
Abstract

A 56-year-old man presented with symptoms of exertional breathlessness and presyncope since last 6 years. In addition, there was history of palpitations since last 1 year and the last 3 episodes of non-exertional syncope were preceded by palpitations. The patient was diagnosed to have hypertrophic cardiomyopathy with interventricular septal thickness of 21 mm, moderate mitral regurgitation and dynamic left ventricular outflow tract gradient of 100 Hg at rest.
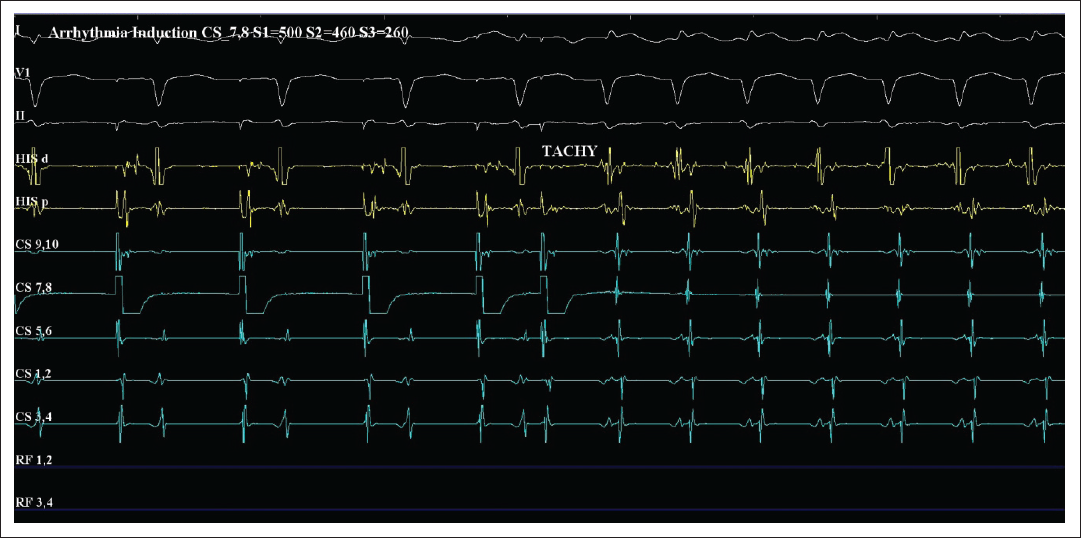
The Holter test did not reveal any significant arrhythmia. Hence, an electrophysiology study was done to evaluate for any arrhythmias. Surprisingly, an atrioventricular nodal reentrant tachycardia (AVNRT) with cycle length 240bpm (Figure) was easily and repeatedly inducible that showed significant hypotension at onset with fall in systolic blood pressure from 140 to 40 mm Hg. No ventricular tachycardia could be induced during the study.
Radiofrequency ablation of the slow pathway was performed successfully, and no tachycardia was inducible post ablation. The patient didn’t have any episode of syncope at 3-months follow-up. He was referred to an interventional cardiologist for consideration of alcohol septal ablation for persisting LVOT gradient despite being on 100 mg of extended release Metoprolol per day. In view of absence of any major risk factors for sudden death, implantable cardioverterdefibrillator (ICD) implantation was not considered.
Atrial activation that is simultaneous in all coronary sinus channels and is also simultaneous with QRS complexes with a diagnosis of typical AVNRT is seen (Figure 1).
Induction of AVNRT
Take home message: Not all syncopal episodes in patients with HCM need ICD for management. Careful history and knowledge that other arrhythmias like atrial fibrillation, atrial flutter and supraventricular tachycardia can also result in syncope in patients with HCM are important for appropriate management of such patients.
Editor’s Commentary
Kartikeya Bhargava
Keerthika et al report a case wherein the cause of syncope in a patient with hypertrophic cardiomyopathy (HCM) was found to be easily treatable supraventricular tachycardia (SVT) that shows the undoubted importance of clinical history and appropriate evaluation in all patients, especially those with syncope. 1
I wonder if the patient had received a defibrillator considering just syncope and proven HCM, he would have certainly presented shortly in future for shocks due to SVT!
Although ventricular arrhythmias are the most dreaded cause of syncope in patients with HCM since they can lead to sudden cardiac death, syncope in HCM can result due to many other reasons.
The identification of the cause of syncope in these patients can be quite challenging considering that the structural abnormality in the form of obstruction in left ventricular outflow itself can result in reduced cardiac output and syncope. Moreover, these patients have predisposition for the occurrence of both atrial and ventricular arrhythmias, both of which can lead to the worsening of symptoms and result in syncope. Lastly, the most common cause of syncope overall, namely, vasovagal or neurocardiogenic syncope, that can be diagnosed primarily from the history, accounts for one-third of the causes of syncope in patients with HCM and indicates a benign outcome in itself. 2
Also, as with vasovagal causes, patients with HCM are not immune to the development of SVTs. SVTs especially atrioventricular nodal reentrant tachycardia (AVNRT) are a rare cause of syncope, 3 but elderly and patients with structural heart disease like HCM may have a higher risk of hypotension because tachycardia can reduce diastolic filling time, worsen the outflow tract obstruction, and reduce the cardiac output further. Similar circumstances may occur with other atrial arrhythmias like atrial fibrillation and flutter as well.
The occurrence of unexplained syncope is a risk factor for sudden death in patients with HCM, especially if it occurs in close temporal proximity to the initial evaluation and diagnosis of this disease.
The risk of sudden death in HCM due to ventricular tachycardia is also more likely in younger patients. Various risk prediction models exist that estimate the risk of sudden death and need for primary prophylaxis implantable cardioverter-defibrillator implantation with great sensitivity in patients with HCM. 4, 5
Recent studies on magnetic resonance imaging also indicate that the amount of late gadolinium enhancement may also predict the risk of future arrhythmias and sudden death in patients in HCM, although they are yet to be incorporated in most guidelines. 6
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.