
Abstract
Tricuspid regurgitation (TR) is a highly prevalent echocardiographic finding in general population being present in almost 80% to 90% of them. However, TR is mild or functional rather than organic in majority of people. Significant TR was seen in 14.8% of adult men and 18.4% of adult women, respectively. Of all the significant TRs, approximately 8% to 10% are primary. Mild TR is benign but moderate-to-severe TR tends to progress and carries significant morbidity and mortality. Tricuspid valve disease is either primary or secondary (functional) in nature. Valve leaflets are predominantly diseased in primary TR, whereas annular dilatation is the main culprit in secondary TR. Of all the heart valves, tricuspid valve was the most neglected valve till a decade ago, though there was enough evidence to show that moderate to severe TR was not as benign as was assumed. With the availability of 2-dimensional echocardiography (2D echo) and transesophageal echocardiography, we are able to diagnose and determine the severity as well as etiology of TR. Although surgical therapy remains the gold standard for severe primary tricuspid valve disease, it continues to suffer from one of the highest morbidity and mortality rates among all cardiac valve-related surgeries even in the hands of experienced surgeons. For the same reason, majority of patients are not referred or subjected to surgical therapy. Therefore, there is an unmet need for less invasive and safer form of therapy to overcome this hurdle. So, several less-invasive and innovative technologies for treating patients with severe tricuspid valve disease at high surgical risk are being developed. Some of them have already been used for treatment of severe mitral regurgitation. They are being adopted for the treatment of severe TR. This review provides a comprehensive picture of newer guidelines and latest technologies and their impact on diagnosis and outcome of high-risk TV disease.
Keywords
Introduction
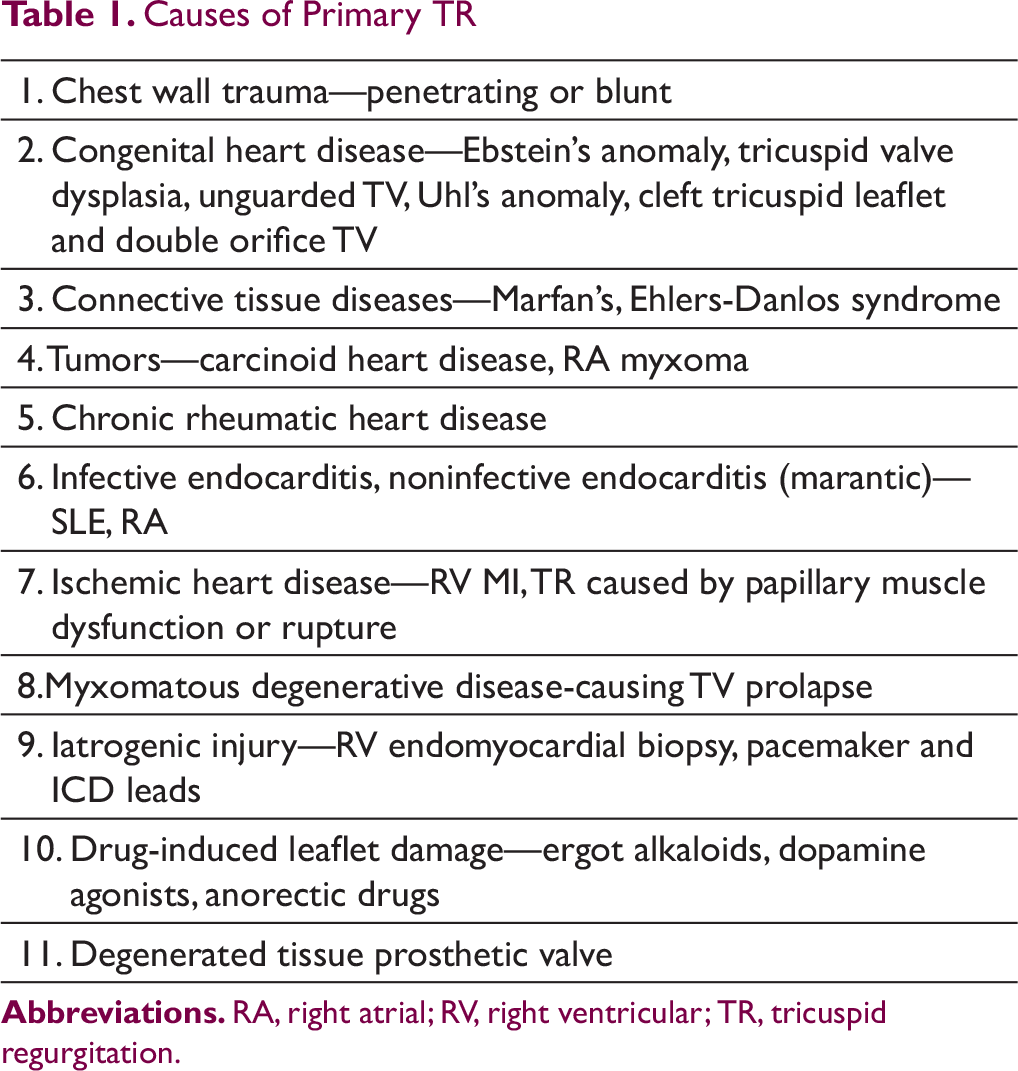
Causes of Primary TR
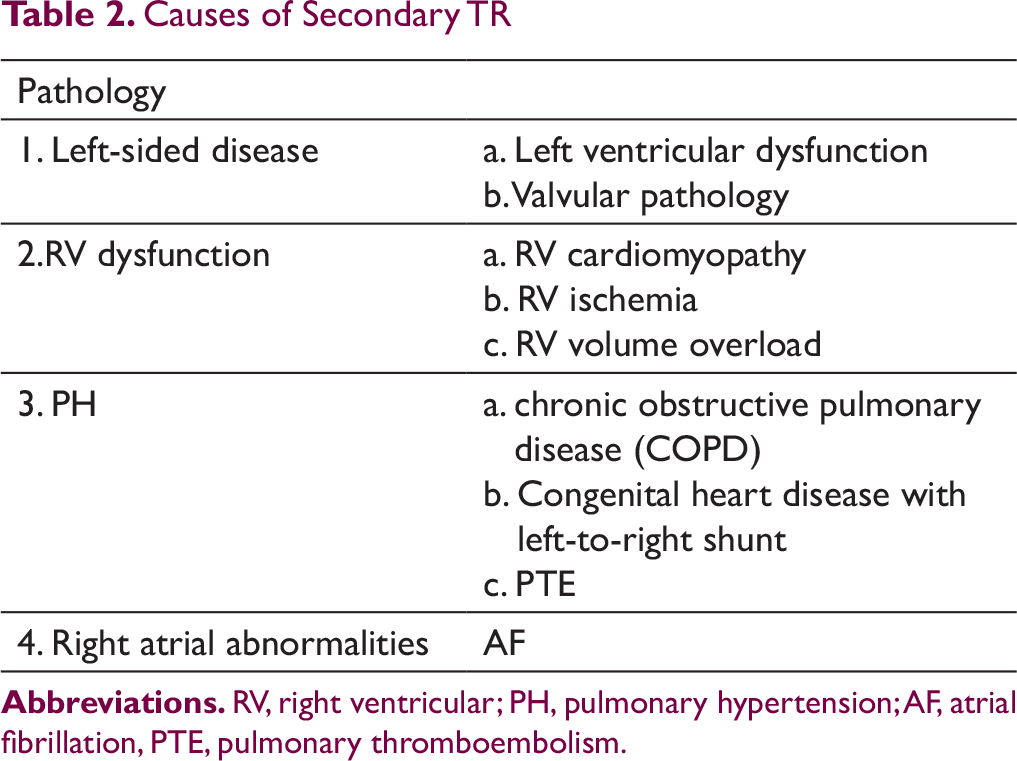
Causes of Secondary TR
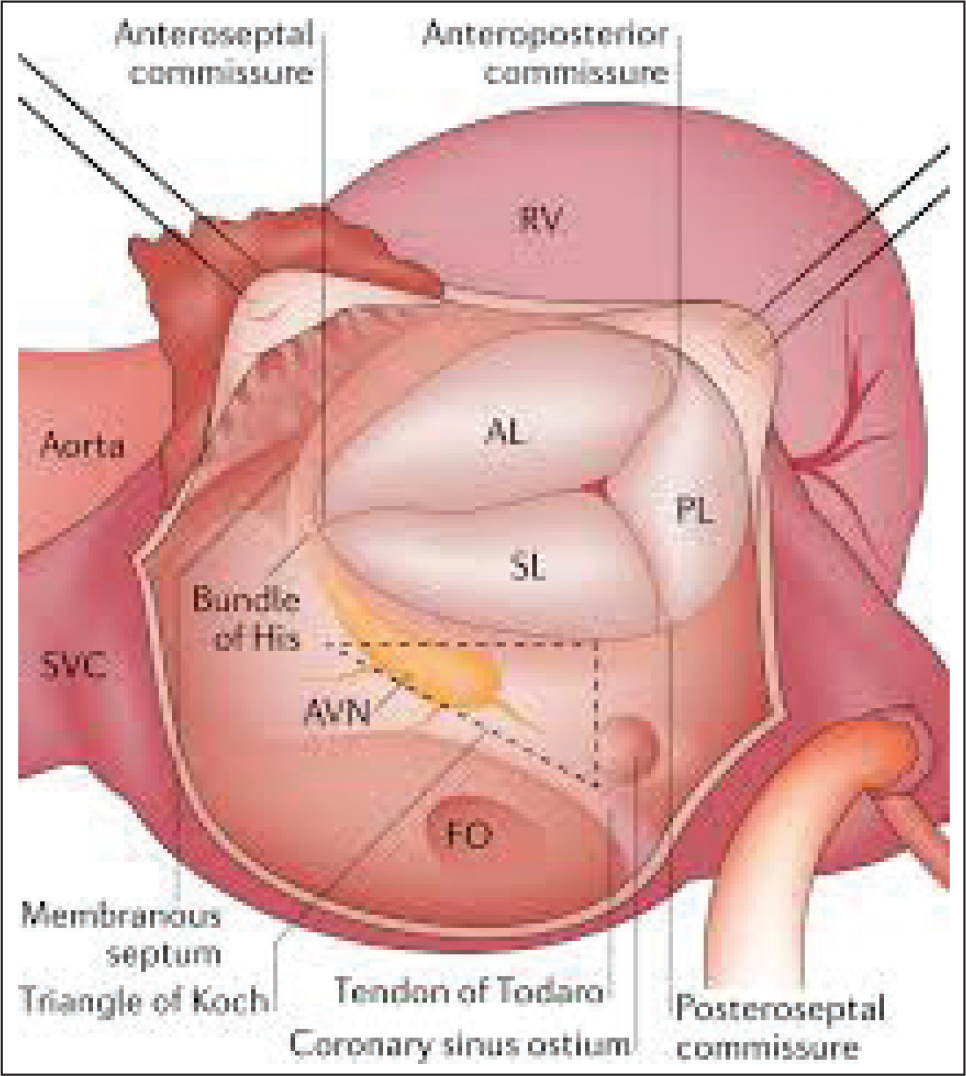
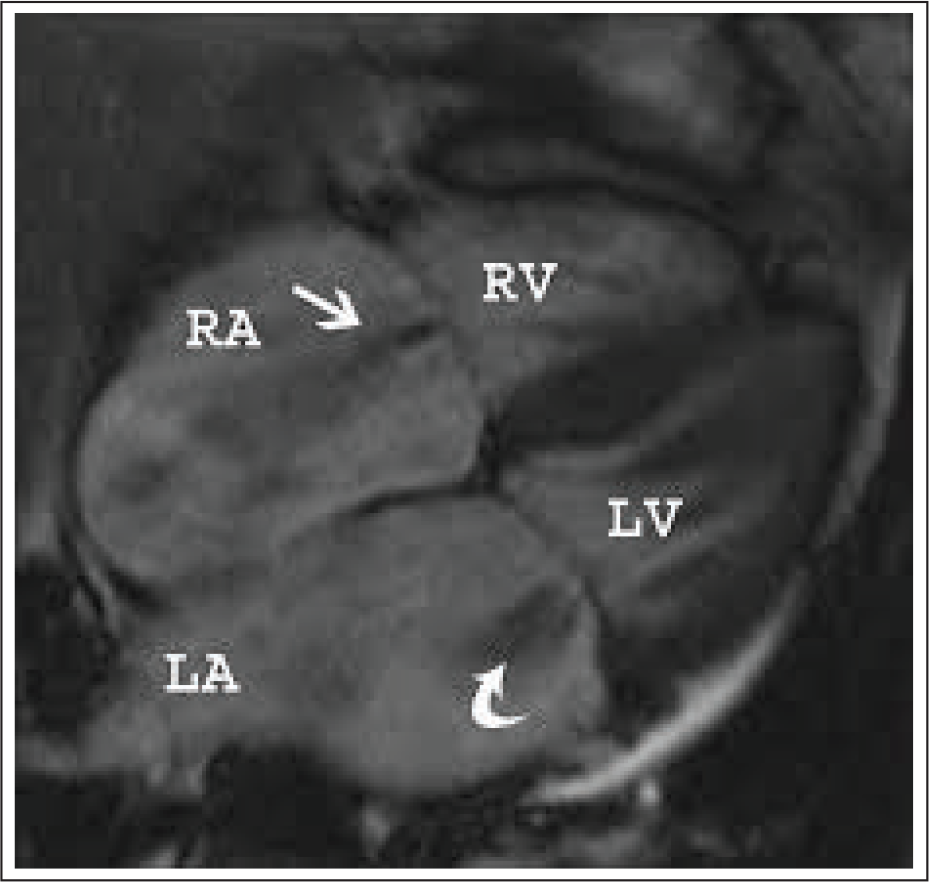
Tricuspid Valve (TV) Anatomy
TV has complex anatomy (Figure 1) warranting thorough assessment before contemplating surgical or interventional procedures. The TV is the largest of 4 valves with saddle-shaped annulus. The TV complex consists of three leaflets (anterior, posterior, and