
Abstract
Myocardial viability is an important concept that though conceptualy inituitive however has eluded any positive benefit in a randomised trial situation . The two techniques that are cutting edge and also the most accurate are the PET and CMR . In this review we will try to address the fundamentals and the pros and cons of each technique to enable clinical cardiologists to have an understanding on which technique will be the most optimum in a given clinical situation.
Viability “a state of myocardial hypocontractility during chronic hypoperfusion, in the presence of completely viable myocardium which recovers functionally upon revascularization.”
Perspective on Viability
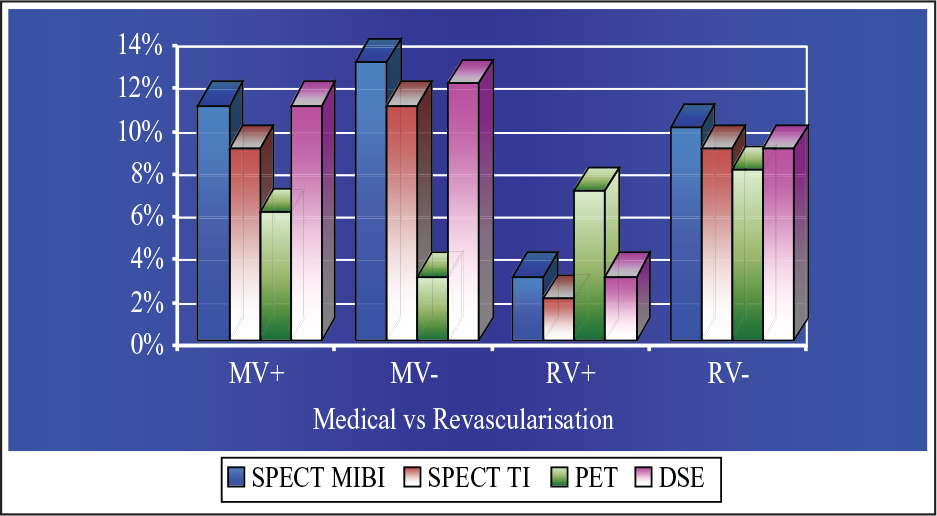
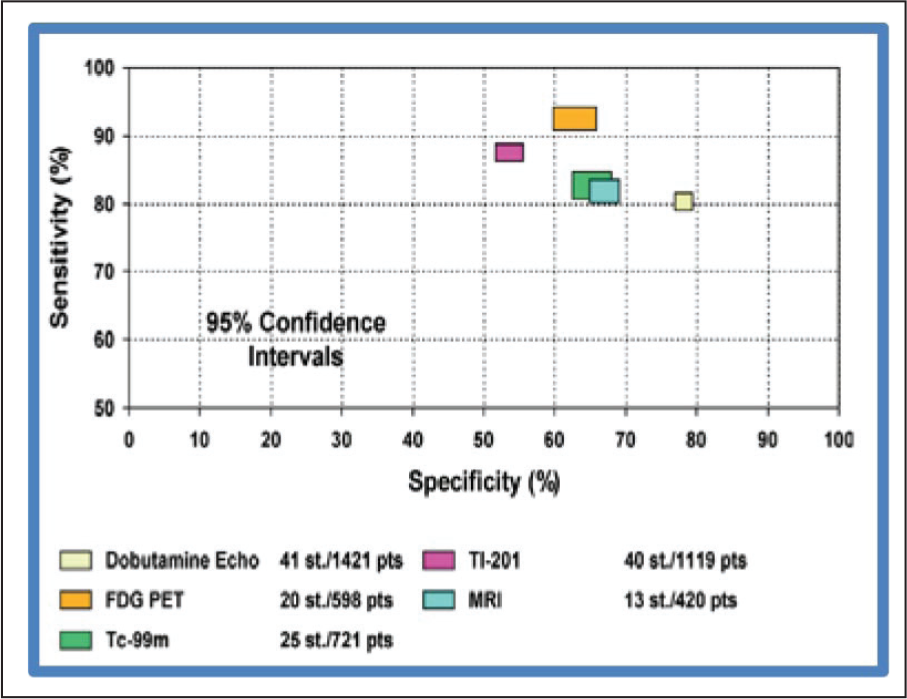
There were 3088 patients with ejection fraction of 32% ± 8%, followed for 25 ± 10 months. In patients with viability, revascularization was associated with 79.6% reduction in annual mortality (16% vs 3.2%) compared with medical treatment. Patients without viability had intermediate mortality, trending to higher rates with revascularization versus medical therapy (7.7% vs 6.2%) (Figure 1). Patients with viability showed a direct relationship between severity of left ventricular (LV) dysfunction and magnitude of benefit with revascularization (P < .001). There was no measurable performance difference for predicting revascularization benefit between the 3 testing techniques. This meta-analysis demonstrates a strong association between myocardial viability on noninvasive testing and improved survival after revascularization in patients with chronic coronary artery disease (CAD) and LV dysfunction. The absence of viability was associated with no significant difference in outcomes, irrespective of treatment strategy.
