
Abstract
Background:
Palliative care access remains limited in Lebanon, particularly outside the capital. Data on public palliative care knowledge and perceptions in general and among disadvantaged populations remain insufficient.
Objective:
This study aimed to assess palliative care awareness and knowledge among community users of a non-governmental organization serving socioeconomically disadvantaged populations in Tripoli, north of Lebanon.
Methods:
A cross-sectional study was conducted using a structured survey targeting 400 individuals using the Palliative Care Knowledge Scale (PaCKS) in the colloquial Arabic language. Data on palliative care awareness and background information were collected. Multivariable binary logistic regression using stepwise backward selection was conducted to identify predictors associated with palliative care knowledge levels and common misconceptions.
Results:
Low awareness of palliative care was observed, with 95.8% of participants reporting never having heard of it. PaCKS’s mean score was 9.24 ± 2.89; 40.8% (N = 163) had high scores (11–13), 42.8% (N = 171) had moderate scores (7–10), and 16.5% (N = 66) had low scores (0–6). Common misconceptions included perceiving palliative care to be limited to hospital care, to cancer, and to end of life. Higher educational attainment was a strong and stable predictor of palliative care knowledge and common misconceptions. Participants with middle or high school education had 1.754 higher odds (p = 0.013), and those with university education had 4.938 higher odds (p < 0.001) for higher knowledge compared to participants with no or primary education, potentially indicating a graded association. More than half of the participants expressed interest in having information about palliative care made generally available.
Conclusion:
Our results indicate low awareness and several misconceptions about palliative care along with the presence of health inequities. Low educational attainment, mainly linked to socioeconomic disadvantage, may limit health literacy, and as such, reduce access to information and the ability to understand complex concepts such as palliative care. These findings highlight the urgent need for a collaborative, multi-sectoral system-thinking, community-centered, and equity-driven approach that involves the community, researchers, healthcare providers, and policymakers.
Plain language summary
In Lebanon, people have limited access to palliative care services. There is insufficient information on the knowledge and awareness of palliative care among laypeople including disadvantaged communities. We conducted this study to understand how much people using the services of a non-governmental organization in Tripoli, north of Lebanon, know about palliative care and what common misconceptions they have.
We administered a survey in the colloquial Arabic language by trained interviewers. We looked at the knowledge scores and examined whether information such as education, age, gender, and others influence the level of knowledge of participants.
Our study found that most participants never heard of palliative care before. Although they had good palliative care knowledge, almost half of them thought that palliative care is limited to hospitals, cancer, and end of life. Participants who had no school education or completed primary education were more likely to have lower knowledge and more misconceptions about palliative care compared to those who completed high school or university education. Participants were interested in knowing about palliative care even in the absence of a serious illness.
Our findings indicate that participants have limited awareness and several misconceptions about palliative care, especially among those who have lower education, making them less likely to access correct information and palliative care services when they need it. Interventions should focus on engaging communities as equal partners to improve palliative care awareness and access, with collaboration between researchers, healthcare professionals, and policymakers.
Keywords
Introduction
Palliative care is a holistic approach that aims to reduce suffering and improve quality of life for people living with serious illnesses and their families. 1 Globally, an estimated 56.8 million people require palliative care, with 78% residing in low- and middle-income countries (LMICs). 2 Meeting the immense need for palliative care requires a public health palliative care approach known as “compassionate communities.” This social model of care aims to bring death, dying, grief, and caregiving back into social networks by empowering community members to reclaim their caregiving role, connect people to support, and raise awareness about end-of-life issues. 3 Studies demonstrate that compassionate communities can enhance understanding of palliative care 4 ; reduce utilization of hospital services 5 ; improve quality of life, decrease loneliness and stress, strengthen social support and self-confidence, 6 and improve community awareness and access to care and resources.7,8
Although awareness and knowledge of palliative care is a crucial first step to building compassionate communities and increasing access to palliative care, studies worldwide including Arabic-speaking countries have consistently shown low public awareness and knowledge of palliative care.9–12 Addressing this gap through traditional top-down health campaigns has widened disparities by benefiting more advantaged groups. 13 As such newer interventions focus on equity through community-based participatory approaches14–18 while addressing structural determinants 19 and barriers to sustainability. 20
Lebanon is an LMIC in the Eastern Mediterranean region that has been grappling with economic, financial, and security crises since 2019. 21 The overlapping crises impacted the Lebanese healthcare system, through the migration of healthcare workers, reduction in financing, and shortages of medicines and supplies, thus reducing the availability and affordability of quality healthcare and delaying treatment. 22 In Lebanon, it is estimated that 31,000 people need palliative care annually 23 mainly attributed to an aging population 24 and a high non-communicable disease burden (48% of all mortalities), 25 especially cancer where 13,000 people were newly diagnosed and 7,307 died from cancer in 2022. 26 A study showed that certain remote areas in Lebanon had a higher percentage of advanced-stage breast cancer diagnosis compared to central areas. 27
Palliative care provision in Lebanon is described as “progressing” with uneven development, isolated services, and lack of system-wide integration 28 with most services concentrating in the capital. Barriers include inadequate specialist training, lack of financial reimbursement, physician reluctance, and limited public awareness. 29 The 2023 5-year National Cancer Control Plan includes a chapter with actionable recommendations on supportive and palliative care that aim to strengthen health system integration, including addressing public awareness and involvement. 30
Even though Lebanon is known for its collectivist culture and the important role families play in caregiving, death, and loss, community involvement in shaping this scene has been very passive. Awareness among the public is generally limited. According to a survey conducted in the capital and its suburbs, 65.5% were totally unaware of palliative care and almost 37% of those aware of palliative care had low knowledge levels. 31 Data on palliative care awareness and knowledge outside the capital and among disadvantaged populations are particularly unavailable. The rationale of this study is rooted in the limited research on palliative care awareness and knowledge, particularly amid increasing efforts to strengthen palliative care integration within the Lebanese healthcare system.
Methods
Study aim
The primary aim of this study is to assess public’s awareness and knowledge of palliative care and explore characteristics significantly associated with good knowledge among a disadvantaged community within the context of a non-governmental organization (NGO) in Tripoli, Lebanon. The study aimed to answer the following research questions among socioeconomically disadvantaged populations:
What is the level of awareness and knowledge of palliative care?
What are common misconceptions about palliative care?
What factors are significantly associated with high palliative care knowledge?
What are the community preferences toward receiving information about palliative care?
This study is part of a larger project that explored the community needs, knowledge, perceptions, and attitudes toward palliative care. Its overall goal was to provide baseline information to support the development of a culturally tailored home-based palliative care service and awareness activities in Tripoli where no palliative care services were available at the time, and with the technical support of a leading home hospice care organization in Lebanon.
Study design
A cross-sectional study was conducted using a structured survey administered by trained interviewers.
Study setting and participants
The study took place at a local NGO located in Tripoli, north of Lebanon. Tripoli is the country’s second largest city, one of the most deprived cities and known for its highest poverty rates. 32 In an already strained healthcare system, hospitals in Tripoli face even more challenges in providing quality care, where barriers vary from financial constraints and inadequate skilled staff to limited staff compensation and motivation, among others. 33 No palliative care services were available in the city at the time of study initiation.
The NGO supports socioeconomically disadvantaged people in the local area, serving around 18,000 residents and providing a multi-faceted approach to basic services, including food, education, and healthcare services, among others. Service users benefit from the NGO’s services based on a socioeconomic assessment to determine eligibility to support services.