septal), chordae tendinae, 2 discrete papillary muscles, the fibrous tricuspid annulus (TA), and the RA and RV myocardium. Successful valve function depends on the integrity and coordination of these components. The anterior leaflet is the largest, whereas the posterior leaflet is notable for the presence of multiple scallops. The septal leaflet is the smallest and arises medially directly from the TA above the interventricular septum (IVS). The anterior papillary muscle provides chordae to Dthe posterior and anterior leaflets, and the medial papillary muscle provides chordae to the posterior and septal leaflets. The septal wall gives chordae to the anterior and septal leaflets. In addition, there may be accessory chordal attachments to the RV-free wall and the moderator band. These multiple chordal attachments are important mediators of TR, as they produce tethering and impair proper leaflet coaptation in the setting of RV dysfunction and dilatation. 4
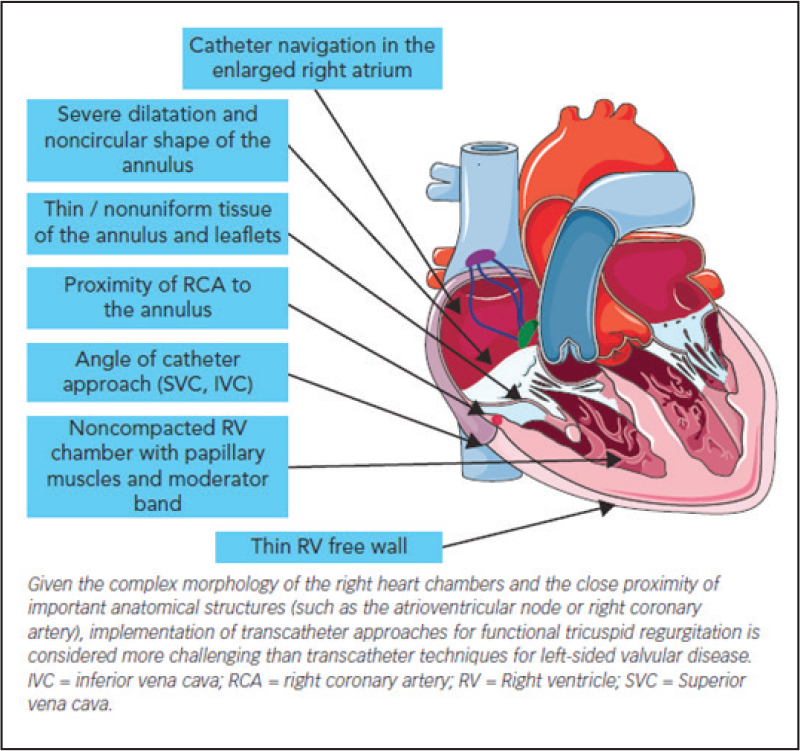
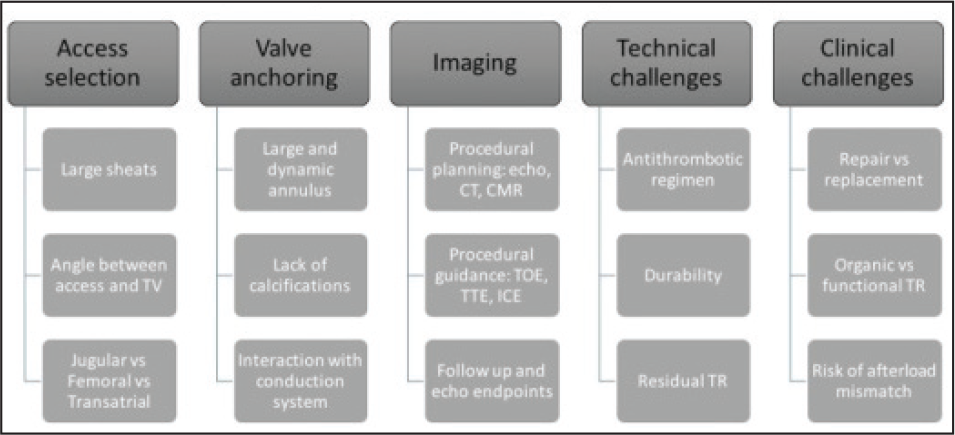
Noncalcified, fragile, and large dynamic annulus, trabeculated and thin-walled RV, unfavorable angle between TA and vena cavae (IVC and SVC) and proximity to AVN, IVC, and RCA pose challenges during surgery and transcatheter interventions (Figure 2).