Positron Emission Tomography
Fundamentals
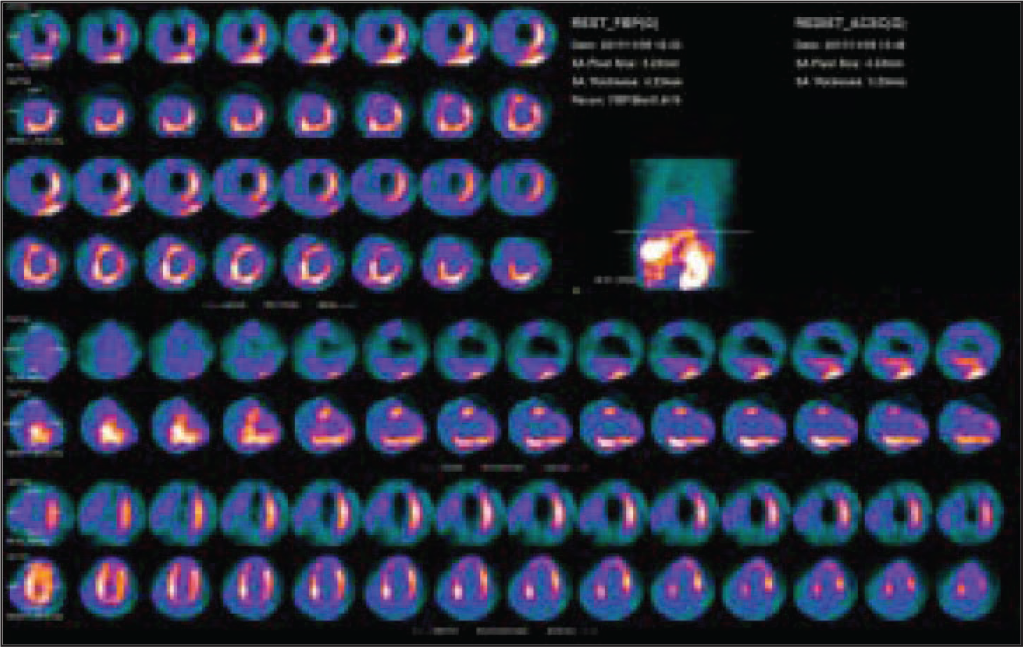
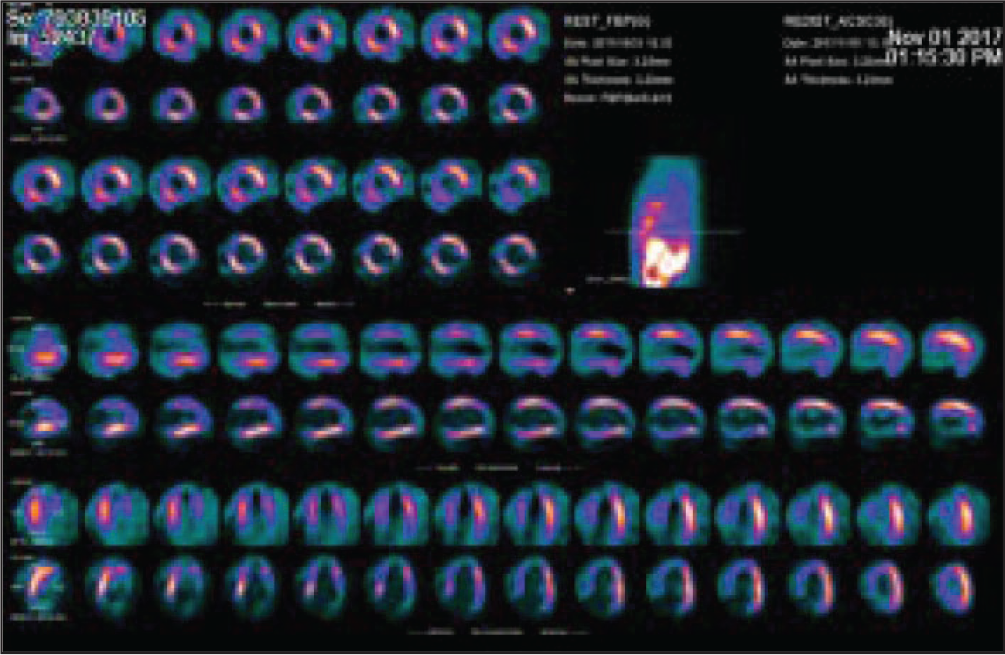
This technique has the ability to assess perfusion (via N-13 Ammonia) and metabolism (via FDG fluorine-18 labeled deoxyglucose). During ischemia myocyte metabolism shifts to glucose from fatty acids. Hence, uptake of FDG by myocytes in an area of dysfunctional myocardium indicates metabolic activity and thereby viability. The presence of enhanced FDG uptake in regions of decreased blood flow defines “hibernating myocardium” by positron-emission tomography (PET) imaging, while a concordant reduction in both metabolism and flow is indicative of “scarred myocardium.” Regional dysfunction with regional wall motion abnormality with underlying normal perfusion is indicative of “stunned myocardium.”
Technique
The PET study is performed under fasting conditions (at least 4 h) and after oral administration of 75 g of glucose. Imaging is performed using a high-resolution PET camera. Forty minutes after intravenous application of [18F]-FDG (370 MBq), PET data is acquired in a 2-dimensional (2D) fashion 1 : transmission scan (duration, 10 min) 60 min after injection and 2 emission scan (duration, 30 min). After attenuation and scatter correction the emission data is reconstructed in an iterative fashion. Furthermore, the 2D data stack is reformatted into a 3D volume to create 8 mm long and short axis slices. Gated acquisitions were performed using 16 frames per cardiac cycle and a heart rate acceptance window of 50 to 150/min. Data analysis is performed. Results are analyzed using a 20-segment polar map. The activity concentration (Bq/mL) is determined for each segment. Visual analysis is based on a 3-point rating scale: (a) viable, (b) nontransmural scar, and (c) transmural scar. End-systolic and end-diastolic LV volumes and LV ejection fraction (LVEF) are calculated automatically with specific validated software.
Pros and Cons
Advantages
Metabolic imaging is a relative gold standard for viability assessment.
It is highly sensitive to pick up small areas of viability.
Its negative predictive value is also good in that a matched defect will almost certainly not improve function post revascularisation.
It is a powerful tool for predicting outcomes after revascularization.
Disadvantages
Availability is restricted to a dozen centers concentrated in the metros.
Cost is prohibitive for a majority of the patients.
A total of 2 tracers are used in tandem for the diagnosis of viability, which is a logistical nightmare.
The preparation is cumbersome especially in diabetics.
The examination is long and can be claustrophobic.
Radiation is an issue and can be up to 7 to 9 mSv.