The study’s target population and inclusion criteria included all cognitively competent adults aged 18 years and above, oriented to person, place, and time, residing in Tripoli and seeking healthcare services at this NGO. Anyone who didn’t meet any of the inclusion criteria was excluded.
Sampling, recruitment, and data collection
The organization’s database included 10,000 health service users. To achieve a 95% confidence level and draw a convenience sample, 370–400 completed surveys were required based on the below formula for sample size calculation 34 with N = 10,000 being the number of beneficiaries of the NGO, Z = 1.96, e = 0.05, and p = 0.5 in our case, given the unknown proportion of palliative care knowledge in our population.

Data collection took place between April 2023 and May 2023 following a non-probability convenience sampling approach. Eligible participants visiting the NGO were approached and recruited by the organization’s administrative staff who were not involved in healthcare delivery. Staff, who are trained to communicate with disadvantaged populations, were also trained by the research team on ethical conduct and survey administration aspects and informed of study’s general aim without knowledge of its hypothesis. To reduce bias, interviewers were trained to read questions as written, maintain neutral body language, and avoid influencing participants’ answers when clarifications were needed.
To ensure autonomy, all eligible participants were informed of the study aim and their right to voluntarily participate and refuse without affecting their ability to access the organization’s services. Participants who agreed to participate were required to sign a consent form or provide their fingerprint as a form of signature. If participants could not read or write, an additional research assistant was present during the consent process as a witness. To ensure privacy the survey was administered in a separate room at the center. If participants experienced emotional distress, they were referred to the on-site social worker at the NGO to receive the appropriate support.
Data collection tools
In this study, a total of 25 questions were used to assess palliative care awareness, knowledge, and background information (see Supplementary Material).
Awareness of palliative care was assessed using three questions: perceived level of awareness of palliative care (never heard of it/know it by name/have a vague idea/have a general idea/have a clear idea), source of information about palliative care, and whether they have received palliative care services before.
The level of palliative care knowledge was measured using the Palliative Care Knowledge Scale (PaCKS) tool that was developed and validated by Kozlov et al. 35 The PaCKS is a 13 True/False/Don’t Know item tool that includes statements about palliative care timing, target population, and care provision.35,36 According to Kozlov et al., 36 a score of 1 is given to correct answers and a score of 0 is given to incorrect and Don’t Know (DK) answers, with the total score ranging between 0 and 13, with higher scores indicating more knowledge. All participants were asked the PaCKS questions regardless of their awareness of palliative care, as done by Kozlov et al. 36 In our study, Cronbach’s alpha value for the PaCKS was 0.76, including the DK option.
After the PaCKS questions, participants were provided with the palliative care definition and then were asked about the best timing to receive information about palliative care (would not want information at any point/more information to be generally available/only want information to be provided if diagnosed with a life-threatening illness/only want information if a life-threatening illness becomes terminal). Background and demographic information included eight questions: age, gender, highest level of education, marital status, nationality, living condition, perceived health status, presence of illness(es), and list of illness(es).
The survey questions were translated from English to Modern Standard Arabic by the research team members whose native language is Arabic, and are fluent in English, following principles of good practice for translation and cultural adaptation. 37 Two forward translations were conducted independently and were then reconciled by a third team member and piloted by the research team to assess the understandability and smooth flow of the questions. Survey questions were piloted with 10 participants, with results revealing difficulty in understanding Modern Standard Arabic. As such, colloquial Lebanese Arabic was used to make the questions easier to comprehend and standardize the way questions were asked. This colloquial version was piloted again with another 10 participants and finalized with no additional changes.
Statistical analysis
Data obtained were exported for statistical analysis using SPSS v. 26.0. 38 The dataset didn’t have any missing data. Categorical variables were described using frequencies and percentages, while continuous variables were presented using medians, means, and standard deviations. Illnesses were summarized using the categorization of the Health Research Classification System. 39 For the PaCKS descriptive analysis, a score equal to or below 6 was considered a low level of knowledge, 7–10 a moderate level, and 11–13 a high level, guided by Atena et al. 40
To identify factors associated with palliative care knowledge, bivariate analysis was conducted to examine the unadjusted association between each independent variable and the dependent variable, followed by stepwise backward multivariable binary logistic regression. The dependent variable was palliative care knowledge scores that were computed as indicated by Kozlov et al. 36 (correct answer = 1, incorrect/DK answer = 0) and grouped into two categories for inferential statistics: high (PaCKS = 11–13) and low (PaCKS <11) guided by the Atena et al. division. 40 Independent variables included in the model were categorized as follows based on established divisions and data distribution: Gender (male [reference]/female), Age (<40 [reference]/40–60/>60), Marital status (never married [reference], married, previously married), Living condition (alone [reference]/with family or others), Education (low education—no school and elementary school [reference]/medium education—middle and high school/high education—university education or equivalent), nationality (non-Lebanese [reference]/Lebanese), palliative care awareness (never heard of palliative care [reference]/heard of palliative care), perceived health status (very ill [reference]/ill/relatively good/good), and having a chronic illness (no [reference]/yes; chronic illness coded as “yes” and acute illnesses/no illness as “no”). A stepwise backward selection logistic regression method using p values was used where all the variables are tested in a regression model and, subsequently, the least significant variables are eliminated in a stepwise approach. 41 First, a full model was conducted with all nine independent variables, which were then removed one by one based on the highest p value until all variables in the final model had a p ⩽ 0.2 as a removal threshold according to Hosmer–Lemeshow. 41 Model fit was tested using the Hosmer–Lemeshow test, and the predictive power was evaluated using Nagelkerke’s R².
To test the robustness of the regression model findings, sensitivity analysis was conducted for the outcome of palliative care knowledge levels with DK answers weighed as 0.5 (neutral) and as 1 (correct answer). Results of the final regression models were compared to the final model obtained when DK was weighed as 0. Furthermore, multivariable binary logistic regression was conducted for the three most common misconceptions as the outcome with the same nine independent variables following the same stepwise backward selection method. Prior to conducting regression, independent variables were tested for multicollinearity using VIF and Tolerance statistics. All values demonstrated the absence of multicollinearity with VIF values ranging between 1.014 and 1.365, well below the threshold of 5. Statistical analyses were conducted at a significance level of 0.05 with a 95% confidence interval.
Results
Participants’ demographics and background information
A total of 400 participants completed the survey with a response rate of 79.8%. Initially, 501 participants were eligible to participate; 101 individuals either refused (N = 95) to participate or withdrew (N = 6). The most common reason for refusal was the absence of direct benefit (Figure 1).

A flow diagram showing inclusion and exclusion process with 400 participants completing responses.
Participants’ age ranged between 19 and 82 years, with an average of 46.8 years. Most participants were females (63.5%, N = 254), Lebanese (95.5%, N = 382), married (61.5%, N = 246), and lived with family members (93.8%, N = 375). Educational levels varied, with 45.0% (N = 180) having completed elementary school, 22.0% (N = 88) middle school, 11.3% (N = 45) high school, and 9.5% (N = 38) university or equivalent technical education. Notably, 12.3% of participants (N = 49) reported they did not receive any formal education (Table 1).
Demographic and background information about participants.

HRCS: Health Research Classification System.
The majority of participants (78.3%, N = 313) reported having one or more illnesses, with the most frequent disease categories being cardiovascular (17.6%, N = 108), musculoskeletal (15.8%, N = 97), and metabolic and endocrine (12.0%, N = 74) conditions. Almost 51.3% (N = 205) of participants described their health condition as ill or very ill, and 48.8% (N = 195) as good or relatively good (Table 1).
