
Abstract
Background:
Compassionate communities are a key public health palliative care strategy for addressing the social determinants of death. However, their evaluations often prioritize health indicators, overlooking the intended social and cultural transformations that are central to this social model. This study addresses this research gap by analyzing the transformative outcomes emerging from two distinct community initiatives.
Methods:
Building on our prior analysis of community engagement processes, this comparative ethnographic analysis examines the transformative outcomes of two distinct compassionate communities in Montréal, Canada (2021–2023). Data from 84 h of participant observation and 26 semi-structured interviews with 22 participants were analyzed to identify the social and cultural changes resulting from the community-led and institutionally-led models.
Results:
Findings demonstrate that local contexts act as active forces shaping which social determinants of death are prioritized, specifically overdose stigma in Centre-Sud and fraud-induced social death in the West Island, thereby dictating unique engagement trajectories toward transformation. A universal outcome was the creation of safe spaces to break the death taboo, which addressed the mismatch between private loss and the lack of collective social scripts. This facilitated the emergence of “death sociability”: a reciprocal mechanism for experiential learning grounded in shared recognition of human finitude, which actively builds cultural capital in its embodied (new skills and language), objectified (rituals and shared narratives), and institutionalized (formal recognition of community practices) forms.
Conclusion:
Death sociability is a core mechanism through which compassionate communities achieve transformative change, addressing both biological and social mortalities. As an empirically grounded concept, it offers a novel theoretical lens for future research to track social and cultural impacts beyond health metrics. Therefore, supporting the creation of safe spaces where death sociability can thrive is crucial for building the cultural capital needed to advance equity in social determinants of death.
Plain language summary
This study explored the social and cultural transformations within “compassionate communities,” local initiatives supporting those experiencing serious illness, death, and grief. We aimed to understand how these projects change the way people relate to mortality.
For three years, our research team followed two distinct Montréal projects: a grassroots, community-led effort and an institutionally-led initiative. We analyzed their impact through 84 hours of participant observation and 26 interviews with 22 participants.
We found that local settings acted as active forces, shaping how each community addressed its unique needs. For instance, programs tackled challenges such as the stigma of drug overdoses or “social death”—the profound separation from community life caused by the shame and isolation felt by victims of senior fraud. Despite their different paths, both projects successfully created “safe spaces” to bridge the gap between private loss and grief and a society that often lacks the rituals or social “scripts” needed to discuss loss.
In these spaces, a powerful process we call “death sociability” emerged. Participants formed reciprocal relationships to learn from one another’s experiences, building lasting community resources like new skills for discussing loss and shared rituals to honor the dead. By addressing both the physical and social aspects of mortality, these initiatives foster the human connection needed for a more equitable and human-centered approach to death, dying, and grief.
Keywords
Reclaiming death as a social experience: The role of compassionate communities
A public health approach to palliative care operates as a social model targeting the determinants of living with a life-limiting illness, caregiving, grief, and loss.1,2 This approach places community support at the center of its collective action, sourcing it from a synergistic and dynamic partnership of neighborhood, community, and wider civic-sector action. This social model is realized through a range of community-led initiatives, based on social ecology, health promotion, and public education (death literacy) strategies, with compassionate communities serving as a key community development model. 3
Compassionate communities are defined as community-led initiatives that mobilize citizens to address the social determinants of death. 1 These determinants include the structural conditions, such as income, access to services, and social support, that “determine not only how people live but also how they die and grieve.” 2 Throughout this paper, we use the term “social determinants of death” to broadly encompass the structural forces shaping the full continuum of experiences with death (including social death): serious illness, end-of-life, dying, loss, and bereavement. Compassionate community initiatives engage with communities to identify local needs, co-create solutions, coordinate intersectoral action, and advocate for death and end-of-life care as a collective responsibility to reduce health and social inequalities. 1 This social movement has gained global traction, with initiatives adapting to diverse cultural landscapes ranging from Latin America 4 to East Asia,2,5 Europe,1–3,6,7 and North America. 8 Yet, empirical research on how these local contexts shape engagement remains limited.4–8
While compassionate communities are a primary strategy for enacting this social model, empirical research exploring the interplay between context, engagement, and social outcomes remains scarce.4–8 Existing compassionate community evaluations often prioritize health indicators, overlooking the intended social and cultural transformations.8–10 This research gap stands in contrast to the urgent call from the Lancet Commission on the Value of Death for a radical transformation of the Western relationships with death. 2 Grounded in Rawls’s 11 political philosophy, the concept of a “realistic utopia” serves as the Commission’s normative framework. 2 It envisions a radical yet achievable rebalancing of power: moving from a system where death is the sole domain of health professionals to one where communities reclaim their essential role in dying, caregiving, and grieving. This vision provides a practical roadmap built on five public health palliative care principles: (1) addressing the social determinants of death; (2) viewing dying as a relational process; (3) building networks of care; (4) breaking the silence surrounding mortality; and (5) recognizing value in death. The original contribution of this study is to highlight these overlooked social and cultural changes as vital public health outcomes of compassionate communities.
To address this gap, this article presents a comparative ethnographic analysis of two culturally distinct compassionate community initiatives in Montréal, Canada. Building on our previous work, which detailed how local contexts shaped community engagement processes and development trajectories, 12 this study asks: “how do context-sensitive engagement processes translate into concrete social and cultural transformations within these communities?” This study focuses on the resulting programs and the specific social and cultural transformations observed. We demonstrate that despite divergent, context-sensitive pathways—one a grassroots, community-led model and the other combining institutionally-led and community-led approaches—both communities achieved similar transformative outcomes.
Methods
Study design and approach
The comprehensive methodological framework for this study is detailed in our previously published protocol. 8 Employing a comparative ethnographic design, we utilized immersive, contextualized observation and analysis to explore participants’ lived experiences, behaviors, and social interactions within their natural settings. 13 This approach was selected to understand how local contexts shaped community engagement and to compare the resulting variations in development trajectories, results, and outcomes across culturally diverse compassionate community initiatives over a 3-year period (2021–2023).