Positron Emission Tomography Data
Large multicenter studies such as the PET and recovery following revascularization PARR-2 trial 3 and the surgical treatment for ischemic heart failure STICH-trial have been performed with no clear verdict. 4 There is no general consensus as to the optimum strategy in patients with LV dysfunction in favor of OMT (Optimal medical therapy) or revascularization. A study looked at 43 patients with regional asynergy and an EF of 41% by PET. The positive and negative predictive value of PET for improvement post revascularisation was 76% and 96%, respectively. 5
Studies have clearly shown the linear correlation between FDG uptake and the magnitude of improvement in EF and symptoms after surgical revascularisation. 6
A viability study using PET showed that scar size on FDG was an independent predictor of improvement in EF after revascularization. In 70 patients with a mean EF of 26%, scars were divided into tertiles of 0% to 16%, 16% to 27.5%, and 27.5% to 47% of total myocardium. The incremental change in EF was greater in smaller scars, ie, 9%, 3.7%, and 1.3% for 0% to 16%, 16% to 27.5%, and 27.5% to 47%, respectively. 7
Magnetic Resonance Imaging (MRI)
Fundamentals
Spin echo imaging depicts the tissue structures of the heart as bright and the blood pool as dark (black blood approach). The spin echo method is predominantly used for anatomical imaging. 8 Steady-state free precession (SSFP) imaging generates images in which the blood pool appears bright and myocardium dark. This technique is used to evaluate left and right ventricular cavity sizes and function, ventricular mass, intracardiac shunts, valvular functions, and intracardiac masses. SSFP can generate high temporal (less than 30 ms) and spatial (2 mm in-plane) resolution cine images in an 8 to 10 s breath hold. Flow velocity encoding is a technique that is used to directly measure blood flow and is useful for quantifying the severity of valvular regurgitation and stenosis, intracardiac shunt size, and the severity of arterial vascular stenosis. 9 Cardiac gating is generally used for cardiovascular magnetic resonance (CMR) since data are typically acquired during a number of cardiac cycles to optimize spatial resolution. 10 CMR imaging can be generally performed during breath holds, longer image acquisitions require respiratory gating in addition to cardiac gating. Respiratory gating can be accomplished using a navigator approach.
Technique
CMR scans are performed on a 1.5 and 3 T scanner. Patients are examined in the supine position. The array coils are combined for signal reception. The CMR protocol consists of a LV functional study by an ECG-triggered breath-hold segmented SSFP cine sequence. Slice thickness is usually 8 mm. At first, 3 standard long axis views are acquired (4-chamber view, 2-chamber view, 3-chamber view); thereafter, the entire LV is covered by contiguous short axis slices without interslice gap. LGE (late gadolinium enhancement) images are acquired after administration of 0.2 mmol/kg gadolinium-diethylenetriamine pentaacetic acid at a flow rate of 2 mL/s. The 3 long and all short axis slices are scanned utilizing an established ECG triggered, segmented 2D inversion-recovery gradient recalled echo sequence (TR/TE, 8/4 ms; flip angle 25°) during breath-hold. LGE images are acquired 8 to 10 min after contrast media injection. To null the signal of normal myocardium the inversion time (TI, nonselective inversion pulse) is manually adjusted between 200 and 280 ms. The rectangular field-of-view (FOV) provides an in-plane resolution of 1.6 × 1.3 mm2 for all sequences.
Magnetic Resonance Imaging
Advantages
CMR has no ionizing radiation
High spatial and temporal resolution
Excellent signal to noise ratio
Free choice of imaging planes
No geometric assumptions required
Interobserver variability is low
Technique is relatively simple
Gadolinium is freely available
Assessment of post-MI complications is possible
Disadvantages
CMR is potentially problematic in patients with ferromagnetic metallic implants.
Devices such as prosthetic heart valves, intracardiac devices, sternal wires, and intravascular stents cause artifacts in imaging with CMRI at field strengths of 1.5 T.
Gadolinium contrast agents administered to patients with moderate to severe kidney disease has been associated with the syndrome of nephrogenic systemic fibrosis.