Participants’ awareness of palliative care and PaCKS scores
A significant majority (95.7%, N = 383) of participants never heard of palliative care prior to the study. Of those who heard of it (4.2%, N = 17), only 1.2% (N = 5) reported having a clear understanding, and only one participant had previous experience with palliative care services. Participants’ PaCKS scores had a mean of 9.24 ± 2.89, a median of 10, and ranged between 0 and 13. When the PaCKS score was divided into three categories, the results showed that 40.8% (N = 163) had high scores (11–13), 42.8% (N = 171) had moderate scores (7–10), and 16.5% (N = 66) had low scores (⩽6). Nearly half of the participants had incorrectly answered that “people must be in the hospital to receive palliative care” (51%, N = 204), “palliative care is exclusively for people who are in the last six months of life” (47%, N = 188), and “palliative care is specifically for people with cancer” (41.3%, N = 165; Table 2 and Figure 2).
Participants’ awareness and knowledge of palliative care.

PaCKS: Palliative Care Knowledge Scale.

Distribution of correct and incorrect answers across PaCKS statements.
Factors associated with PaCKS scores
Bivariate analyses were conducted with education, nationality, and living conditions showing statistical significance (Table 3). The results of the full logistic regression model with the nine variables significantly predicted palliative care knowledge compared to a model without predictors with χ²(14) = 36.768, p < 0.001. The model had a Nagelkerke R² = 0.119, suggesting a modest explanatory power of variables explaining almost 12% of the variation in palliative care knowledge. The model demonstrated a good fit as indicated by the Hosmer-Lemeshow test (χ²(8) = 8.756, p = 0.363). Education and nationality were significantly associated with palliative care knowledge. The stepwise backward selection process resulted in a final model that retained three variables, almost maintained its explanatory power (Nagelkerke R² = 0.099), and enhanced its fit Hosmer–Lemeshow test (χ²(3) = 1.033, p = 0.793). Education remained strongly significant, with participants with middle or high school education having 1.754 higher odds (p = 0.013) and participants with university education having 4.938 higher odds (p < 0.001) for higher palliative care knowledge compared to participants with no or primary education, potentially indicating a graded association. Nationality also remained a significant predictor, with Lebanese participants having 3.656 higher odds (p = 0.048) for higher palliative care knowledge compared to non-Lebanese (Table 4).
Unadjusted estimates between the outcome palliative care knowledge groups and independent variables.
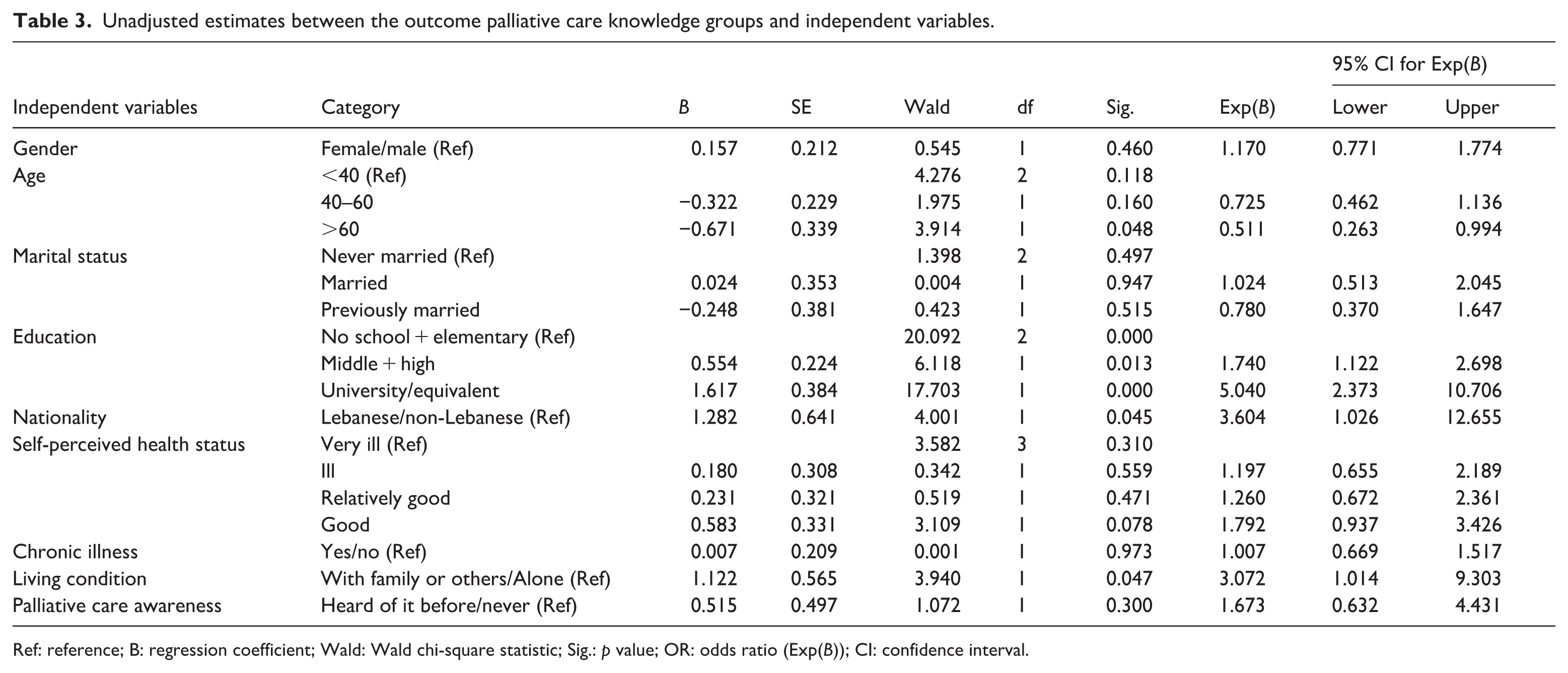
Ref: reference; B: regression coefficient; Wald: Wald chi-square statistic; Sig.: p value; OR: odds ratio (Exp(B)); CI: confidence interval.
Multivariate logistic regression for factors associated with palliative care knowledge groups (DK = 0).