Research setting and case selection
Supported by philanthropic funds, this study was a collaborative effort initiated by a non-profit Palliative Care Residence with an academic research team specializing in community partnership science. The interdisciplinary team was composed of clinicians, community members, a patient-partner, and researchers from diverse fields (including anthropology, community psychology, medicine, public health, and sociology), with complementary expertise in community engagement, participatory research, palliative and end-of-life care, and social innovation.
Two culturally contrasting neighborhoods in Montréal, Centre-Sud and West Island, were strategically selected to establish clear case boundaries. These neighborhoods exhibit distinct socio-cultural profiles, including variations in language (French/English), socioeconomic status (affluent/less affluent), and age demographics (older/younger), making them suitable for comparative ethnographic research. West Island represents the catchment area of the Palliative Care Residence. Centre-Sud was chosen for its demographic diversity and potential to engage with marginalized populations, aligning with the study’s objectives.
Key features of Centre-Sud and West Island local contexts
Centre-Sud and the West Island, while both within Montréal, have contrasting local contexts that significantly shaped the development and outcomes of their respective compassionate community initiatives. Centre-Sud, a densely populated urban core, is marked by high social diversity and a concentration of marginalized populations (people using drugs, experiencing homelessness, LGBTQ+ community, refugees, and sex workers). This historically working-class neighborhood benefits from a well-established network of community organizations that foster a strong collaborative culture. Conversely, the West Island is a sprawling suburban territory with a predominantly English-speaking population and a higher average socioeconomic status. With nearly half its population over 65, it faces unique challenges related to aging and caregiving in a competitive landscape for community resources. As the community engagement processes and development trajectories were detailed in our prior work, 12 these contextual differences are now crucial for understanding how it influenced the implemented programs, observed and perceived outcomes, and socio-cultural transformations detailed below.
Participants
For this study, participants were drawn from three principal groups across both community sites:
1. Compassionate community facilitators: This group consisted of the individuals tasked with guiding the initiatives. Their responsibilities included community outreach, event organization, support for co-design processes, and the facilitation of governance structures.
2. Community organization representatives: This category comprised staff and members from local partner community and health organizations who were actively involved in the development of the compassionate community initiatives, such as those serving on the Centre-Sud governance committee or the West Island’s Community Seniors Table.
3. Citizens, patients, and community members: This general group included any local residents, patients, or other community members who took part in public-facing activities sponsored by the initiatives, such as workshops and citizen forums.
Eligibility to participate in this study was to be adults (18 years of age and older) able to provide informed consent. Recruitment strategy was purposive sampling of people engaged in a compassionate community.
Action-research team
To ensure methodological rigor and acknowledge our own positionality, the research team adopted established ethnographic roles, utilizing an “emic” (insider), an “etic” (outsider), and a “bridge” perspective.14–16 This approach allowed for a multi-perspective analysis to mitigate bias and capture the nuances of each community context. The roles were defined as follows:
“Inside” researchers (C.L., D.W., L.J., S.D.): These team members led and facilitated the community engagement activities, serving as both action-researchers and participants, providing an emic perspective.
“Outside” researchers (A.B., A.K., G.R., I.M., L.S.): This group held scientific responsibility for the project, providing research-driven guidance on its design, methodology, and knowledge translation. They were not involved in data collection or analysis, thus maintaining an etic perspective.
“Bridge” researcher (E.L.): The lead author acted as both an observer of and a participant in the development activities. In this role, she conducted real-time data collection and analysis, serving as a liaison between community members and the “insider” and “outsider” researchers.
This multi-perspective approach fostered a more holistic understanding of the contextual factors influencing the engagement, development, and outcomes of both compassionate communities.
Data collection
Data were collected between February 2021 and December 2023, concurrent with ongoing community engagement and development activities. In keeping with our comparative ethnographic design, the study utilized two primary methods to identify social changes and cultural transformations within the two compassionate communities: participant observation and semi-structured interviews.
Participant observation
Initial observations were conducted on virtual platforms (Zoom) due to COVID-19 pandemic restrictions in Quebec (March 2020–May 2022), with in-person activities resuming as restrictions eased. The observation strategy was specifically designed to address the knowledge gap regarding social and cultural transformations. Therefore, the focus was on documenting shifts in practices, attitudes, and discourses that reflected the principles of realistic utopia (e.g., how participants shared stories about dying and grief and found value in death). A total of 63 h of participant observation was conducted in Centre-Sud and 21 h in West Island. As detailed in our prior work, 10 this disparity stemmed from pandemic-related delays, which acted as a facilitator in Centre-Sud while serving as a barrier in the West Island.
The lead author (E.L.) conducted all participant observation, embedding herself within community mobilization and development activities such as governance meetings, co-designed programs, and citizen forums. A key methodological concern was establishing reciprocal relationships to bridge the dual roles of fieldwork and research. To this end, (E.L.) actively contributed to project development by sharing knowledge and connecting partners, while also providing logistical, practical, and emotional support to the team. Her inclusion in relevant meetings was facilitated by other members of the research team (C.L., L.J., S.D., D.W.). At each event, virtual and in-person, she introduced herself, explained the study’s purpose and her role as an observer, and informed participants of their right to decline observation at any time (none declined). Participant observation notes were taken by hand during activities and later transcribed digitally for analysis.
Semi-structured interviews
Semi-structured interviews, recorded and transcribed with participant consent, were conducted with participants from both the Centre-Sud and West Island compassionate communities using a purposive sampling strategy. The number of participants was adjusted throughout the study to account for staff turnover and the inclusion of new partners. To ensure interviewees had sufficient knowledge of the initiatives, community partners were interviewed in the final year of the study (2023), while interviews with the project’s facilitators and leader were conducted annually from 2021 to 2023. The sole inclusion criterion for all interviewees was their direct involvement in the development of a compassionate community initiative.
