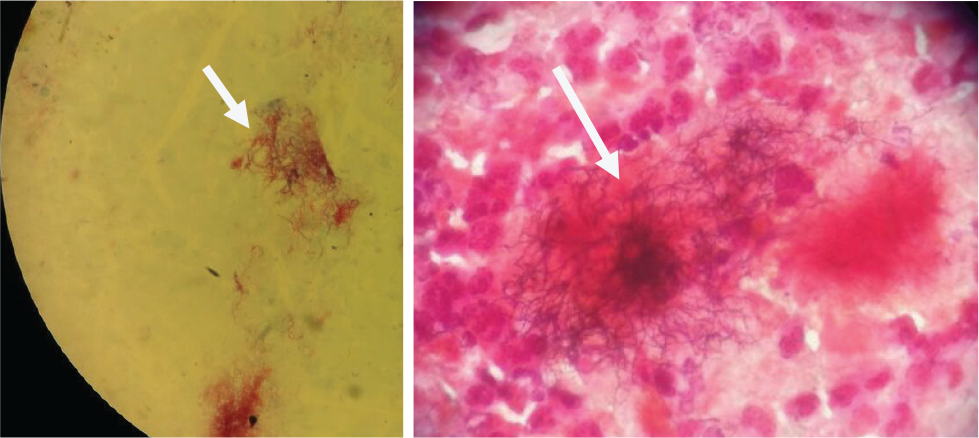
Subsequently, blood cultures were sent to the microbiology laboratory in a pair of BacT/Alert bottles. BacT/Alert detection system flagged positive after 72 h of incubation and bottles were further processed with routine Gram staining and culture on routine media. Gram stain revealed multiple Gram-positive rods with branching at right angles resembling the Nocardia spp. Ziehl-Neelsen stain also showed multiple weakly acid-fast bacilli. For further identification, routine biochemical tests were also put up like growth on tryptone glucose yeast agar at 45° C for 1 day, production of: 14-day arylsulfatase, nitrate reductase, and urease; hydrolysis of adenine, casein, esculin, hypoxanthine, tyrosine, and xanthine; and utilization of acetamide, citrate, l-rhamnose and d-sorbitol. Final speciation was done using the matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF-MS). Final ID of the organism was identified as N. farcinica. Antibiotic susceptibility testing was done using the VITEK-2 system. The isolate was sensitive to aminoglycosides (Gentamicin, Amikacin), trimethoprim-sulphamethoxazole (TMP-SMX), imipenem, linezolid and was resistant to ceftriaxone and other cephalosporins.
The patient was started on the combination therapy of TMP-SMX, amikacin, imipenem with linezolid for about 2 weeks. On regular visits, the patient reported some partial relief in his symptoms. Then the antibiotic regimen was altered to TMP-SMX, amikacin, and imipenem. He finally underwent valve replacement surgery after 15 days and was discharged in a good general condition after one and a half month with a course of antibiotics for further 3 months.
Discussion
Literature search shows very scarce case reports of IE due to Nocardia sp. Infections due to nocardial infections affect mostly immunocompromised patients but rare cases in immunocompetent are also noted. 5 The most common manifestations of Nocardia include pulmonary and skin infections. Pulmonary infections are the most common (43%). Disseminated or extrapulmonary manifestations are seen frequently as septic embolus to the brain or CNS infections/abscesses comprising 30% and less frequently as wound infections 15%. In most of the cases of IE due to nocardia, patients had prior valvular heart disease and subsequently went for valve replacement surgery.6, 7 An increase in these infections can also be attributed to the increase in numbers of heart and liver related transplant procedures. 8 A case of IE and brain abscess has also been reported by Nocardia kroppenstedtii sp. 9 It was the first reported case of infectious endocarditis and brain abscess. Nocardia kroppenstedtii resembles in 99.8% of its genome with N. farcinica. 10
The frequency of Nocardia in different countries varies from 0% to 20% with a mean of 2.8%. 11 In the current scenario, the overall incidence of nocardia infection has reduced due to the introduction of chemoprophylaxis with TMP-SMX in solid organ transplant recipients. One center from Stanford University reported a reduction in incidence of Nocardia infection from 13% to 4.2%. 7
Infection due to N. farcinia is an extremely rare phenomenon and to the best of my knowledge no such case reports of septic embolism have been published in the past. N. farcinica is rarely isolated from blood and urine.10, 11 Some cases of isolation of this rare pathogen from brain infections and abscesses have been reported.12, 13 Disseminated Nocardiosis poses a challenge in diagnosis as it may mimic a variety of bacterial as well as fungal infections. 14 High index of suspicion is required on the part of clinicians as well as the microbiologists in getting to a definitive diagnosis on time. Our patient was also diagnosed with liver cirrhosis and cirrhosis in itself is an immunocompromised state, 14 which raises the chances of infection by this opportunistic organism. In the appropriate clinical and laboratory setting, the diagnosis of Nocardia can be made easily by the demonstration of organisms in gram stain, Ziehl-Neelsen stain, culture, or tissue histology. 15 PCR can also be used for the rapid diagnosis of Nocardia, as the cultures take a longer time to grow. However, with the advent of newer molecular techniques like MALDI-TOF and VITEK-2, the diagnosis as well as antibiotic sensitivity testing take a lot lesser time and are very convenient too.
Current recommendations for empirical treatment of Nocardia infection are either TMP-SMX or other agents such as amikacin, imipenem or linezolid, and antibiotic adjustments as soon as the final sensitivity results arrive.16, 17 Empirical treatment with TMP-SMX along with carbapenems and Amoxiclav have been tried and resulted in successful outcomes in one such case series of 22 Nocardia cases. 18 Most of the Nocardia infections show susceptibility to TMP-SMX, moxifloxacin, linezolid, minocycline, and amikacin, and have variable susceptibility to ciprofloxacin and imipenem-cilastatin.18, 19, 20 CNS infections require a longer course of antibiotics for even up to 8 to 12 months as the mortality rate in these cases is also very high over 55%. 19 Combination regimens with TMP-SMX and carbapenem or cephalosporins are usually recommended in severe infections.21, 22 The patient in our case showed good response to antibiotics as per the sensitivity results and was later discharged after surgery in a good general condition .
Conclusion
Disseminated nocardiosis and septic embolism together is an extremely rare phenomenon in infective endocarditis patients. Ours is one such case report from north India and certainly draws attention toward the increasing infections due to this opportunistic pathogen. Systemic/disseminated nocardiosis should be dealt with utmost caution in both diagnosing and timely institution of therapy as per sensitivity results. Timely intervention in such cases usually results in favorable outcome in majority of the patients.
Ethical Considerations
Informed consent was obtained from the patient regarding the publication of images and clinical information in the journal. They were informed of the confidentiality of the data, however, the anonymity cannot be guaranteed.
Footnotes
Author’s Contribution
SS performed literature search, data analysis, and first draft of the manuscript and figures. USS contributed with the clinical radiograph images of the patient, literature search, and final draft of the manuscript.
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.