Magnetic Resonance Imaging Data
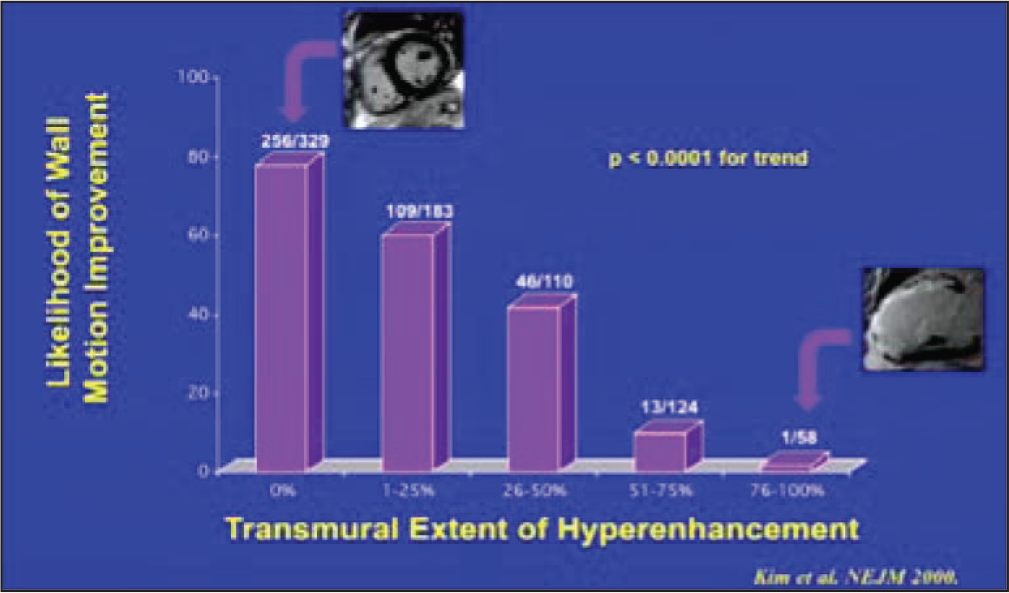
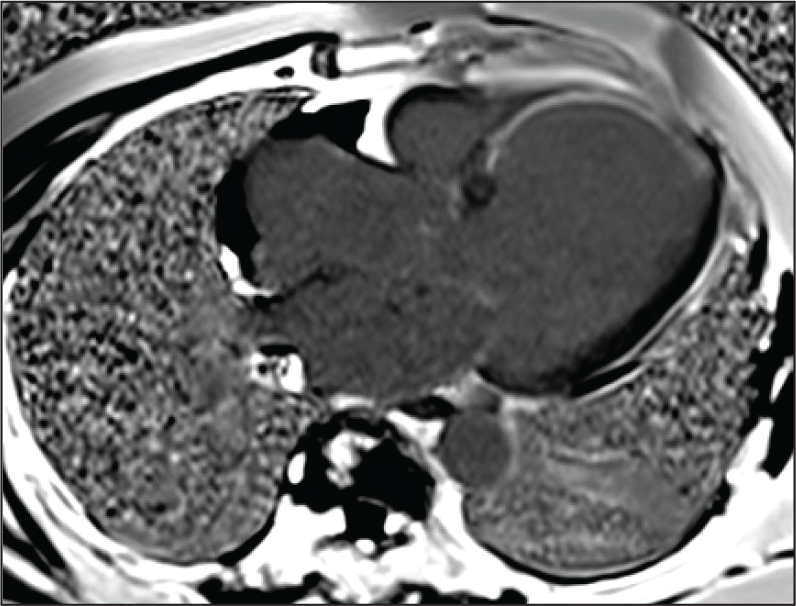
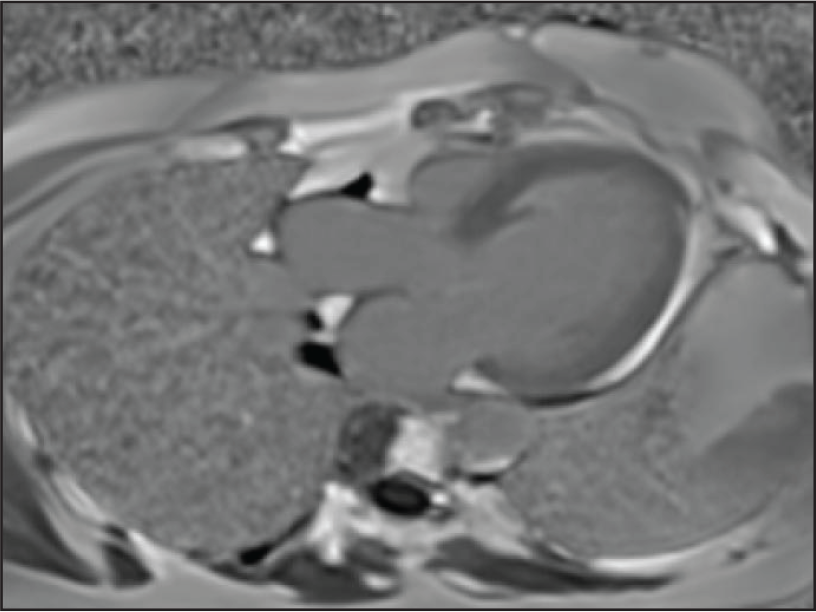
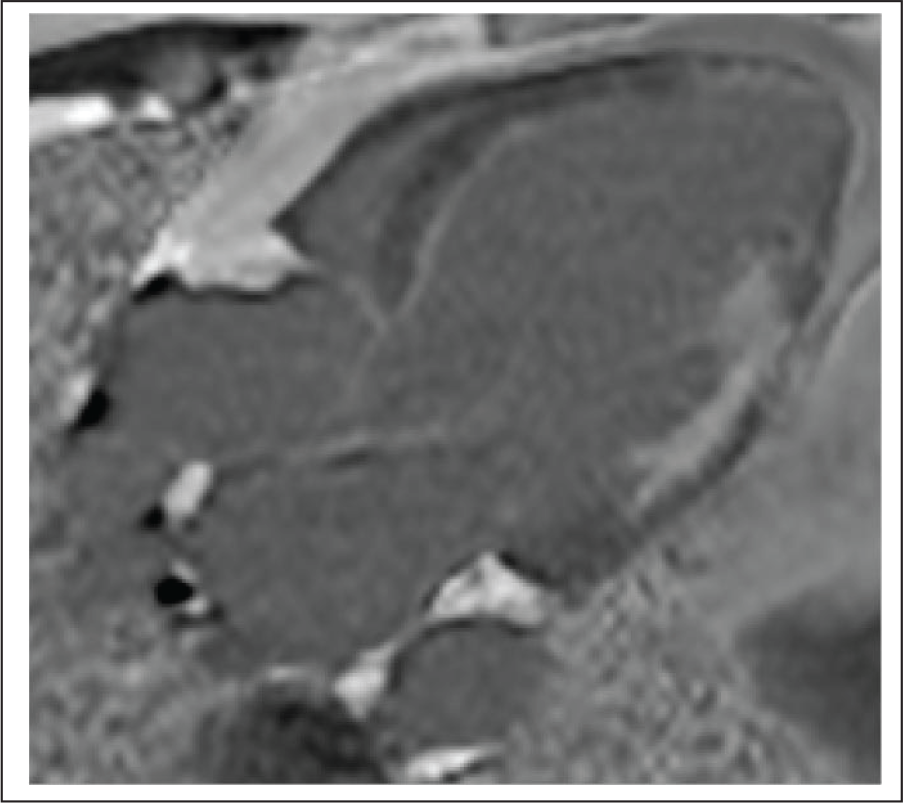
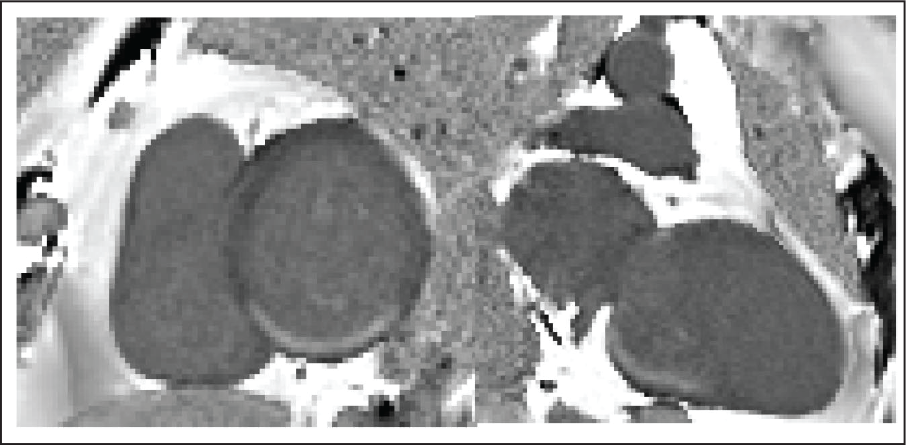
Clinical studies have confirmed that a normal LGE pattern occurs in dysfunctional myocardium that is viable and displays improved contractile function in response to low dose (5 to 10 mcg/kg/min) dobutamine infusion, while central regions with enhancement where the infarct is transmural display (Figure 5) no contractile activity in response to the dobutamine infusion. Territories that have nontransmural necrosis display a diminished contractile response to dobutamine (Figure 4). 11 LGE as a marker of scar closely agrees with the finding of matched defects on PET viability scanning. 12 A total of 32 patients with a proven MI who underwent CAG; LGE, performed after the MI, accurately established the presence, location, and transmural extent of healed Q wave and non-Q wave MI. 13 The transmural extent of infarction predicts improvement in left ventricular function. In one study of 24 patients, the extent of dysfunctional myocardium that had necrosis comprising <25% of left ventricular wall thickness (Figure 6), as established by LGE, was the best predictor of global improvement in contractility at 3 months. 14 The extent of enhancement with LGE can predict recovery of left ventricular systolic function after revascularization. 15 A total of 50 patients with CAD who had LV dysfunction prior to surgical or percutaneous revascularization found that 33% of myocardial segments in 80% of patients had evidence of LGE (Figure 7) and 38% of segments had abnormal contractility. 