A total of 26 semi-structured interviews were conducted with 22 unique participants, including community engagement facilitators (n = 5), project leader (n = 1), and community partners engaged in the development of a compassionate community (n = 16). For Centre-Sud, the interviewed participants (n = 14) were community engagement coordinators (n = 3) and community partners (n = 11). For West Island, interviewed participants (n = 8) were community engagement coordinators (n = 2), project manager (n = 1), and community members involved in the development of the compassionate community (n = 5).
Data analysis
Our analytical approach integrated concept-driven research 17 with thematic lens analysis. 18 Data from participant observation and semi-structured interviews were analyzed using the five public health palliative care principles as a guiding thematic lens. This framework, consistent with its application in our previous work, 12 allowed for a systematic analysis of social patterns to identify and track social changes (e.g., viewing death as a social process) and cultural transformations (e.g., breaking the taboo of death).
The first author conducted the initial qualitative analysis, including coding and categorization, using QSR NVivo 12 software to facilitate intra- and inter-case comparisons. As AI is increasingly recognized as a valid tool for interpreting qualitative data,19–21 we choose Gemini to support our comparative analysis, a large language model architecture distinct from models like ChatGPT. 22 Chosen for its superior multilingual capabilities, crucial for analyzing the subtleties of our Quebec French data, Gemini processes large context windows while treating each prompt as an independent, stateless interaction within a secure enterprise environment where data is not used for model training. 22
Ethical considerations regarding data privacy (compliance with the General Data Protection Regulation [GDPR]) 23 were strictly managed: all input data was fully anonymized and de-identified. The role of AI was confined to two support functions: (1) to validate overarching patterns and help detect subtle variations across the preliminary findings by specifically prompting the model to identify “similarities or differences in the engagement processes, development trajectories, and changes”; and (2) ensuring the fidelity of English translations and enhancing the manuscript’s readability. To ensure robust human oversight, a multi-step validation process was employed: the lead author critically reviewed all AI-generated outputs, and consolidated findings were presented to the action-research teams and community partners for member validation and feedback. The first author retained full authority over all final analytic decisions.
Results
This section presents the results of our comparative ethnographic study. We begin with a concise overview of the local contexts, as previously detailed, 12 which is crucial for interpreting the subsequent analysis of program implementation, outcomes, and the broader social and cultural transformations observed in each community.
Shared goals, diverse approaches, different outcomes
Our ethnography documented the key social and cultural changes that emerged from the two compassionate communities’ distinct development pathways. Following a community-led engagement strategy, six compassionate programs in Centre-Sud were co-designed and implemented with community partners. In contrast, the institutionally-led model in the West Island resulted in a mixture of five co-designed and pre-packaged programs. Tables 1 and 2 provide a detailed overview of these initiatives, including their specific objectives based on local needs, the populations they reached, and their observed outcomes, which will be analyzed in the following sections.
Compassionate Community Activity Outcomes in Centre-Sud (2021–2023).
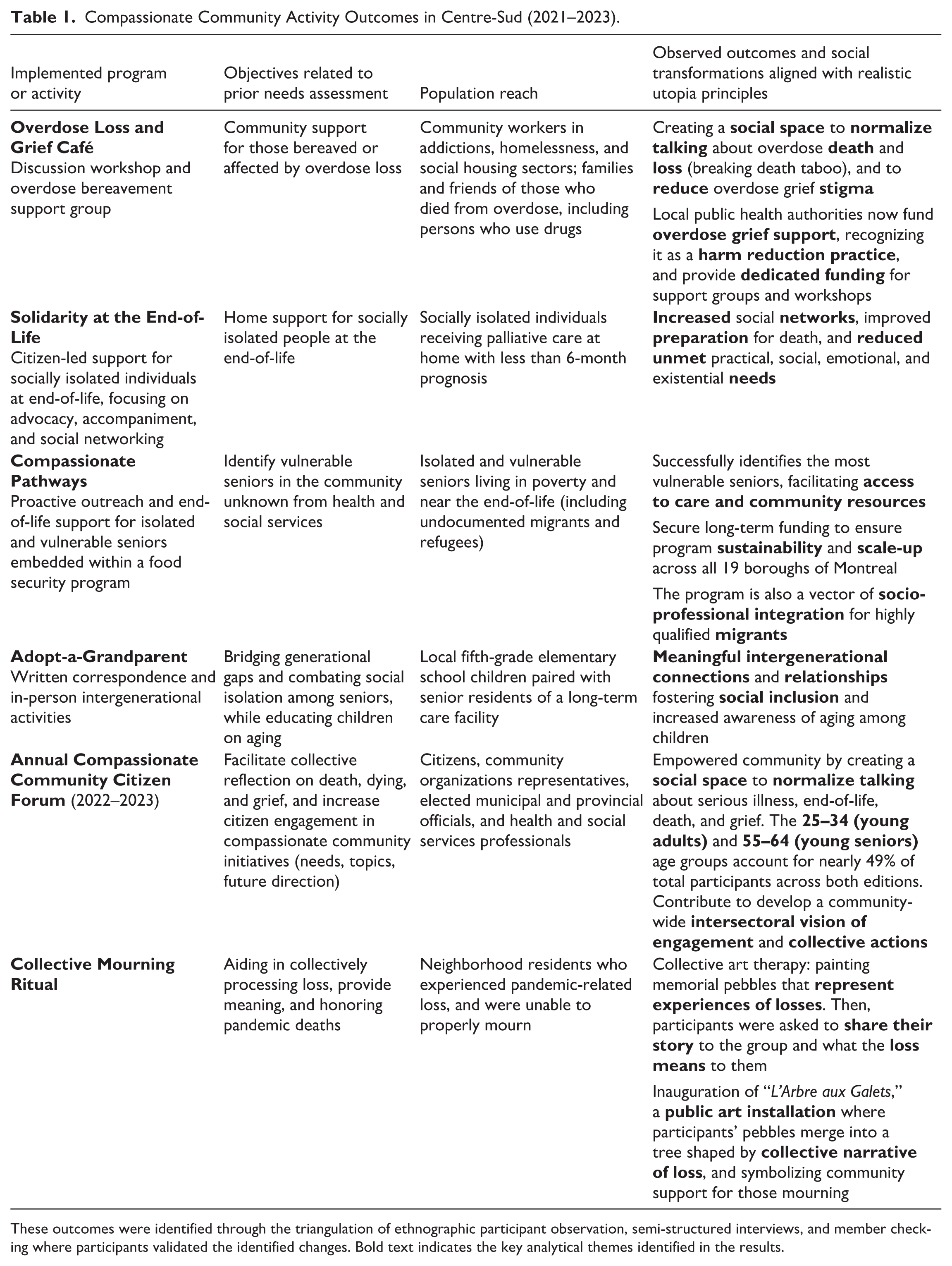
These outcomes were identified through the triangulation of ethnographic participant observation, semi-structured interviews, and member checking where participants validated the identified changes. Bold text indicates the key analytical themes identified in the results.