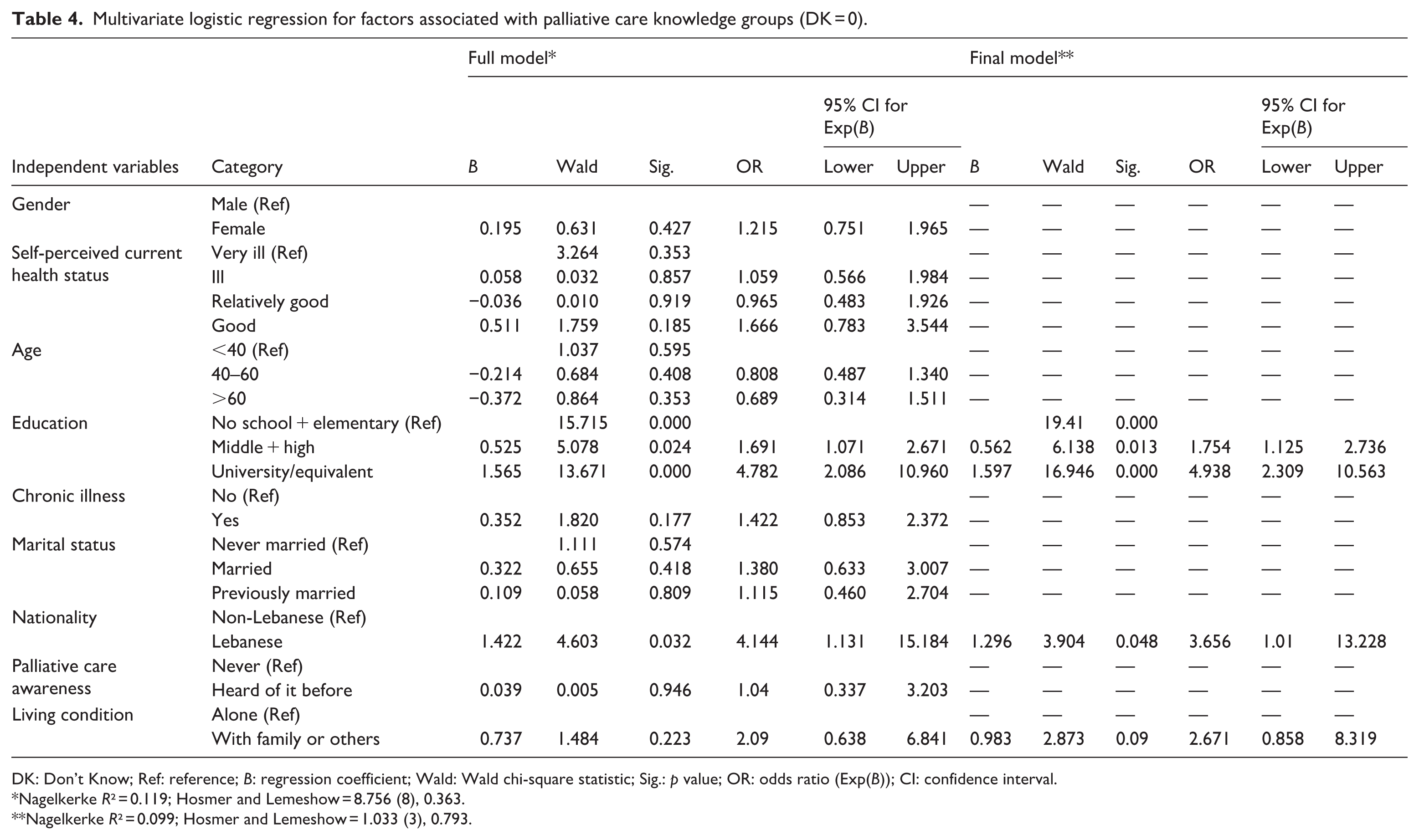
DK: Don’t Know; Ref: reference; B: regression coefficient; Wald: Wald chi-square statistic; Sig.: p value; OR: odds ratio (Exp(B)); CI: confidence interval.
Nagelkerke R² = 0.119; Hosmer and Lemeshow = 8.756 (8), 0.363.
Nagelkerke R² = 0.099; Hosmer and Lemeshow = 1.033 (3), 0.793.
In our study, on average, around 16% of respondents answered DK per PaCKS item with DK responses ranging between 8.3% and 23.8%. The total number of DK responses ranged from 0 to 13, with a mean of 2.10 (SD = 2.665) and a median of 1.00. The most frequently reported number of DK responses was 0, indicating that a substantial proportion of participants provided answers to most knowledge items. When stratified by level of palliative care knowledge, participants with high knowledge had a substantially lower mean number of DK responses (M = 0.40, SD = 0.643) compared to those with low or medium knowledge (M = 3.26, SD = 2.893). To assess the robustness of our findings, we conducted a sensitivity analysis by comparing the final logistic regression model with DK weighed as 0 to those with DK weighed as 0.5 (Table 5) and 1 (Table 6), respectively. Findings indicated a better model fit with an increasing p value for the Hosmer–Lemeshow test and increasing variance explained as the weight for DK increased. Education remained a strong and stable predictor of palliative care knowledge with a marked increase in odds ratio (OR) for the highest educational level (OR = 8.065, p < 0.001, DK = 0.5; OR = 9.016, p = 0.003, DK = 1); potentially indicating that participants with university education were more likely to provide a DK answer when uncertain rather than provide a guessed answer. On the other hand, nationality, which was significant became insignificant in both sensitivity models, indicating that potentially non-Lebanese participants were more likely to provide DK answers compared to Lebanese, and as such, the significance of this variable disappeared with DK weighted as 0.5 and 1. Noticeably, living condition (OR = 3.143, p = 0.033, DK = 0.5; OR = 4.346, p = 0.002, DK = 1) emerged as a new significant predictor in the sensitivity analysis models, indicating that people who lived with family members/others were more likely to provide DK answers compared to those who lived alone.
Multivariate logistic regression for factors associated with palliative care knowledge groups (DK = 0.5).
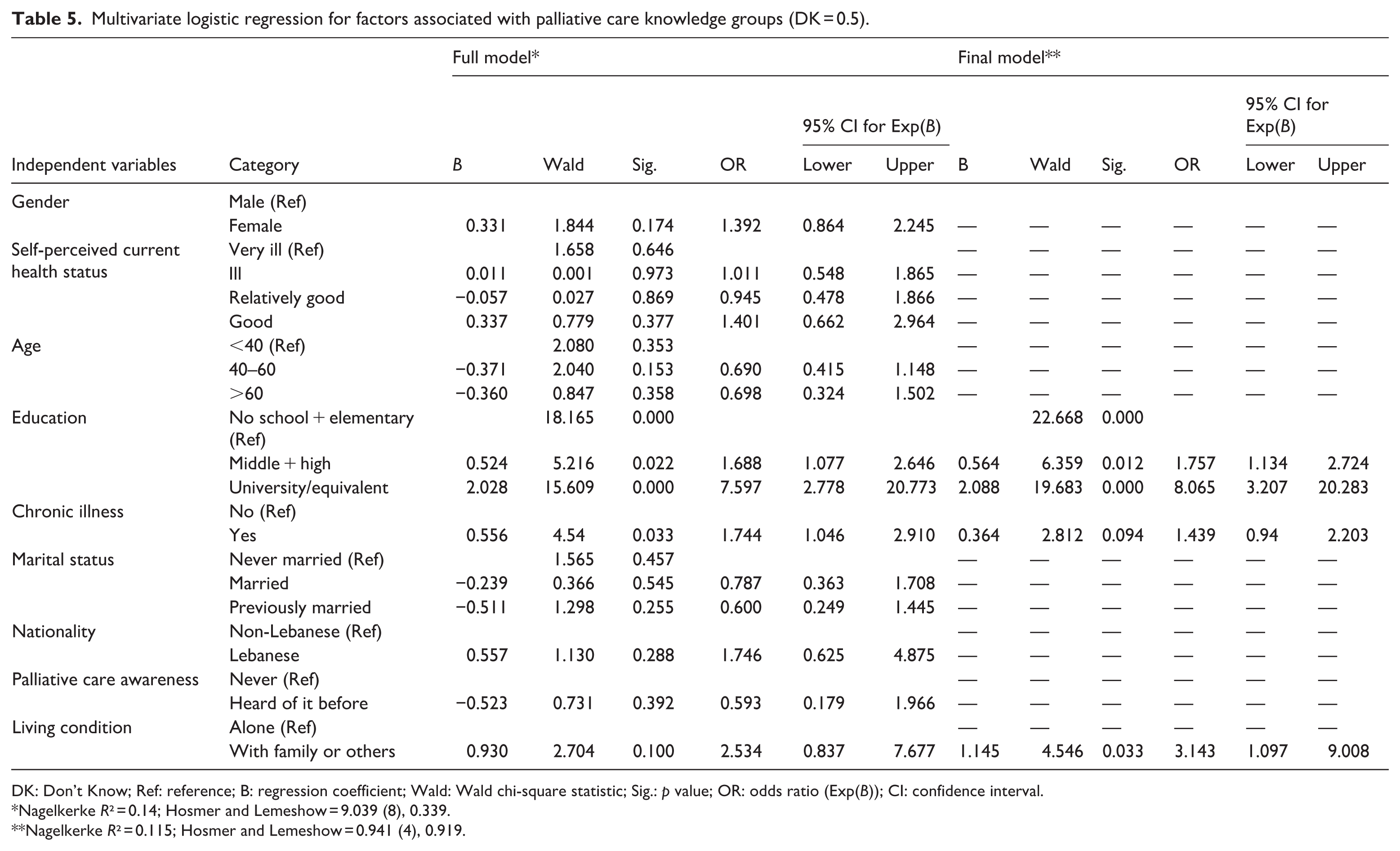
DK: Don’t Know; Ref: reference; B: regression coefficient; Wald: Wald chi-square statistic; Sig.: p value; OR: odds ratio (Exp(B)); CI: confidence interval.