16 After revascularization, more dysfunctional segments without LGE improved (78% vs 17%) with enhancement of more than 75% of the tissue (Figure 8). The likelihood of improvement in regional contractility after revascularization decreased progressively as the transmural extent of LGE increased. CMR has been used to evaluate the size of the peri-infarct border zone size in relation to the core infarct as a predictor of post-MI mortality. 17 The peri-infarct border zone may represent substrate for ventricular arrhythmias.
Role of MRI Beyond Viability
MRI has a role in myocardial wall rupture detection. 18 LGE on MRI has detected right ventricular involvement in association with inferior AMI more frequently than current standard techniques. Application of LGE sequences for LV thrombosis detection has been reported to be superior than cine MRI and echocardiography. 19 In patients undergoing surgical LV reconstruction, a complete cardiac MRI protocol has shown higher sensitivity (88%) and specificity (99%) compared with transthoracic (23%, 96%) and transoesophageal (40%, 96%) echocardiography. Long-TI imaging has been suggested to increase accuracy for thrombi detection. 20 In preliminary clinical studies with MRI, the peri-infarct zone is portrayed by the visualization of a gray border zone near the central infarcted core. This “grey zone” has been related to postinfarction mortality as well as arrhythmia inducibility during electrophysiological studies. 21
What to Choose?