Anatomical challenges in the development of Transcatheter techniques for functional TR. [Christian Besler, et al. Interventional Cardiology [London]. January 2017]
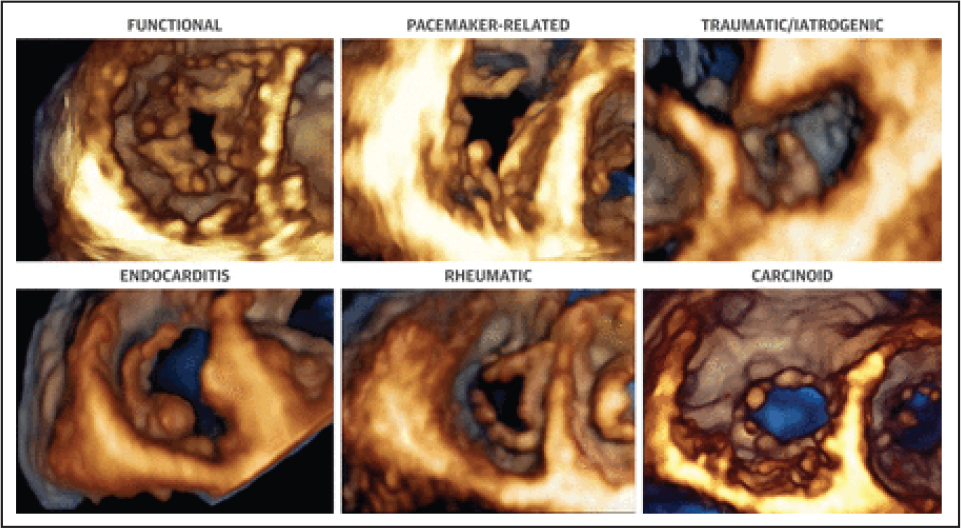
Evaluation
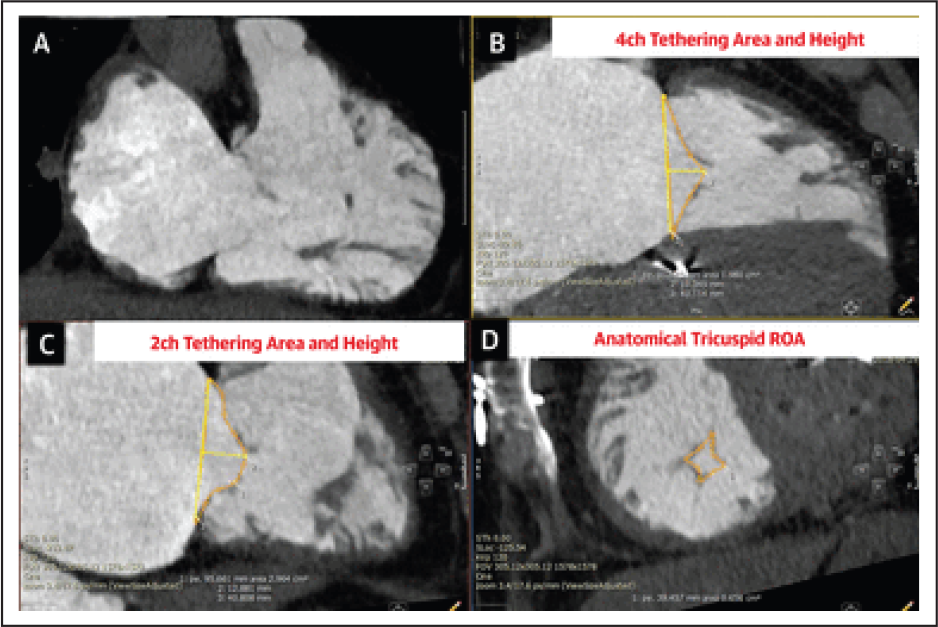
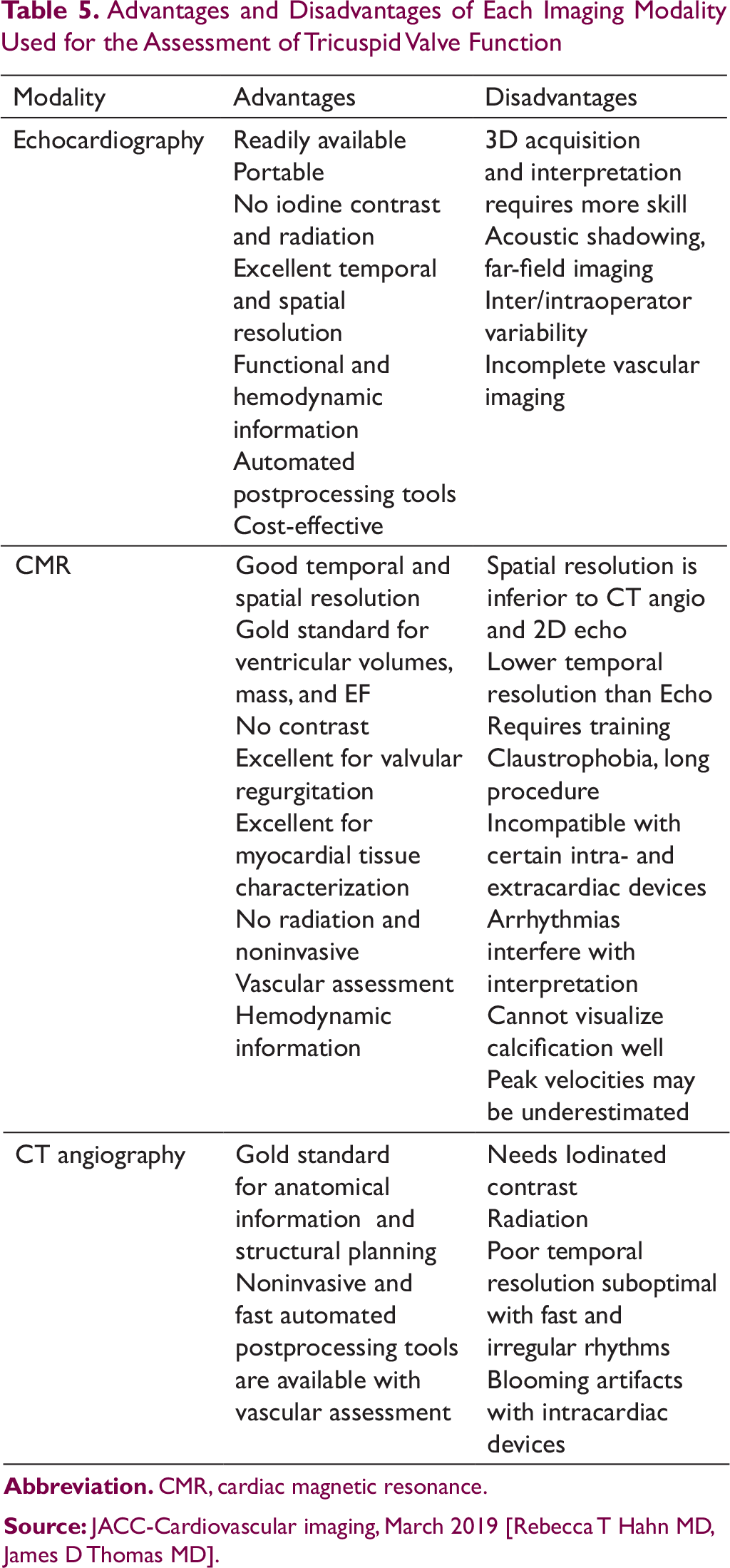
Imaging has a crucial role in the assessment of TV. Transthoracic and transesophageal echocardiogram (2-dimensional and three-dimensional), cardiac magnetic resonance (CMR) imaging, and multidetector computed tomography (MDCT) imaging play a pivotal role in identifying the cause, estimation of the degree of TR and assessment of anatomy of the valve and right ventricle. Above imaging modalities guide during surgical as well as transcatheter repair/replacement and also during follow-up after surgery and transcatheter intervention. Advantages and disadvantages of imaging techniques are as mentioned in Table 5.
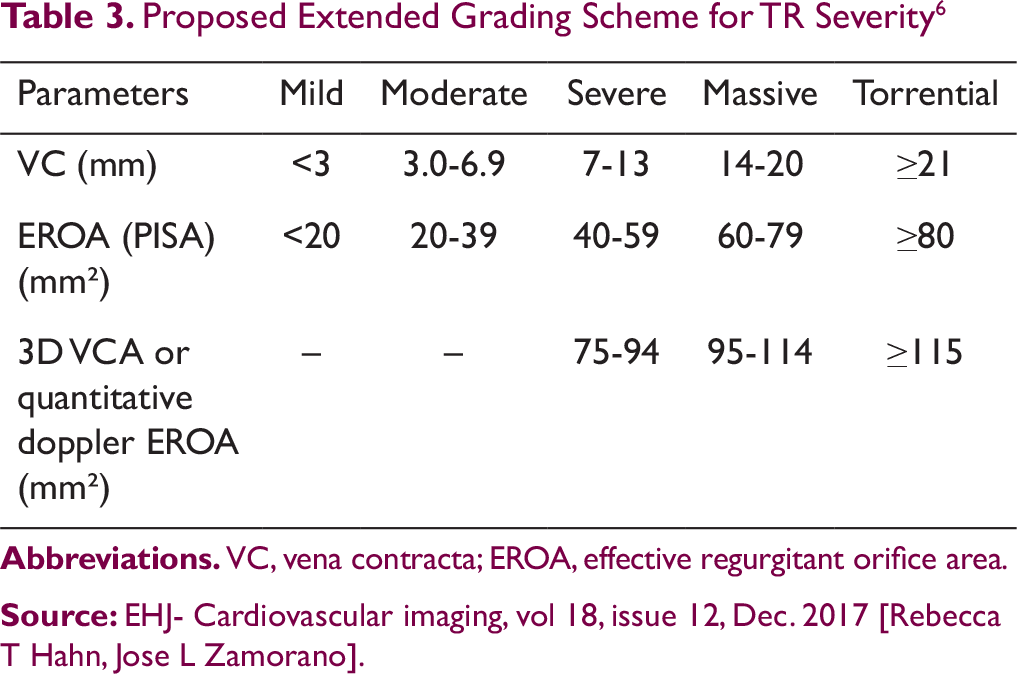
Proposed Extended Grading Scheme for TR Severity 6
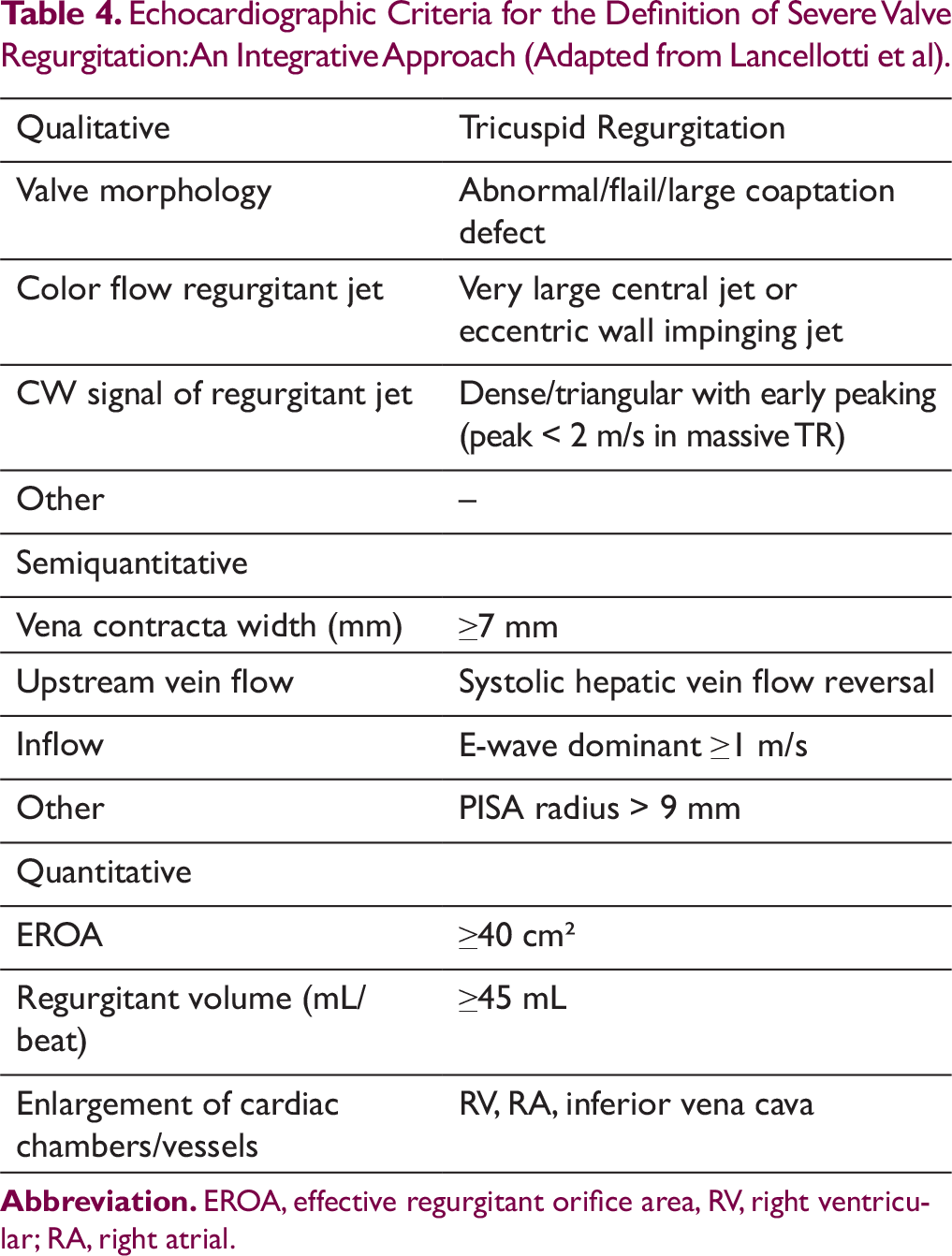
. Echocardiographic Criteria for the Definition of Severe Valve Regurgitation: An Integrative Approach (Adapted from Lancellotti et al).