Nagelkerke R² = 0.14; Hosmer and Lemeshow = 9.039 (8), 0.339.
Nagelkerke R² = 0.115; Hosmer and Lemeshow = 0.941 (4), 0.919.
Multivariate logistic regression for factors associated with palliative care knowledge groups (DK = 1).
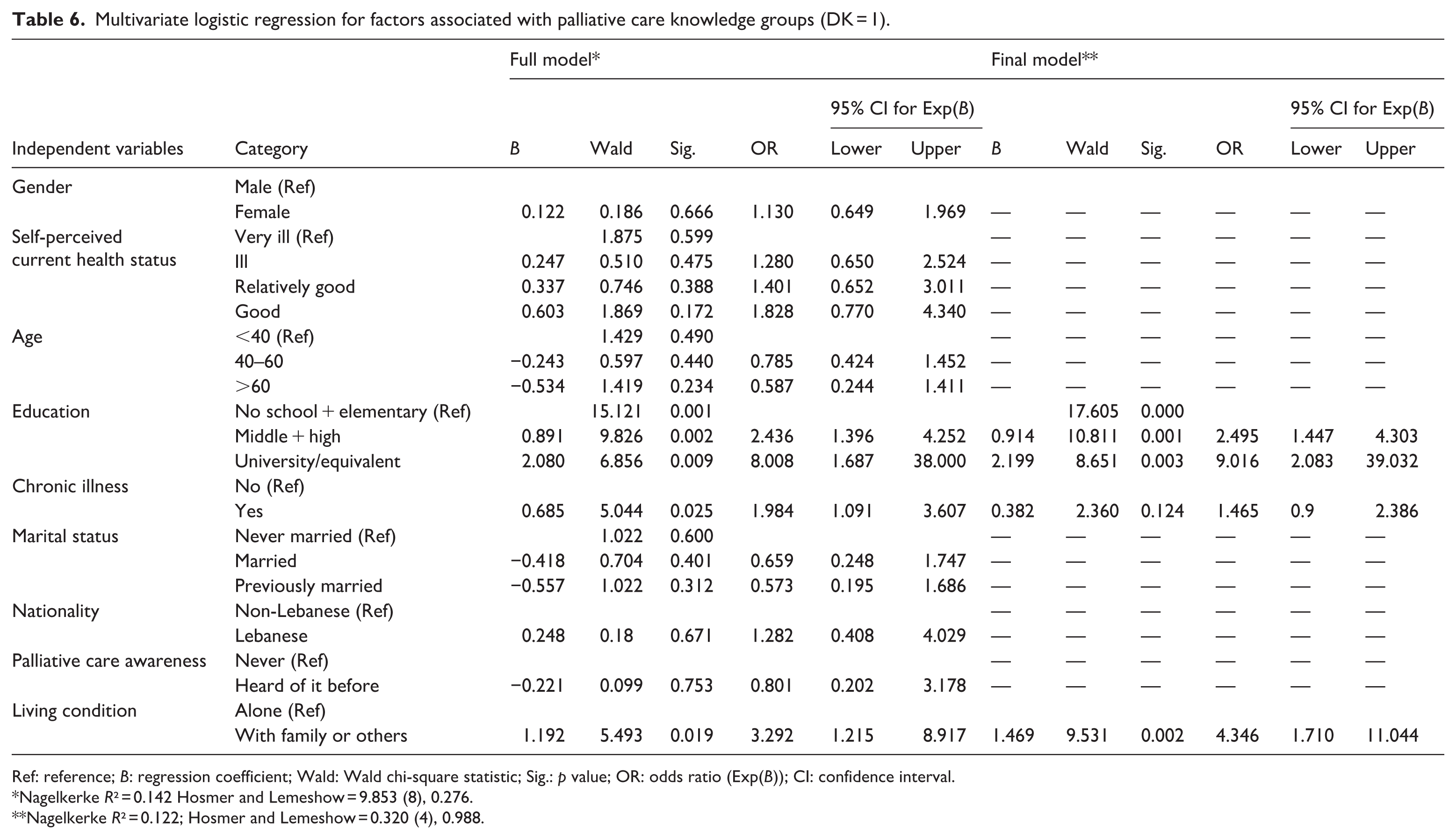
Ref: reference; B: regression coefficient; Wald: Wald chi-square statistic; Sig.: p value; OR: odds ratio (Exp(B)); CI: confidence interval.
Nagelkerke R² = 0.142 Hosmer and Lemeshow = 9.853 (8), 0.276.
Nagelkerke R² = 0.122; Hosmer and Lemeshow = 0.320 (4), 0.988.
Factors associated with common misconceptions
Multivariable binary logistic regression analysis using the backward stepwise selection method was conducted to identify factors associated with the three common misconceptions: palliative care is only provided in hospitals, palliative care is only provided during the last 6 months of life, and palliative care is only for cancer patients.
Higher educational attainment was strongly associated with lower odds of believing that palliative care is only provided in hospitals (middle/high school: OR = 0.56, p = 0.009; university-level: OR = 0.08, p < 0.001), while participants living with others had lower odds of holding this belief compared with those living alone (OR = 0.24, p = 0.017; Table 7). Participants older than 60 years had approximately twice the odds of endorsing the misconception that palliative care is only provided during the last 6 months of life (OR = 2.10, p = 0.035), whereas those with middle or high school education were significantly less likely to hold this belief compared to participants with low education (OR = 0.61, p = 0.029; Table 8). Participants with middle or high school education (OR = 0.46, p = 0.001) and those with university-level education (OR = 0.23, p = 0.001) were significantly less likely to hold the misconception that palliative care is only for cancer patients compared to those with low education (Table 9).
Multivariate logistic regression for factors associated with misconception 1—Palliative care is only delivered in hospitals.