Compassionate Community Activity Outcomes in the West Island (2021–2023).
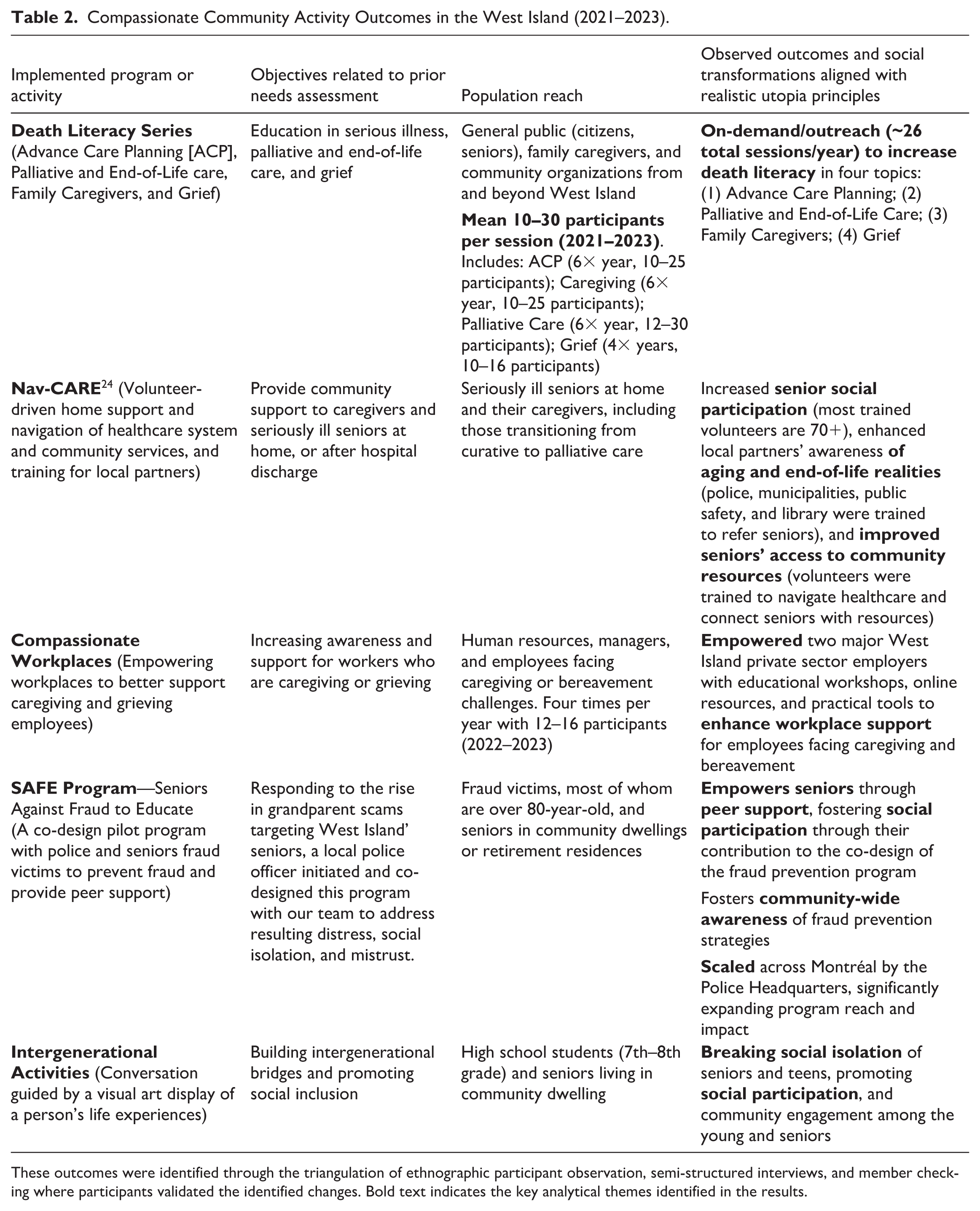
These outcomes were identified through the triangulation of ethnographic participant observation, semi-structured interviews, and member checking where participants validated the identified changes. Bold text indicates the key analytical themes identified in the results.
Social and cultural changes as a ripple effect of community engagement
Our analysis reveals key mechanisms driving change. Despite variations in context and approach, both communities demonstrated similar transformations: (1) the expansion and strengthening of support networks (e.g., peer bonding, intersectoral collaboration); (2) the integration of compassionate practices into the workplace and schools cultures to reach citizens of all ages in their daily environments; and (3) the cultivation of a broader culture of compassion by normalizing discussions about death and addressing social determinants of death (e.g., safe spaces reversing structural silence). Specifically, our findings identify two promising transformative practices with the potential to profoundly reshape our relationship with death: creating safe spaces for discussing death and promoting intersectoral collaboration to better address social determinants of death. To support these findings and illustrate the common need for safe spaces across diverse populations, we now report on the changes observed within and across Centre-Sud and West Island compassionate communities.