Advantages and Disadvantages of Each Imaging Modality Used for the Assessment of Tricuspid Valve Function
Positron Emission Tomography (PET-CT)
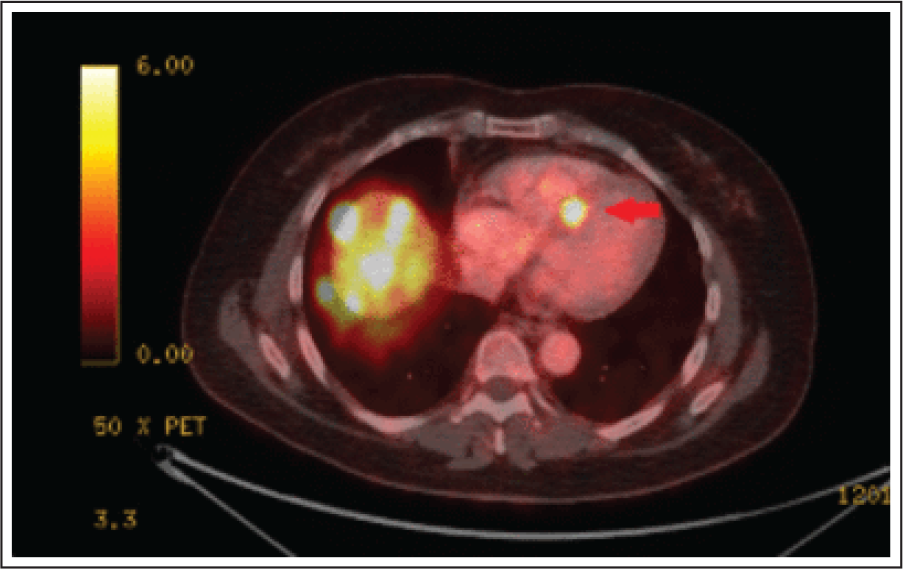
It has a limited role in assessment of TV with the exception of carcinoid syndrome. A hallmark of neuroendocrine tumors is their increased density of somatostatin receptors. PET takes advantage of this unique feature as somatostatin analogues labeled with radioactive substance (typically gallium-68) are avidly taken up by neuroendocrine neoplasms and are easily identifiable on PET scan. This is useful for identifying metastasis including myocardial metastasis in carcinoid heart disease (Figure 6). This method has shown to be >97% sensitive and 92% specific for the identification of metastatic neuroendocrine neoplasms. 7
Natural History and Prognosis
Increasing evidence suggests that clinically significant TR has a detrimental impact on long term clinical outcomes if left untreated. Moderate TR progressively worsens over a period of time, leading to irreversible RV dysfunction, heart failure, and death. Heart failure is responsible for 50% of deaths in severe TR. Mean years of survival from diagnosis of severe TR was 4.35 ± 3.66, and mean years of survival from onset of symptoms was 2.28 ± 1.40. 7 In a retrospective study of 5223 patients, after controlling LV EF, RV dilatation and dysfunction, and PAP, mortality increased with increasing severity of TR. The 1 year survival rate was 91.7% with no TR, 90.3% with mild TR, 78.9% with moderate TR and 63.9% with severe TR. Failure to refer the patient in time for surgery was the main reason for high surgical morbidity and mortality.
Management
Management of significant TR includes medical management, surgery and transcatheter interventional therapies. In patients with primary TR where valve leaflets are diseased, surgical repair or replacement is the gold standard. Transcatheter tricuspid valve interventions are mostly relevant to those patients with severely symptomatic secondary TR (FTR) who are high risk for surgery.
Medical Therapy
Combination of diuretics and mineralocorticoid receptor antagonists (IIa-C) is the most commonly used treatment to mitigate right-sided heart failure symptoms and signs. However, none of these measures should unnecessarily delay surgical intervention in deserved and suitable patients. Main obstacle to successful surgery in a significant number of patients is advanced disease due to late referral.
Surgical Management
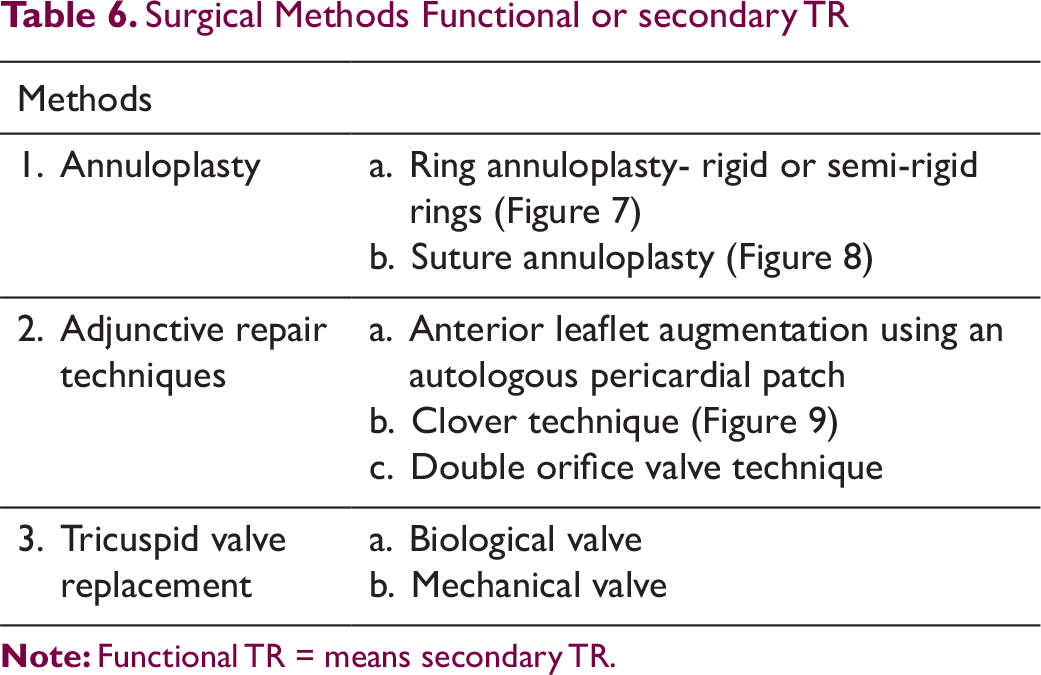
Surgical Methods Functional or secondary TR
Surgical Ring Annuloplasty repair of severe functional TR. [De Bonis et al. Surgical techniques for tricuspid valve disease. Front.Cardiovasc.Med., 28 Aug 2018]

A. Kay procedure [Bicuspidization]. B. De Vega procedure [Suture annuloplasty]. [De Bonis et al. Surgical techniques For tricuspid valve disease. Front.Cardiovasc.Med., 28 Aug 2018]

Clover technique. [De Bonis et al. Surgical techniques for tricuspid valve disease. Front.Cardiovasc.Med., 28 Aug 2018]

Tricuspid annuloplasty improves leaflet coaptation by reducing the diameter of annulus. It is accomplished by using a ring or suture. Ring annuloplasty, using flexible or rigid, is more popular because of better results and ease of the procedure. In suture annuloplasty, partial purse-string sutures (De Vega technique) are applied to the annulus to plicate the annulus to reduce the diameter of annulus. Postoperative conduction disturbances are less common. Rigid annuloplasty rings have a lower incidence of recurrent TR than flexible rings or the De Vega technique.