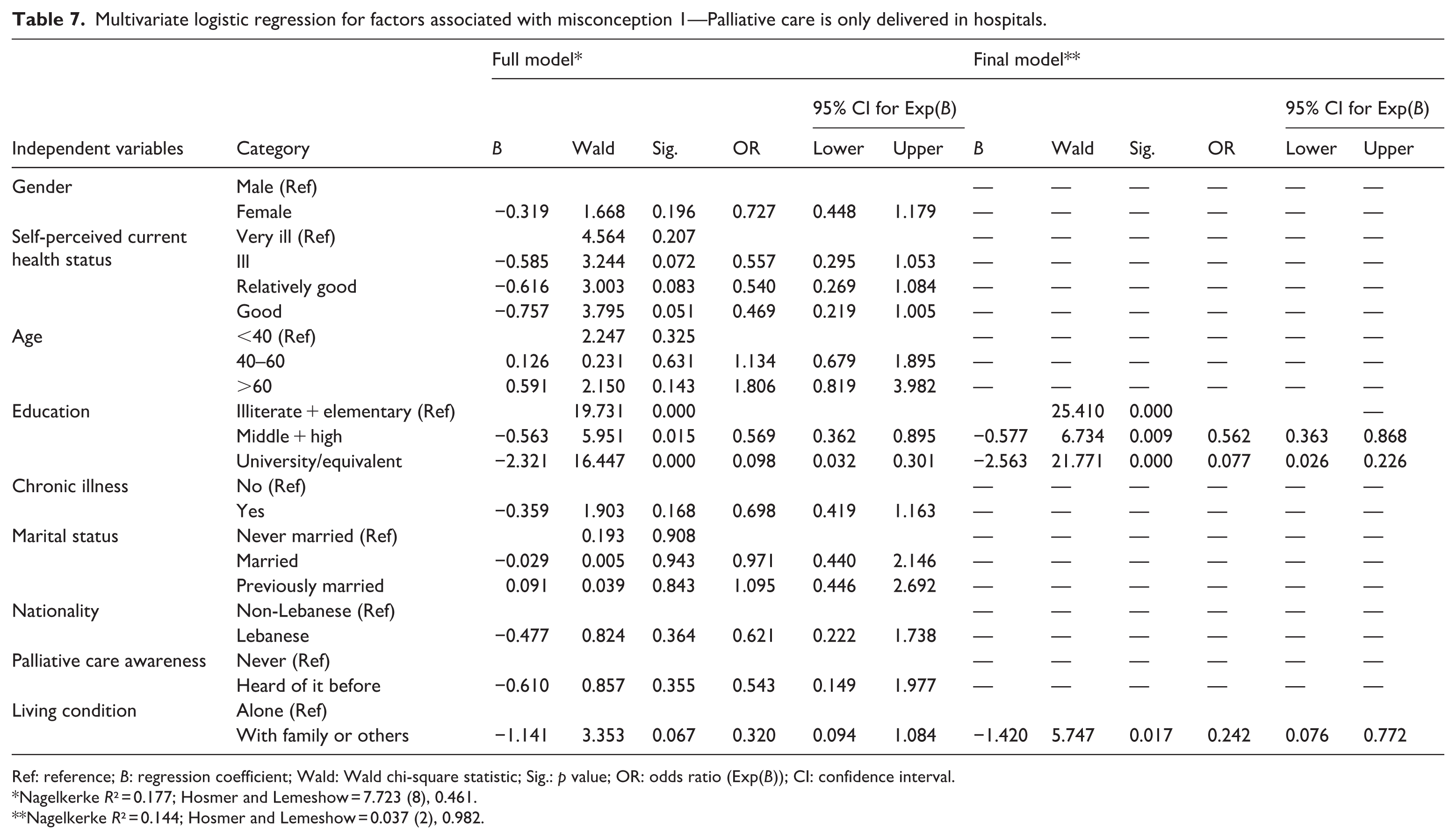
Ref: reference; B: regression coefficient; Wald: Wald chi-square statistic; Sig.: p value; OR: odds ratio (Exp(B)); CI: confidence interval.
Nagelkerke R² = 0.177; Hosmer and Lemeshow = 7.723 (8), 0.461.
Nagelkerke R² = 0.144; Hosmer and Lemeshow = 0.037 (2), 0.982.
Multivariate logistic regression for factors associated with misconception 2—Palliative care is for the last 6 months of life.
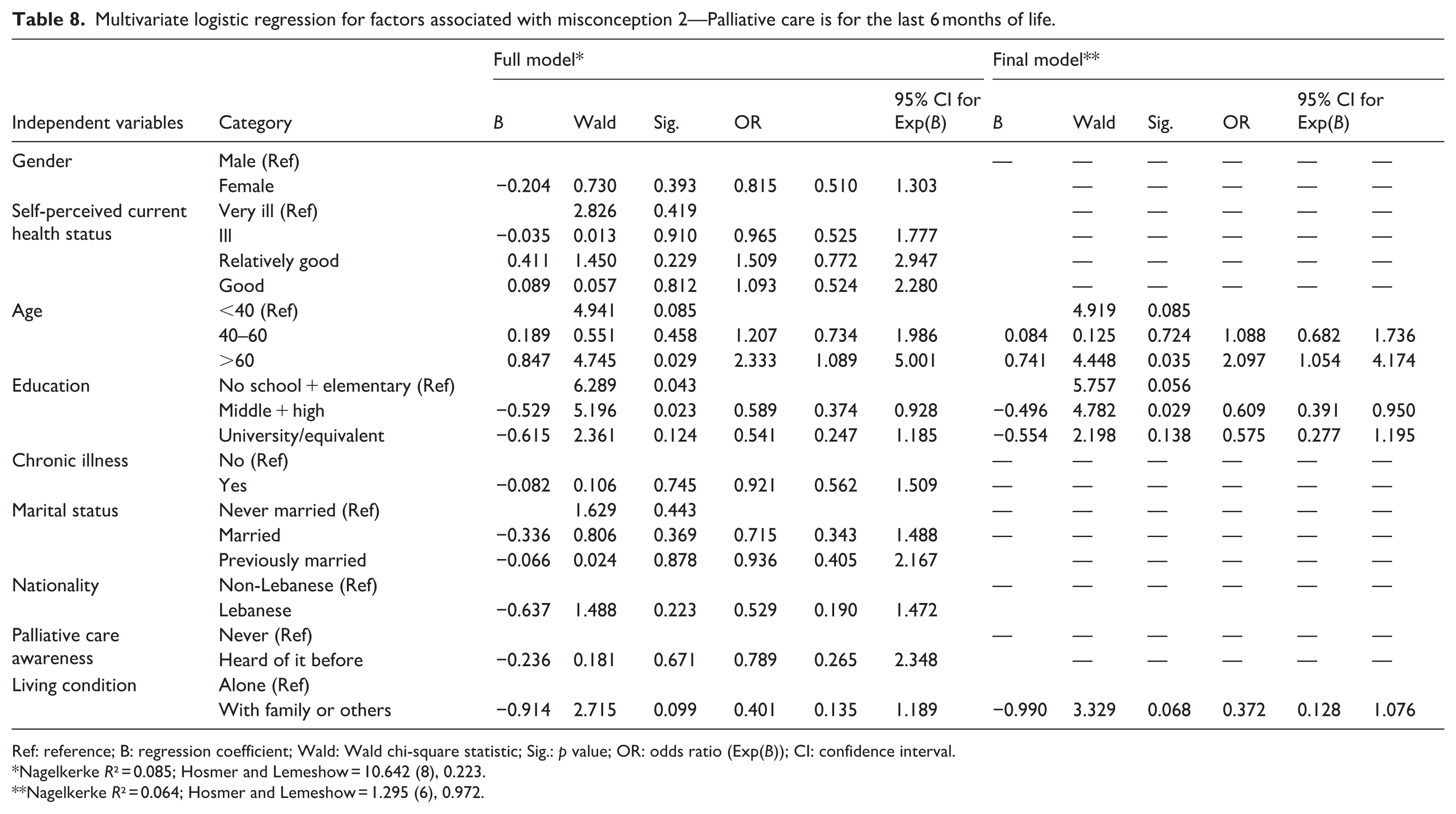
Ref: reference; B: regression coefficient; Wald: Wald chi-square statistic; Sig.: p value; OR: odds ratio (Exp(B)); CI: confidence interval.