Breaking the taboo: Safe spaces for discussing death
A central finding of our ethnography is that the creation of safe spaces was a direct response to social determinants of death, the wider social forces that shape how people live, die, and grieve. In Centre-Sud, community workers routinely encounter death in their daily work with vulnerable populations, which include seniors with intellectual disabilities, LGBTQ+ community, people who use drugs, experiencing homelessness or poverty, and people living with HIV. Yet, a significant barrier to providing adequate support is the prevailing taboo surrounding death. Laurence, a harm reduction worker in Centre-Sud, explains that the lack of space to talk about the repeated death and grief they experienced leads to burnout: If our workers keep burning out from dealing with so much repeated violent grief (. . .) And there’s no place in those [harm reduction] environments to talk about it. And I think it’s important that it be part of the curriculum of these organizations. Then, I think with compassionate communities, it’s something we can do.
For the workers in the homelessness sector, engaging with the compassionate community initiative directly influenced their practice: “Simply discussing death has an effect on the way we intervene” (Field notes, Centre-Sud_2021-12-03). This led some to feel more comfortable discussing end-of-life wishes and integrating grief support into their follow-ups.
The first Citizen Forum in 2022 provided a striking example of this need for safe spaces. The opening conference transformed into a space for the social recognition of grief after the speaker shared his experience about his step-daughter’s suicide. This story created a breach in the death taboo, paving the way for others in the subsequent Q&A session to share their own experiences with stigmatized loss: a bereaved mother spoke of the shame following her daughter’s overdose, and another participant discussed the isolation of those who die alone (Field notes, Centre-Sud Citizen Forum_2022-05-11). This emphasis on open expression continued throughout the subsequent workshops, where participants prioritized sharing their experiences with death and bereavement over their introductions and discussion topic.
The second Citizen Forum in 2023 showed how these needs were addressed programmatically. The hosts of the Overdose Loss and Grief Café explained the benefit of pairing individuals with lived experience of substance use with bereaved parents. This was powerfully illustrated when such a pair co-chaired the opening conference, with the bereaved mother’s concluding call to action: “Shame kills more than a grain of Fentanyl,” directly confronting the stigma surrounding drug-related deaths. This statement is a stark illustration of how participants themselves identify shame and stigma as social determinants perceived as more lethal than the substance itself. Subsequently, in a workshop on ritual, another Café host explained that introducing a candlelight ritual for those lost to overdose: “reinforces belonging, social cohesion, and the sense of community,” demonstrating how these initiatives build new social bonds to counteract stigma (Field notes, Centre-Sud, 2023-05-10). Observations indicate that these encounters built crucial bridges, fostering the mutual understanding and solidarity pivotal to deprofessionalizing addiction and overdose grief. Integrating lived experiences complement professionally-led interventions while concurrently generating meaning, hope, and change (Field notes, Centre-Sud, 2023-05-10).
Similarly in the West Island, the 10 senior fraud victims participating in the SAFE program’s co-design discovered that the process itself offered a safe space to discuss the emotional impact of their loss, revealing a broader need for such spaces. One participant summed up the common experience of the grandparents’ scams victims: “It’s the first time I even talk about it. I never told my husband or my children because I was so ashamed” (Field notes, West Island, 2023-04-24). This need became even more evident at the second co-design meeting, where the SAFE program’s components were validated, as a woman requested to retell her fraud story despite having already shared it 2 months earlier (Field notes, West Island_2023-06-26). This highlights the seniors’ need for social recognition of their loss, encompassing not only financial repercussions but also shame, guilt, social isolation, and loss of trust that can even lead to suicide (Field notes, West Island, 2023-06-26). By creating a dedicated space for these non-illness-related losses, the initiative directly addressed the social determinants such as shame and isolation, that can lead to life-threatening consequences.
Across both communities, this process of creating safe spaces fostered social recognition and community support. It facilitated a collective narrative woven from individual experiences that helped break down taboos, strengthen community bonds, and enhance death literacy. This demonstrates that breaking the death taboo is a broad social imperative, relevant beyond those with immediate palliative needs. Despite their distinct socio-demographic contexts and community dynamics, both Centre-Sud and the West Island revealed a profound common need for safe spaces to share experiences with death, grief, and loss, demonstrating the universality of such experiences and the societal need to normalize their discussion.
Fostering compassionate cultures: Addressing social determinants of death through intersectoral collaboration
According to participants, a broader cultural transformation occurred as partner organizations, through intersectoral collaboration, began to collectively identify and respond to the social determinants of death. This engagement fostered an understanding that death is a shared human experience transcending professional boundaries, which in turn spurred a transformation within partner organizations toward becoming more compassionate workplaces. For example, initiatives like “Compassionate Pathways,” “Overdose Loss & Grief Support,” and “Solidarity at the End-of-Life” provided the foundation for this shift by bringing together diverse community workers, health and social care professionals, and palliative care volunteers.
In Centre-Sud, interviewed steering committee members (n = 8) reported that this collaboration led to an increased awareness of their own biases, prompting them to adjust their practices. For example, Camille, a community worker in the intellectual disability sector, used her membership in the Compassionate Community Montréal to promote awareness about the unique end-of-life needs of seniors with intellectual disability among residential care facility professionals (Field notes, Centre-Sud, 2023-05-10). Stéphanie, a community HIV worker, reported creating dedicated spaces within her organizations for such discussions: We had taken the time to think about people and the question of death. It’s very. . .I realize that in the HIV community, it’s very difficult to talk about death because often, they’ve known several people who have died.
This new awareness and sense of belonging also increased motivation, and improved understanding of how to compassionately address death-related needs: The team was deeply moved and inspired when they learned about the project’s impact on the community. They felt a strong sense of belonging and pride in being part of something that was making a real difference, directly or indirectly. Jean-Baptiste, Compassionate Pathways leader
This growing awareness within Centre-Sud fostered a paradigm shift: moving beyond a medicalized view of death to embrace its fundamentally social and human nature, acknowledging the collective responsibility in providing social care and community support.