Adjunctive repair techniques may be needed for enhancing the effect of the ring annuloplasty in patients with marked leaflet tethering and RV remodeling and significant residual TR in spite of annuloplasty. The durability and outcome of these adjunctive repair techniques are not well established. Adjunctive procedures include (a) anterior leaflet augmentation using autologous pericardial patch, (b) clover technique, and (c) double orifice valve technique. 9 Surgical edge-to-edge TV repair was reported early by Maisano et al to treat traumatic TR. 10 The Clover technique involves suturing of the three leaflets edge-to-edge thus creating triple orifice and has been used to treat severe TR due to severe prolapse or tethering. 11
Primary TR
Surgical Methods
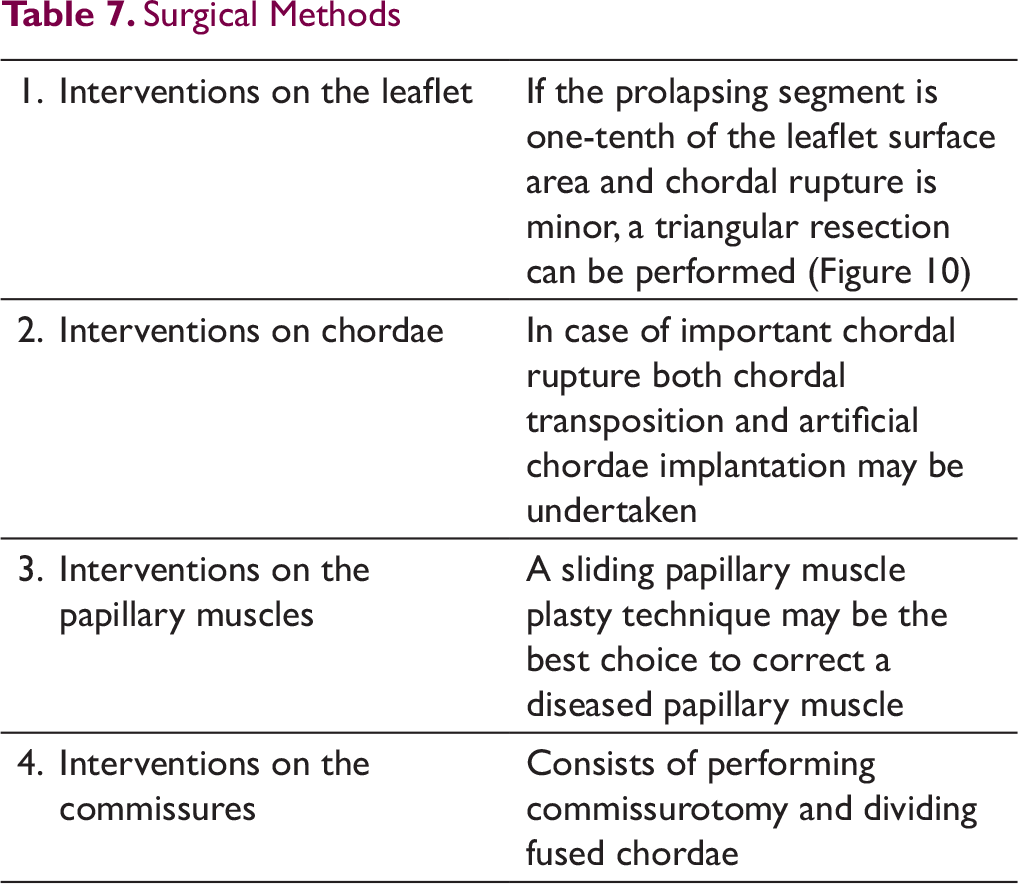
Triangular resection and pericardial patch repair. [De Bonis et al. Surgical techniques for tricuspid valve disease. Front.Cardiovasc.Med., 28 Aug 2018]

Surgical TV Replacement
Should be undertaken whenever valve repair is not feasible or durable as in rheumatic and carcinoid heart disease though it carries a higher risk compared to valve repair. Ten-year actuarial survival after TV repair and replacement was 47.5 % ± 3.5% vs 37% ± 4.8%. 12 Overall, the benefits of repair vs replacement in primary TR are ambiguous. Peri-operative mortality is fairly high, especially in older and severely symptomatic patients and in the presence of RV dysfunction, ranging between 4% and 17%. Although mechanical valves still account for nearly 40% of all TV replacements, however, bioprosthetic valve is the first choice in the tricuspid position. But no difference in survival or occurrence of adverse events at long term follow-up has been reported in patients receiving mechanical or biological valve. In a large US national registry, a total of 5005 isolated TV operations were performed over 10 years with an in-hospital mortality rate of 8.8%. 13 The incidence of re-operation is low with no significant difference when the TV has been repaired or replaced. Little is known about long term durability of TV repair for primary TR, and TV replacement is generally performed in most cases of complex, primary TR including Ebstein’s anomaly, rheumatic heart disease, infective endocarditis and carcinoid heart disease. Singh et al have shown in their seminal report that the TV repair is correlated with better outcomes than TV replacement, at least in patients with organic TV disease. 14 Most surgeons prefer placement of annuloplasty ring because it is associated with improved survival.
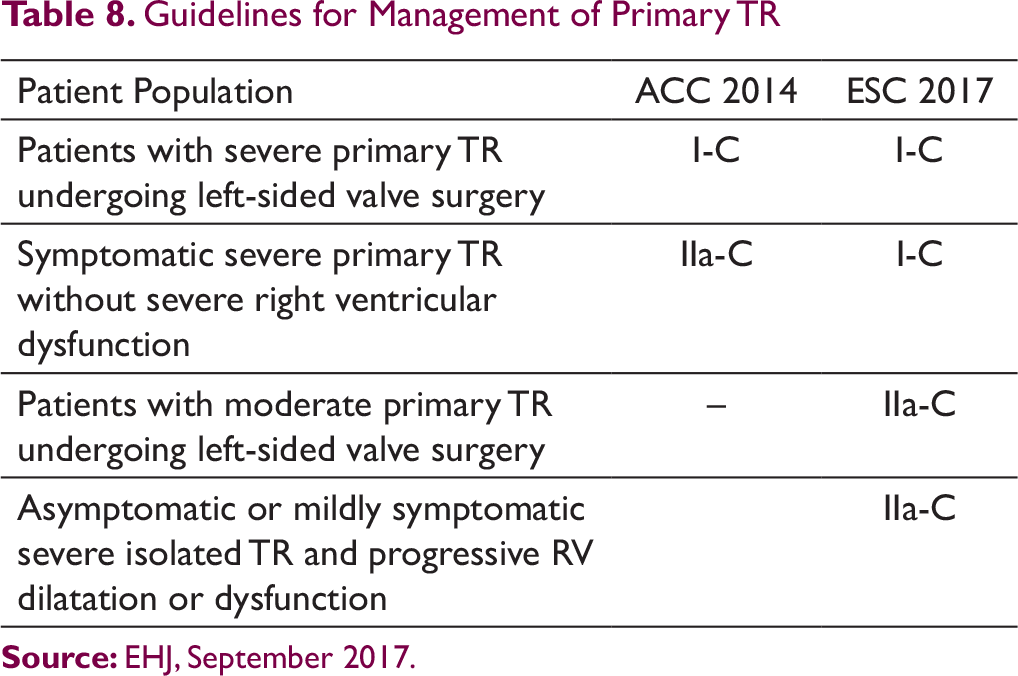
Current North American and European guidelines for the surgical treatment of primary tricuspid regurgitation with the respective levels of evidence 15 are summarized in Table 8.
