
Abstract
An interesting electrocardiogram obtained during a cardiac pacing procedure is presented and discussed.
Keywords
A 60-year-old gentleman underwent a cardiac pacing procedure for symptomatic sinus node dysfunction. An electrocardiogram (ECG) obtained during the implantation of one of the leads is shown in Figure 1. The question is: What cardiac structure is being captured during pacing?
Discussion
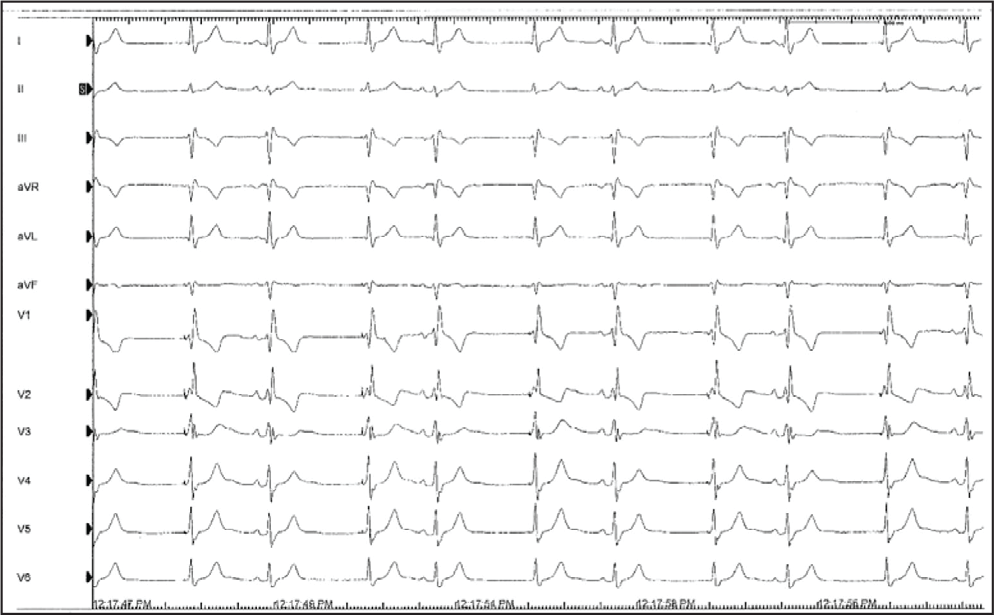
The 12-lead ECG in Figure 1 shows 2 different types of complexes. The complexes 2, 4, 6, 8, and 10 show a wide QRS complex of right bundle branch block (RBBB) morphology following a sinus P wave with a normal PR interval. These complexes are the intrinsic P-QRS complexes occurring at a slow rate. The other complexes (1, 3, 5, 7, and 9) show a pacing stimulus followed by a wide QRS complex of RBBB morphology without any preceding P waves. The question is: Where is this lead implanted and what cardiac structure is it capturing?
Since there is no P wave following the pacing stimulus, the captured chamber cannot be atrium. Interestingly, the QRS morphology following the pacing stimulus is identical to that during the intrinsic sinus rhythm. During the sinus rhythm, myocardial capture anywhere in the right or the left ventricle cannot result in a QRS that is identical to that during intrinsic QRS. Hence, the pacing stimulus is not capturing the ventricle also. The only structure that can result in the production of QRS on pacing with a QRS identical to the sinus rhythm is the atrio-ventricular (AV) junction or the His bundle. In fact, if one ignores the pacing spikes, the ECG looks like that of sinus bradycardia with RBBB and frequent junctional extrasystoles. A QRS complex follows the pacing spike after a short interval (30–40 ms) that is akin to the HV interval during the electrophysiology study.
Twelve-lead ECG during a pacemaker implantation procedure.
The same 12-lead ECG as in figure 1 showing the P waves (P), intrinsic QRS complexes (Vs) and QRS occurring as a result of pacing (Vp). The Vs to Vp interval is constant at 1000 ms or 60 bpm indicating pacing at 60 min– 1 . The arrows show the pacing stimulus.