In the West Island, this cultural transformation took a different path. A key barrier to addressing community needs was the pre-existing distrust toward the Palliative Care Residence, which, as previously reported by Patricia, a senior’s home support director, had operated in isolation prior to the project (Lessard et al.
12
, p. 7). To navigate this, the Residence adopted a multi-strategic approach to build partnerships, which required a profound internal transformation from being a central palliative care provider to a community facilitator. Elizabeth, the project leader, reflect on this shift: When we control or even engage others to do their own things, it’s about learning from what already exists. . . That’s what will ultimately fuel a sharing of ideas. . . That’s why I say we must take advantage of what is already there. And build on that. And we don’t only have to do our own projects or initiatives. So that has changed.
This quote reflects a fundamental shift in the Residence’s perspective, demonstrating the internal cultural change that was necessary to enable broader intersectoral collaboration and achieve successful partnerships.
Finally, as shown in Table 2, two specific West Island compassionate initiatives extended their reach into citizens’ daily environments. The Compassionate Workplaces program engaged and empowered human resources managers and employees from two major private sector employers to enhance support for staff facing caregiving or bereavement. Simultaneously, Intergenerational activities connected high school students (7th–8th grade) with seniors in community dwellings. Beyond breaking social isolation for both groups (especially at the end of the COVID pandemic), this initiative promoted community engagement among a future generation, fostering social participation for both the participating seniors and the teens.
Comparative synthesis of social and cultural transformations
Comparing the two communities reveals both a common pattern and distinct trajectories. The need for safe spaces proved to be a universal finding, stemming from the pervasive taboo surrounding death. In both sites, community engagement processes actively confronted this taboo, fostering a broader development of compassionate cultures. Building on this common foundation, the nature of the cultural transformations varied. In Centre-Sud, the community-led approach empowered community partners to recognize their own capacity to provide support, challenging the notion that palliative care is solely the domain of health professionals. Conversely, in the West Island, the key transformation was internal to the Palliative Care Residence as it opened up to the community, a shift driven by its multi-strategic, institutionally-led approach. In both contexts, these engagement processes led partners to integrate new knowledge about death into their workplace cultures, highlighting a growing sense of collective responsibility. These changes in social practices reverberate across the community, contributing to cultural transformations in the relationship with death with effects that surpass what research can fully capture, measure, and quantify.
Discussion
This comparative ethnography demonstrates that co-designing initiatives rooted in local context actively translates engagement into tangible social and cultural transformations, specifically by fostering safe spaces and death sociability. Yet, our findings highlight a compelling duality: while the fundamental need for safe spaces to break the death taboo emerged as a universal driver of engagement, the pathways toward cultural transformation diverged significantly based on local context and engagement processes strategy. Our findings suggest that successful compassionate community development and its outcomes depend less on prescribed models and more on context-sensitive strategies that foster collective engagement, whether initiated organically or through institutional adaptation. 10
This emphasis on context-sensitive processes resonates with a growing body of evidence. For instance, two complementary studies in Belgium offer key insights: a cross-sectional survey by D’Eer et al. 25 found that neighborhood participation is strongly associated with prior personal experience and perceived social cohesion, while a detailed process evaluation by Quintiens et al. 9 revealed that top-down, city-led initiatives faced significant barriers related to bureaucracy and stakeholder frustration, highlighting the importance of the existing social fabric. In Germany, a qualitative formative evaluation by Meesters et al. 26 shows that a blend of community engagement strategies is often necessary but difficult to manage. While international efforts rightly seek standardized outcomes for benchmarking, 27 Pesut et al. 24 found that implementing structured compassionate programs like Nav-CARE requires significant local adaptation, particularly “skillful messaging” to avoid stigma, to ensure feasibility and acceptability. Our ethnographic findings demonstrate that local contexts are not merely settings but active forces that shape how social determinants of death are identified and addressed. In our study, overdose stigma in Centre-Sud versus fraud-induced social death in the West Island dictated the unique engagement trajectories required to achieve transformative outcomes.
Central to our findings is the emergence of “death sociability”—the formation of new social bonds through shared experiences of human finitude—as a key mechanism through which both the grassroots and institutionally-led models achieved these profound social and cultural transformations. The following discussion explores the nuances of this finding by interpreting the divergent community pathways, analyzing how both led to the creation of safe spaces, and connecting the concept of death sociability to broader public health palliative care principles.
Addressing diverse needs and population through context-sensitive approaches
Our findings demonstrate that the primary work of both compassionate communities was to identify and respond to the specific social determinants of death that manifested in their local contexts. Reflecting its community-led approach, Centre-Sud targeted the unmet palliative care needs of vulnerable populations, such as socially isolated seniors and people who use drugs in a context of overdose and loneliness epidemics. 28 This focus echoes concerns from a commentary by Higgs et al., 29 published in the context of Australian palliative care reforms, where they highlighted the unmet needs of the underserved populations. Conversely, the West Island addressed needs pertinent to its context, such as supporting seniors and caregivers, and brought to light the profound social and emotional needs arising from non-illness-related loss.
The outcomes of these initiatives align with the five public health palliative care principles (realistic utopia), 2 which provide a framework for the transformations needed to address these social determinants of death: (1) reducing social inequalities; (2) viewing death as a social and relational process; (3) building support networks; (4) breaking the death taboo; and (5) recognizing the value of death in the life cycle. The “Overdose Loss and Grief Café” in Centre-Sud and the “SAFE” peer support program in the West Island serve as powerful examples of how these principles are put into practice to address diverse forms of stigmatized loss.