Nagelkerke R² = 0.085; Hosmer and Lemeshow = 10.642 (8), 0.223.
Nagelkerke R² = 0.064; Hosmer and Lemeshow = 1.295 (6), 0.972.
Multivariate logistic regression for factors associated with misconception 3—Palliative care is only for people with cancer.

Ref: reference; B: regression coefficient; Wald: Wald chi-square statistic; Sig.: p value; OR: odds ratio (Exp(B)); CI: confidence interval.
Nagelkerke R² = 0.103; Hosmer and Lemeshow = 11.901 (8), 0.156.
Nagelkerke R² = 0.08; Hosmer and Lemeshow = 1.892 (2), 0.388.
Preferences for receiving information about palliative care
When asked about the preference to receive information about palliative care, 60% (N = 239) of participants preferred having information about palliative care be more generally available, 25% (N = 101) preferred information only in case of diagnosis with a life-threatening illness, 8% (N = 32) wanted it specifically if their life-threatening illness becomes terminal, while only 7% (N = 28) did not desire information about palliative care at any point. Preferences for receiving information about palliative care were not associated with demographics or level of knowledge.
Discussion
This is the first study that explores palliative care awareness and knowledge and identifies common misconceptions and associated factors among a socioeconomically disadvantaged community in Tripoli, north of Lebanon.
This study reveals a lack of awareness and the presence of several misconceptions about palliative care. The significantly high percentage of participants who never heard of the term “palliative care” 96% (N = 383), and the very low percentage of those who had previous experience with palliative care, 0.3% (N = 1), resembles the results of a survey study conducted in 2020. 31 The study, which was conducted in the capital and its suburbs, where most of the palliative care services are concentrated, showed that only 18.6% recognized the term “palliative care” without any explanations and 65.5% were totally unaware of the term “palliative care,” while as little as 2.7% had a direct experience with palliative care. 31 This significant lack of awareness of palliative care aligns with results of international studies 42 and studies in the region such as in the KSA (77.2%) 12 and Jordan (41.7%) 11 both of which have a longstanding history and notable development in palliative care services. In our study, the lack of awareness can be attributed to several factors. First, the absence of palliative care services in Tripoli at the time when the survey was conducted could have contributed to the lack of awareness. Palliative care is not yet fully integrated into the Lebanese healthcare system, including primary care, 9 and palliative care services are mostly concentrated in the capital, hence making “palliative care” a new terminology for the Tripolitan community in general and the disadvantaged communities in specific. Second, the term “palliative care” in Arabic might seem unfamiliar among the public and is more widely used by the healthcare community as the technical medical term. In Fneich and Adib study, 17.7% recognized the concept of palliative care after providing them with its definition, 31 suggesting that the terminology is not always self-explanatory. The equivalence of palliative care in Arabic is a literal translation of the English term and is used in Lebanon and the region with some minor derivations. However, there have been no studies conducted that explore whether such a literal translation is contextually and culturally relevant to the public. Third, awareness-raising efforts that target the public have been generally restricted to the efforts of community-based palliative care organizations with a limited reach. Recently, national efforts to enhance public awareness are being exerted as part of the National Cancer Plan palliative care chapter recommendations. 30 Lately, several awareness-raising sessions have been conducted across Lebanon targeting communities in different regions while aiming to open discussions about palliative care and its main concepts and dispel common misconceptions.
Despite the lack of awareness of palliative care, this study revealed moderate to high knowledge scores. The study conducted by Fneich and Adib revealed that almost 63% of those who successfully recognized palliative care had high knowledge scores compared to 37% who had low scores. 31 Our average PaCKS knowledge score was 9.2 compared to 6.8 in Jordan, 11 8.31 in the United Kingdom/Northern Ireland, 43 and 5.25 in the United States. 36 It is possible that our high knowledge scores are attributed to acquiescence bias, also known as “yea-saying,” where participants are more likely to agree with any statement, regardless of what it says. 44 Studies have shown that participants with low socioeconomic profiles and education are more likely to acquiescence. Given that this study targeted socioeconomically disadvantaged communities, and that over half of our participants (57.3%, N = 229) had either no schooling or had only completed elementary education, acquiescence bias could have contributed to the observed results. An acquiescence bias analysis was conducted by calculating the acquiescence bias score for each participant as the proportion of “True” answers out of their valid responses to the six false statements, thereby excluding DK answers from the denominator. The average acquiescence bias score representing the proportion of times participants answered “True as yea-saying” to the six false statements was 0.275 (SD = 0.289), which is substantially lower than the 0.50 rate expected from random chance or acquiescent responding. A one-sample t test was conducted to compare this sample mean against the hypothesized mean of 0.50. The results indicated a highly statistically significant difference (t(346) = −14.486, p < 0.001), with a mean difference of −0.22498 (95% CI: −0.2555 to −0.1944), indicating that participants did not exhibit a general “yes-saying” tendency, thereby invalidating acquiescence as a significant source of bias in these specific items. One statement “Palliative care is exclusively for people who are in the last six months of life,” was misunderstood and poorly received. Several participants mentioned during the data collection that only God could determine how long a person will live and as such correctly answered the statement as false, indicating a moral judgment rather than true knowledge. On the other hand, positively framed statements (80.2%) were answered correctly more often than false ones (60.3%; p = 0.00004). With more than half of the tool statements (7 out of 13) being positively framed, having high scores is expected despite participants’ unfamiliarity with the term “palliative care.” Statements indicating stress relief, psychological support, and symptom management reflect intuitive and caregiving-rooted practices making their endorsement natural.
In our study, education was a strong and stable predictor of palliative care knowledge across the different DK sensitivity analyses, thereby indicating a robust relationship that is not influenced by the assumptions of handling the DK responses. Furthermore, progressively higher odds were observed across higher educational levels, specifically those with university education in comparison to those with middle or high school education, potentially indicating a graded association and resonating with other studies conducted in the United Kingdom/Northern Ireland 43 and the Netherlands. 45 Our findings underscore the importance of health literacy in accessing information and understanding complex concepts such as palliative care and shed light on health inequities where low educational attainment, mainly linked to socioeconomic disadvantage, limits health literacy and access to information and resources. 19 Nationality was a significant predictor, with Lebanese having higher odds of higher palliative care knowledge, potentially reflecting the familiarity of Lebanese with the healthcare system and their increased exposure to serious illnesses, death, and dying that can be limited in non-Lebanese given the number of years lived in the country and their exposure to serious illnesses. Nevertheless, this finding should be interpreted with caution given the homogeneity of our sample and the very low sample size of non-Lebanese in our study.
This study exhibits three main misconceptions about palliative care. While some resonated with findings from other countries, others did not. Although the misconception that palliative care is exclusive to hospital care is not generally widespread, it was the most common in our study (51%, N = 204), resembling the findings from a study conducted in Portugal (60.2%). 46 Such a misconception might be attributed to the unavailability of home-based palliative care services in Tripoli at the time when the survey was conducted and to associating healthcare services with hospital care only. Having higher education and living with family or others were associated with lower odds of having this misconception, indicating the significance of health literacy, social support among families, and exposure to caregiving experience. Nevertheless, the finding related to living conditions should be treated with caution given the homogeneity of the sample and the low sample size of those living alone.