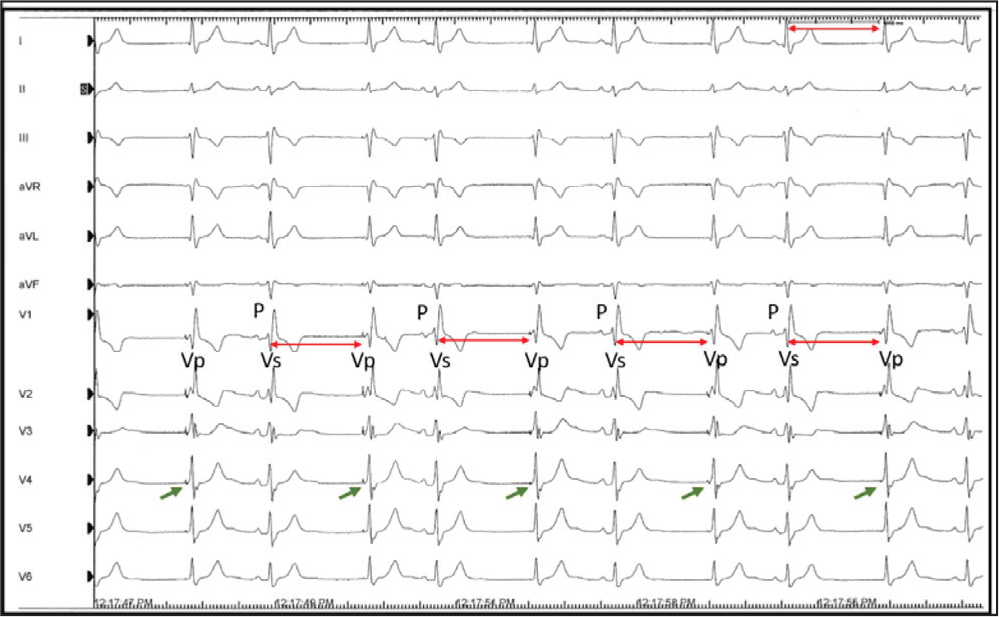
The measurement of the intervals between intrinsic (Vs) and paced (Vp) QRS complexes shows that the Vs to Vp interval is constant at 1000 ms but the Vp to Vs interval is variable (Figure 2). This finding is consistent with VVI pacing at 60 beats per minute (bpm), where V is representing the His bundle pacing (rather than ventricle).
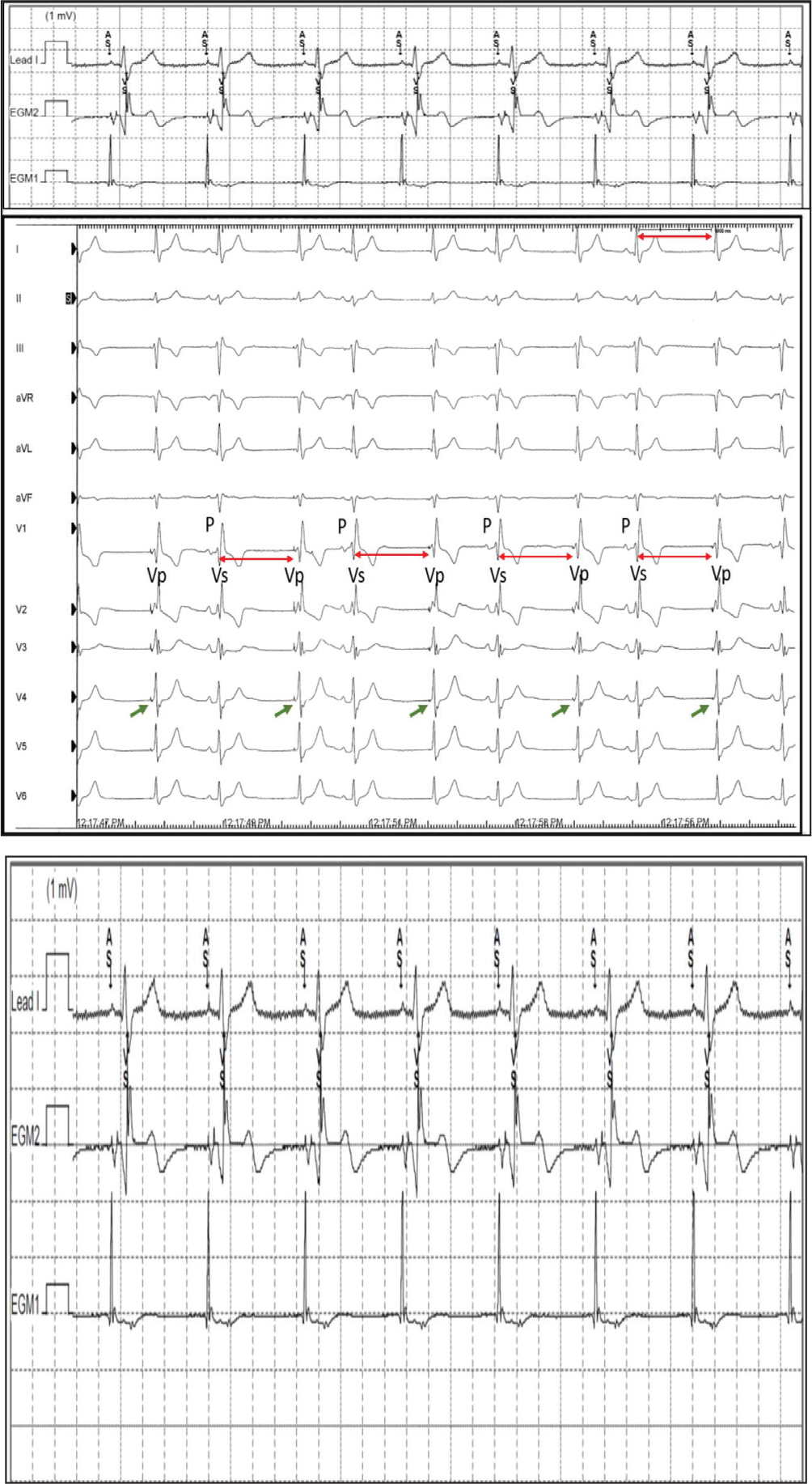
The ECG was recorded while placing the His bundle lead during the dual chamber (atrial and His bundle) pacemaker implantation. The unipolar electrogram at the site of good His bundle capture shows a His signal (Figure 3) apart from the atrial and ventricular signal like that recorded by a His bundle catheter during electrophysiology studies. His bundle pacing results in the recruitment of cardiac conduction tissue ensuing preserved normal ventricular activation sequence and the absence of any dyssynchrony. 1 Hence, there is no potential risk of pacing-induced left ventricular dysfunction during the long term. 2
It is easy to understand that His bundle capture can result in a normal appearing QRS complex in patients with preserved AV conduction3, 4 as in the present case. However, fortunately, it can also result in a narrow QRS complex in patients with deranged AV conduction including bundle branch block, and complete nodal and even infranodal AV block.5, 6 His bundle pacing has been shown to normalize the QRS complex in some patients with left bundle branch block and left ventricular dysfunction, and hence can be used as an alternative to cardiac resynchronization therapy.7-9 Various mechanisms have been described to explain the narrowing of QRS with His bundle pacing
10
and include the following:
longitudinal dissociation of the His bundle with pacing adjacent or distal to the site of block; virtual electrode polarization effect; and differential source and sink relationships during pacing versus intrinsic impulse propagation.
The current interest among the electrophysiologists as well as the industry in His bundle pacing along with future advancements in the implant technology and hardware is likely to increase its use in patients who require pacing and resynchronization therapy. Hence, it is important for clinicians and cardiologists to know the electrocardiographic basics and nuances of His bundle pacing.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.