Reducing social inequalities (Principle 1)
Both initiatives worked to reduce social inequalities by directly confronting specific social determinants of death: the social conditions that shape how people grieve and die, with a particular focus on vulnerable populations. The Overdose Café challenged the stigma surrounding drug use by validating overdose grief support as a legitimate harm reduction practice. This implicitly acknowledges the palliative dimensions of addiction and the stigmatized grief following overdose deaths. It aligns with research by Stajduhar et al., 30 which demonstrates that harm reduction principles, such as non-judgmental support and meeting people “where they are,” are intrinsically aligned with a palliative approach to care for structurally vulnerable populations. Similarly, the SAFE initiative empowered senior fraud victims by engaging them in the co-design of the peer support structure itself, a process that fostered social participation while directly addressing the profound shame and isolation associated with their loss. This successful model was ultimately scaled across the City of Montréal.
Creating safe spaces for support networks (Principles 2, 3, and 4)
A compelling commonality was the direct response to social determinants of death like stigma, shame, and isolation, which manifested as a fundamental need for safe spaces to process loss. Both programs created environments where difficult experiences could be shared, thereby normalizing these discussions and breaking taboos (Principle 4). In the SAFE program, participants shared stories of loss (financial, trust, social), overcoming isolation in a supportive peer environment. The Overdose Café provided a similar space for those affected by overdose loss to process their specific stigmatized grief. Beyond these therapeutic environments, the initiative also established proactive safe spaces. Extending “safe spaces” to schools provided a structured environment for youth to confront loss, fostering social participation and early death literacy. This complements the Compassionate Workplaces program, which created similar protections for working adults. Ultimately, anchoring these distinct safe spaces in schools, workplaces, and senior dwellings reframed loss as a broad social and relational process (Principle 2) and established a continuum of support networks accessible across the entire citizen lifespan (Principle 3).
Finding value and meaning through collective action (Principle 5)
Finally, both programs enabled participants to find value and meaning by transforming their personal experiences of loss into collective action. The seniors participating in the SAFE initiative were empowered by co-designing a prevention model to protect their peers from future harm. Likewise, the Overdose Café became a platform for honoring those who were lost and advocating for policy changes, giving a purpose to their grief. Our finding that value and meaning emerged from tangible, co-designed initiatives like the SAFE program and the Overdose Café is significant. This suggests that the “realistic utopia” principles are best achieved not through abstract discussion, but through concrete actions that address immediate, lived experiences of serious illness, end-of-life, loss, and grief. This aligns with the challenges observed by Quintiens, 10 where an initial focus on long-term “cultural change” frustrated stakeholders. Our study therefore suggests that for compassionate communities to succeed, finding value in death must be an emergent property of the new social connections and shared meanings that are forged through collective action, rather than a predefined theoretical goal.
These examples demonstrate that regardless of the specific trigger, be it overdose or fraud, context-sensitive compassionate community approaches can effectively support marginalized forms of suffering and achieve significant outcomes aligned with public health palliative care goals.
Social changes and cultural transformations in compassionate community
Beyond specific program implementation, our comparative ethnography revealed significant social and cultural changes within both communities, including increased death literacy, the creation of safe spaces for discussing mortality, and the development of compassionate cultures within and beyond partner organizations. A key outcome was the creation of a vital social space that normalized discussions around death and loss, directly confronting the prevailing taboo within participants’ environments.
This finding engages directly with the longstanding sociological debate regarding the “death taboo.” While scholars like Lofland 31 and Walter 32 have rightly questioned whether death is truly taboo or merely sequestered, our data suggest that for community workers in Centre-Sud, the distinction is semantic rather than experiential. For these participants, the silence surrounding mortality was not a theoretical abstraction but a tangible, structural barrier to coping. In their professional environments, the absence of dedicated spaces to process frequent encounters with death—whether through overdose, suicide, or the discovery of bodies days after death—left workers isolated in their grief. As Laurence, a harm reduction worker, powerfully articulated, this lack of social recognition for their impactful encounters with death directly contributed to burnout. This echoes findings from another Canadian compassionate community study who observed that inner-city workers frequently perform unrecognized palliative care “under the radar,” carrying a heavy burden of “vicarious trauma” and grief without adequate organizational support. 30 This reality resonates with Lofland’s, 31 argument that modern society suffers less from death denial than from a lack of a “craft of dying”, a set of scripted roles and rituals for navigating mortality. In pre-modern times, rituals dictated behavior. Today, individuals must improvise, resulting in a silence that reflects the mismatch between private loss and a lack of collective social scripts. This state of anomie, or social deregulation, leaves individuals to navigate grief in the absence of a shared “craft of dying.”
Consequently, our interpretation is that this “death taboo,” experienced here as structural silence and a lack of support, became the primary catalyst for engagement. Participants did not join the compassionate community to discuss abstract concepts, but to co-create the safe spaces their professional environments denied them. In doing so, these Compassionate Communities are essentially constructing the new “craft of dying” that Lofland identified as missing. They are building new rituals (e.g., the pebble tree, the candlelight vigil) and norms (e.g., safe spaces, death literacy) to replace silence with solidarity. These localized ethnographic observations resonate with broader evidence from other contexts, such as a UK Compassionate City, 33 a Belgian Compassionate University, 34 and Cities,10,25 where similar efforts were documented despite a more institutionally-led orientation. By creating spaces where death and grief are normalized, these initiatives do more than empower individuals, they strengthen community bonds and create the necessary conditions for a new form of social connection—death sociability—to emerge.
Transforming communities: The emergence of “death sociability”
As identified in our study protocol, 8 a priority gap in compassionate community research remains the measurement of social and cultural outcomes. A recent scoping review on public health palliative care interventions confirms that current metrics, which prioritize health indicators, often miss the mark. 35 Our comparative ethnographic findings address this gap by identifying “death sociability” as a concrete, observable mechanism of social transformation. This finding confirms that the “soft” mechanism of sociability can potentially yield “hard” public health outcomes. In our study, this process of building connections through shared experiences of mortality was a key driver of engagement, 12 catalyzing the development of compassionate cultures across participating organizations.