Linking palliative care to the last 6 months of life (47%, N = 188) came out as the second most common misconception associated with lower education and older age and resonated with other studies.36,43,45,46 In Lebanon, palliative care is associated with death and terminal diagnosis, and as such, is viewed as a last resort when all other treatments fail.47,48 This public misconception is reinforced by the late referrals of patients by primary physicians to palliative care services in Lebanon. There are no published studies that describe referral patterns; however, data obtained from the yearly operational metrics of a main home hospice service in Lebanon show a median length of stay of just 28 days over the past 10 years, increasing from 22 days in 2014 to 29 days in 2024. 49 Linking palliative care with cancer is the third common misconception associated with lower education and resonates with other studies.46,50 In Lebanon, this misconception is reinforced by the limited referrals by non-oncologists, where most referrals to palliative care are limited to cancer. 40 Physicians in Lebanon are viewed as a highly trusted source of information by the public when seeking (87.4%) or recommending (89.7%) palliative care, as indicated by Fneich and Adib 31 thereby highlighting the foundational role physicians can play to influence public knowledge and referral patterns.
Noticeably, after being introduced to the palliative care definition, most participants expressed a preference to access palliative care information regardless of their health status, suggesting openness, interest, and readiness to engage in palliative care discussions.
Strengths and limitations
This is the first study to assess palliative care awareness and knowledge among a socioeconomically disadvantaged population. However, generalizability is limited due to the use of convenience sampling approach and to the inclusion of participants from a single NGO. This study was administered by trained interviewers rather than being self-administered. This helped minimize missing data and increased participation rates; however, this could have resulted in interviewer and social desirability bias and influenced how participants responded, despite having well-trained interviewers. Another notable strength of this study is using colloquial Arabic for translating the PaCKS tool, which helped reduce misinterpretations by making sure to ask questions using the community’s dialect compared to Modern Standard Arabic. However, as a limitation, neither the study’s version of the tool nor other Arabic versions used in other studies have been validated. Our study also lacked cognitive interview testing of the survey. The qualitative finding encountered with some of the participants related to the statement “palliative care is exclusively for people who are in the last six months of life” indicates the need for addressing prognosis-related cultural/religious misconceptions and co-designing with the community culturally sensitive tools. Lastly, although the PaCKS is widely used to assess palliative care knowledge, the tool’s questions are limited to the clinical aspect of palliative care and do not reflect its community and human rights approach. 51
Conclusion and recommendations
This study sheds light on the lack of awareness and misconceptions about palliative care, especially among disadvantaged communities in Lebanon, highlighting the need for a collaborative, multi-sectoral system-thinking, community-centered, and equity-driven approach 52 that involves community, researchers, healthcare providers, and policymakers.
At the research level, community-based participatory research (CBPR) approaches are foundational to allow the co-creation and development of culturally sensitive tools and inform the development of effective public educational interventions. 53 This is especially important to reduce health inequities among disadvantaged groups by building trust and understanding the unique cultural and religious influences. Given the growing need to decolonize palliative care research54,55 and the predominance of Western-developed tools, researchers in Lebanon should use community-based research approaches to co-construct publicly meaningful language and definitions and identify aspects of good palliative care knowledge, thus informing public awareness initiatives.
At the community level, awareness initiatives are necessary to bridge the gap in palliative care understanding in Lebanon at both national and organizational levels. Future campaign development, implementation, and evaluation should go beyond traditional top-down towards participatory approaches that combine CBPR and social marketing methods, such as formative research, audience segmentation, and marketing principles approach 56 for better reach and effectiveness among disadvantaged populations.15–17 Social marketing has been shown to be effective in influencing different health behaviors globally 57 and is thus potentially promising in palliative care despite the limited evidence. Collaborating with religious leaders and institutions across sects is especially important in Lebanon to reduce stigma through cultural framing of campaign messaging. Furthermore, awareness initiatives should be tailored to the level of educational attainment by using innovative approaches such as storytelling, art-related activities, and community discussions conducted through traditional and social media platforms, thus maximizing reach and engagement. Most importantly, initiatives should focus on strengthening compassionate communities. In Lebanon, strong family and community ties remain prevalent, and many individuals are willing to support one another; however, lack the necessary knowledge and skills required. Capacity-building interventions that enhance communication, emotional support, and caregiving skills are essential. Families who have received palliative care represent a key resource for such initiatives including community education and peer-support groups.
At the healthcare system and policy level, early integration of palliative care into all levels of care, including primary care and non-cancer diagnoses, is essential to address misconceptions and increase equitable access to palliative care. National efforts to frame palliative care services and related initiatives beyond cancer necessitate reviving the development of a national palliative care strategic plan. Capacity-building initiatives addressing healthcare professionals should address misconceptions and reinforce community participatory approaches where patients and families are viewed as partners in care. Healthcare professionals should use culturally sensitive communication strategies that consider educational attainment and health literacy levels; allocate adequate time for palliative care discussions; actively involve patients and family members; and use accessible educational material such as short videos and illustrations. 18 Nevertheless, interventions that would enhance organizational, professional, and personal health literacy should be systematically integrated into routine healthcare to strengthen understanding and uptake of palliative care. 19
As palliative care in Lebanon continues to develop, implementing these recommendations will require national efforts led by the Ministry of Public Health and anchored in collaboration among researchers from academic institutions, clinicians from hospitals and community-based organizations, and community members.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524261449268 – Supplemental material for Awareness and knowledge of palliative care in Tripoli, Lebanon: A cross-sectional study in a disadvantaged population
Supplemental material, sj-docx-1-pcr-10.1177_26323524261449268 for Awareness and knowledge of palliative care in Tripoli, Lebanon: A cross-sectional study in a disadvantaged population by Farah Demachkieh, Ahmed Kassab, Mouhamad Darwich, Lea Chaiban, Dalal Kasir, Yomn Rafaela Naji, Zein Adra, Sahar Jamal, Nayla Nahas and Zeina Dassouki in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524261449268 – Supplemental material for Awareness and knowledge of palliative care in Tripoli, Lebanon: A cross-sectional study in a disadvantaged population
Supplemental material, sj-docx-2-pcr-10.1177_26323524261449268 for Awareness and knowledge of palliative care in Tripoli, Lebanon: A cross-sectional study in a disadvantaged population by Farah Demachkieh, Ahmed Kassab, Mouhamad Darwich, Lea Chaiban, Dalal Kasir, Yomn Rafaela Naji, Zein Adra, Sahar Jamal, Nayla Nahas and Zeina Dassouki in Palliative Care and Social Practice
Footnotes
Acknowledgements
The authors are grateful to the non-governmental organization in Tripoli for facilitating data collection, as well as to all the participants for their valuable contributions. The authors also acknowledge the technical support provided by Mr. Ayman Abdou throughout the revision process.
Ethical considerations
Ethical approval was sought and obtained from the DCCPS/Institutional Review Board (IRB) at the University of Balamand on January 12, 2023, DCCPS/IRB120123.
Consent to participate
All eligible participants were informed about the study, participants who agreed to participate were required to sign a consent form or provide their fingerprint as a form of signature. In case participants can’t read or write, an additional research assistant was present during the consent process as a witness.
Consent for publication
All authors approved the final version of the article to be published and take public responsibility for appropriate portions of the content.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data may be available on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.