Transcatheter TV Interventions
Guidelines for Management of Primary TR
Transcatheter tricuspid valve repair techniques for repair of severe TR. [Asmarats, L et al. J Am Coll Cardiol-2018:71[25]:2935–56]
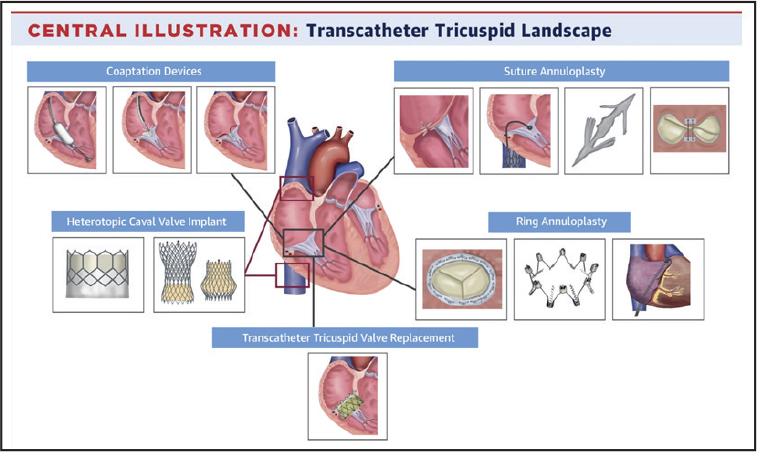
Indications of TTVIs are predominantly limited to severe functional TR at increased surgical risk due to previous cardiac surgery or co-morbidities and in the absence of severe RV dysfunction and/or severe pulmonary hypertension. TTVIs have restricted role in patients having native valve disease. TTVI may be useful in some cases of primary TR due to TV prolapse with symptomatic severe TR. If the valve anatomy is suitable, Mitra clip, the FORMA repair system and the PASCAL system can be tried in patients with primary TR with considerable surgical risk. Percutaneous TV replacement may be an option in some cases where surgical risk is prohibitively high. 28 Heterotopic CAVI aims to mitigate systemic congestion by implanting balloon-expandable or self-expandable valves in the vena cavae (inferior or in combination with the SVC) with the main purpose of abolishing systolic caval backflow. In majority of cases of primary TR, surgery is the initial choice.
The TriValve Registry is the first large scale international database collecting data on transcatheter tricuspid valve interventions. The mid-term results reported a procedural success rate of 72.8% with no difference among the different devices (66% MitraClip, 9% CAVI, 8% FORMA, 6% Trialign, 4% Cardioband, 4% Tricinch, 3% others). Procedural failure with residual TR ≥ grade 2+ was identified as a predictor of adverse outcomes. Periprocedural mortality was 0% and MACCE occurred in 10.3% at 30-day follow up. 29 According to most of the preliminary experience with different TTVI devices, procedural success was high (75%), with fairly low 30-day mortality (3.6%) and substantial functional improvement despite modest alleviation of TR. Mid-term survival at 1.5 years was high (. 30 A recently published propensity-matched case-control study comparing transcatheter valve therapy to medical treatment alone endorses the current strategy. In the 268 patients from the Trivalve registry that were matched to medically managed patients, TTVI was associated with a survival benefit (mortality 23 ± 3% vs 56 ± 3%, P = .001) as well as reduction of rehospitalization for heart failure (26 ± 3% vs 47 ± 3%, P < 0.0001) at 1-year follow-up. 31
Management According to Etiology
Rheumatic TV Disease
Isolated involvement of TV is rare in comparison to mitral valve and aortic valve involvement in rheumatic fever. However, clinically significant TV disease, in association with mitral and/or aortic valve disease, is reported in 10% to 20% of patients. Treatment of rheumatic valve disease consists of valve repair with annuloplasty along with surgery for left-sided valve disease. However, in the presence of severe disease valve replacement with a bioprosthesis are preferred despite a risk of early degeneration in younger subjects.
TR due to Pacing Leads
Severe TR due to pacing and ICD leads is less prevalent. 32 Mechanism of TR after PM implantation was found to be due to lead impingement on the leaflet in 39% , lead adherence in 34%, lead perforation in 17%, and lead entanglement in 39% in a study 0f 41 patients. Management of TR in this situation has not been well established. The strongest evidence for surgical management for lead induced TR is from a case series by Lin et al of 41 pts. Surgical repair, replacement or transcatheter TV implantation may be the solution.
Flail Septal Leaflet due to Chordal Rupture
Transcatheter repair of primary TR using the mitra-clip system favored in high-risk patient.
Drug-induced VHD
The severity of regurgitation will determine the treatment, but in general, most patients experience improvement in the grade of valve regurgitation after cessation of culprit medication. However, in some patients, TR progresses incessantly even after cessation of culprit drug warranting surgical valve replacement.
Traumatic TR
Traumatic TR is a rare complication of blunt chest trauma. Traumatic TR is mostly due to rupture of chordae of the anterior leaflet or rupture of anterior papillary muscles, causing anterior leaflet prolapse. Surgical repair is required in majority.
Endo Myocardial Fibrosis (EMF)
The most frequently used approach is endocardiectomy, combined with mitral and/or tricuspid valve repair or replacement. Because a well-defined plane of cleavage usually exists between the endocardium and the myocardium, endocardiectomy is most often feasible.
Carcinoid Syndrome
Carcinoid heart disease, also known as Hedinger syndrome, is common among 60% of patients with carcinoid syndrome. It is considered to be the result of high circulating levels of serotonin. 33 Carcinoid tumors are rare, slow-growing neuroendocrine malignancies most commonly originate from enterochromaffin cells located in the gastrointestinal tract. Cardiac carcinoid lesions are caused by deposition of pearly fibrotic plaques, notable for the absence of elastic tissue. Symptoms are caused by endogenous secretion of mainly serotonin and kallikrein. A common test measures the level of 5-hydroxy indole acetic acid (5-HIAA) in the urine sample collected over 24 hours. The development of left sided lesions implies a persistent cardiac shunt (PFO, ASD) or a very severe or poorly controlled tumor activity that may overcome the pulmonary potential to inactivate serotonin. In patients with advanced metastatic carcinoid disease, the prognosis is poor, with a median survival of only 2.6 years after diagnosis of cardiac involvement. Analysis of 17 series with carcinoid heart disease patients who had undergone surgical biological tricuspid valve replacement reveals a 30-day mortality of 20%. Typically carcinoid heart disease involves the right-sided endocardium, valves, and subvalvular apparatus (Figure 12). TR was almost universal at 92% to 100%, followed by TS (38-44%), PR (31-38%), and PS (25-38%). The prevalence of left-sided disease was 0 to 39%. 34 Three-year mortality data showed only 31% survival rate after cardiac involvement, whereas carcinoid patients without cardiac involvement have close to double the survival rate.
Indications for valve intervention include symptomatic valve dysfunction or progressive decline in RV function with valve dysfunction. Valve surgery should be considered only for patients whose metastatic carcinoid disease and symptoms of carcinoid syndrome are well controlled. For patients with symptomatic TR or pulmonary valve disease, valve replacement is the procedure of choice. The risk of valve degeneration of tissue valve may be mitigated by aggressive carcinoid tumor intervention and somatostatin therapy. Carcinoid heart disease with advanced symptoms foretell a particularly poor outcome and median survival is only 11 months.