As a cardiologist the decision for utilizing PET should be when a patient with a large myocardial infarction pronounced nonviable by an alternative imaging technique continues to have angina or has a significant discrete lesion where even the presence of a small island of viable myocardium will swing the decision in favor of revascularization. It will also be the preferred investigation in the presence of renal failure or an implanted cardiac device. It should be avoided in uncontrolled diabetics, severe LV dysfunction with end diastolic thickness less than 6 mm, multiple coronary territory area involvement, or a patient with a post-MI mechanical complication. MRI is a relatively easy decision and should be preferred in any situation except in patients with severe claustrophobia, renal failure, and an incompatible implanted cardiac device.
Take Home Message
Absence of delayed enhancement on MRI suggests good functional recovery post revascularization.
Delayed enhancement >50% on MRI suggests variable functional recovery. Matched defects (fixed perfusion and FDG uptake) on PET suggest poor functional recovery.
Transmural scar on MRI and a matched defect on PET scan suggest no recovery post revascularization.
Conclusion
It is a close call when 2 heavyweights like PET and MRI slug it out in a battle to the finish. However, it is my opinion that MRI is the clear winner as it is easily available, cheaper, more reproducible, involves simpler logistics with a shorter procedure, and can image “beyond viability” issues, which are dear to the cardiologist and CT surgeon.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.