Carcinoid heart disease with involvement of TV. [SaamirHassan et al. BMJ journals, open Heart 2019]
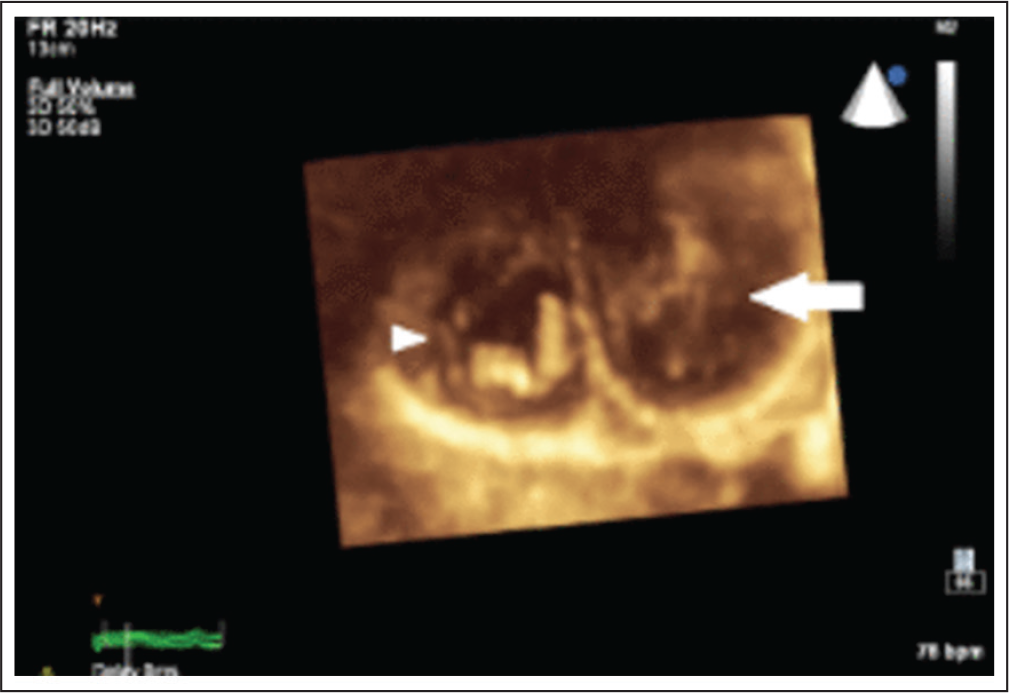
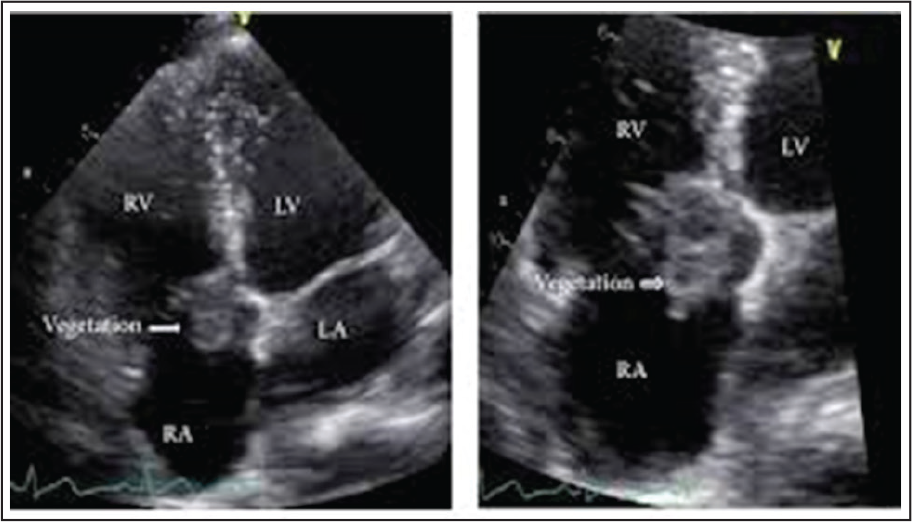
TV Infective Endocarditis (IE) (Figure 13)
Intravenous drug abusers and patients with central venous lines are prone to infective endocarditis. Suspicion is raised by the identification of echocardiographic lesions suggestive of vegetations and confirmed by positive blood cultures. Treatment of drug addicts with IE is especially demanding. Total excision of the TV without immediate replacement while continuing IV antibiotics is recommended. The prosthetic valve is implanted after ensuring complete eradication of infection. 35
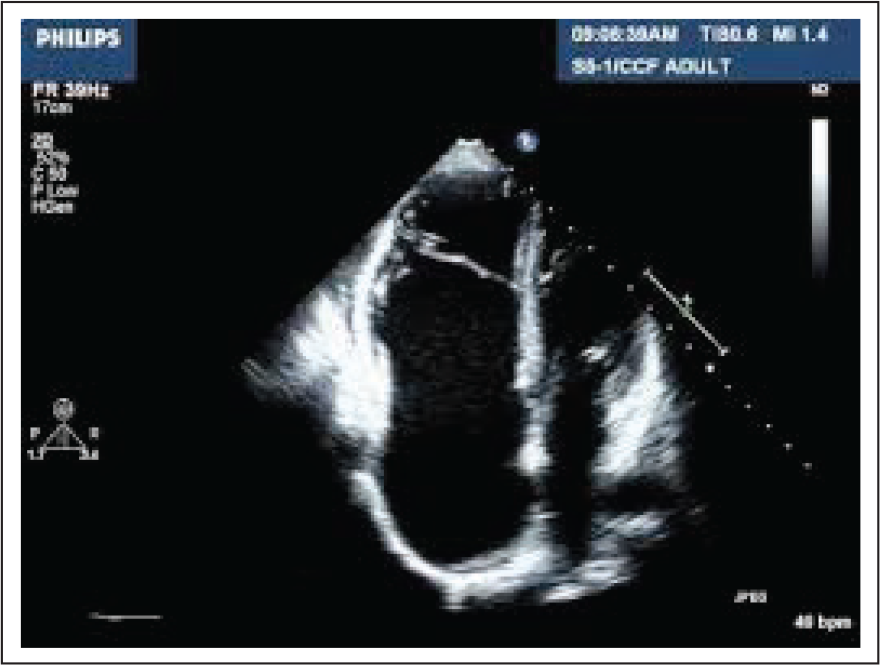
Ebstein’s Anomaly (Figure 14)
Asymptomatic TR does not require surgery. If this anomaly produces symptomatic TR, then TV repair or replacement is indicated. Ibrahim et al found evidence that Cone reconstruction of the TV for severe TR associated with low morbidity and mortality and low incidence of reoperation. In selected cases, especially patients who have been subjected to previous TV surgery, may be candidates for percutaneous TV replacement. 36
Infective endocarditis with vegetation over Tricuspid valve. [Orathai Pachirat et al. Case reports in Medicine. Aug 2015[5]:704785]
Ebstein’s anomaly of right sided tricuspid valve
Corrected Transposition of Great Arteries (C-TGA)
The morphologic TV in C-TGA exhibits some abnormality in 90% of cases. Clinically significant TR has been reported to occur in 20% to 50% of patients with C-TGA and is associated with worst outlook. The most common underlying pathology is dysplasia of the valve with or without displacement of the septal or posterior leaflet of the TV. Ebstein’s anomaly of the systemic atrioventricular valve also occurs but is different from the typical right-sided Ebstein’s anomaly. No large sail-like leaflet exists, adherence of the septal and posterior leaflet is limited, and the atrialized portion of the RV inflow is also relatively small. In addition, the systemic valve can rarely be surgically repaired with success. Sometimes valve may straddle IVS in VSD making a biventricular repair much more challenging. 37
Conclusions
Tricuspid valve regurgitation is a highly prevalent echocardiographic finding. Fortunately, in majority of people TR is mild with a benign course. Functional (secondary) TR is much more common than primary TR. Patients with TR represent a complex and heterogeneous population, and identifying the optimal method and timing of treatment are crucial. Moderate to severe TR is notorious for progression and long-term adverse consequences. Till a decade ago TR was ignored and “forgotten” because it was considered to be a benign echocardiographic finding. With evidence contrary to this myth, tricuspid valve disease has gained increasing recognition ushering paradigm shift in the thinking. Surgical treatment remains the established practice for severely damaged TV but it continues to suffer from one of the highest death rates among all cardiac valve-related surgeries. However, high morbidity and mortality was attributed to late referral for surgery. For the same reason a broad range of patients still do not receive effective therapy. Therefore, several less-invasive innovative technologies have been developed in the past decade, with promising early results for treating patients with severe, native tricuspid valve disease at high surgical risk. Some of the techniques are direct adaptation of methods used for the correction of mitral valve disease. Need for a paradigm shift towards more aggressive treatment strategies, either surgical or transcatheter, targeting less symptomatic patients is the need of the hour. The short and mid-term data on the safety and efficacy of various transcatheter TV therapies are encouraging. Appropriate patient selection, proper evaluation of anatomy, device durability, safety of the procedure and optimal timing of intervention are mandatory for the success and acceptability of the procedure.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.