Central to this transformation was the creation of vital safe spaces that actively mitigated social determinants of death such as stigma, silence and shame by normalizing discussions around loss and confronting the prevailing taboo as reported by participants. To conceptualize these emergent dynamics, we introduce the term “death sociability.” We define this concept as the formation of new social bonds grounded in a shared recognition of human finitude. While often triggered by physical death (illness, dying, bereavement), our findings show it also emerges from experiences related to “social death,”36,37 manifesting as the loss of social connectedness and the radical “separation” from the community caused by stigmatized losses (e.g., addiction, fraud, homelessness).
Beyond the experience of social death reported by participants, emerging evidence confirms that fraud victimization is linked to severe psychological distress and an elevated risk of suicide, particularly among seniors living alone. 38 The resulting shame and isolation mirror the social determinants of death, demonstrating that addressing such “social” mortalities is as critical as addressing biological ones. In both cases, the “sociability” arises when safe spaces allow individuals to openly share these stigmatized narratives, reversing the dynamic of social invisibility and silence to transform the intimate experience of grief into social connection.
Death sociability counteracts what sociologists like Elias 39 and Lafontaine 40 described as the postmodern erosion of social ties in the experience of dying and grieving. Our findings are aligned with recent research on a Belgian compassionate university, which similarly observed the emergence of new informal networks around serious illness and bereavement. 34 This dynamic of reciprocity mirrors findings from the Compassionate Connectors in Australia 41 and Nav-CARE in Canada, 24 where volunteers described a “meaningful contribution” and felt the “reward is greater than the effort,” confirming that the benefits of engagement are bidirectional. This highlights that death sociability is defined by reciprocity rather than one-way service delivery, generating mutual value that reduces isolation for both the giver and the receiver. Furthermore, the tangible impact of these social bonds is supported by the evaluation of the Australian program, which demonstrated that such community-led connectivity interventions significantly reduced social isolation and lowered unexpected hospitalizations. 42
Indeed, our ethnography demonstrates that death sociability is cultivated through tangible, needs-driven activities. This dynamic illustrates how death sociability functions as a mechanism for what Leonard et al. 43 term “Experiential Learning,” the dimension of death literacy that is most strongly predictive of an individual’s capacity to navigate end-of-life care. By transforming private grief into a collective resource, these safe spaces address the critical gap identified by Van Dinther et al., 44 who found that unpaid carers often lack “Death System Literacy” and feel isolated despite their caregiving skills. Death sociability thus acts as a bridge, allowing individuals to build this crucial literacy collectively before a crisis hits, rather than in isolation.
Therefore, the potential for transformation lies in identifying local needs, co-designing solutions, and building momentum so that initiatives can ripple out from the micro to the macro level. Bronfenbrenner’s social-ecological model 45 provides a useful framework for conceptualizing this process, explaining how such transformations are interconnected across individual (micro), community (meso), and societal (macro) levels. The first Citizen Forum in Centre-Sud clearly illustrates this mechanism, where a guest speaker’s vulnerable story about his step-daughter’s suicide prompted others to share their own experiences of traumatic loss. This dynamic was further refined in initiatives like the Overdose Loss and Grief Café, where joining bereaved parents with people who use drugs, combined with collective rituals, created a powerful space to overcome stigma and find meaning. Similarly, the SAFE initiative brought senior fraud victims together with police and the research team; the very process of co-designing a prevention model created a safe space for them to overcome shame and reframe their experience as a prevention tool to prevent future harm. As a concept, death sociability holds significant potential for tracking these transformations, mirroring how Death Cafés create “peg communities” that help strangers connect and cope with dislocation. 46
The emergence of “death sociability” in these dedicated spaces empowers communities to actively reframe loss and advocate for change. Beyond immediate comfort, it actively builds various forms of cultural capital, which Bourdieu conceptualizes in three forms: embodied, objectified, and institutionalized. 47 Embodied cultural capital is evident as individuals acquire new language and skills for addressing mortality. The creation of community rituals, shared narratives, and physical safe spaces represents objectified cultural capital, providing the tangible tools and social norms necessary to reconstruct the “craft of dying” that Lofland identified as missing. 31 Finally, institutionalized cultural capital emerges through the formal recognition of these initiatives and their community practices (the West Island as a palliative care institution, and Centre-Sud as a non-profit organization). This accumulation of specific cultural capital signifies a durable transformation, equipping the community with the valued knowledge, shared meanings, and recognized structures needed to sustain its compassionate ethos and practices over time.
Implications for practice and policies
Our findings translate into a concrete roadmap for action, identifying four essential practice strategies and a critical requirement for policy innovation. Practitioners and community developers should focus on: (1) intentionally creating safe spaces for sharing diverse experiences of serious illness, end-of-life, and loss; (2) employing context-sensitive models like peer support that go beyond typical end-of-life narratives (e.g., cancer); (3) actively supporting vulnerable groups by recognizing how their unique social determinants of death create specific palliative care needs; and (4) fostering death sociability through facilitated experience sharing sessions that mobilize collective action. However, sustaining these efforts requires confronting a systemic barrier prevalent across the social and community sectors: the dominance of performative accountability. Currently, rigid funding regimes force organizations to prioritize administrative compliance over responsive community support, a dynamic that disproportionately deprives the most vulnerable. We urgently call on policymakers to shift from restrictive annual cycles to trust-based, multi-year funding focused on collective impact. By dismantling the administrative burden of constant auditing, the state can empower the social sector to redirect resources from bureaucratic maintenance to direct community support, ensuring that public funds actually reach those they are intended to serve.
Implications for research
Methodologically, this study underscores the value of longitudinal ethnographic methods to capture the influence of local context and identify socio-cultural transformations often missed by quantitative metrics. Analytically, our micro- and meso-level findings provide a crucial foundation for developing frameworks to measure broader, macro-level shifts in societal attitudes toward death. Future research should build on this work by exploring long-term impacts, the dynamics of these initiatives within diverse populations, and low-resource contexts, the role of digital compassionate communities, and the factors influencing scalability and sustainability.
Conceptual contribution: Death sociability as a theoretical lens
Conceptually, this study contributes to death sociability as an empirically grounded theoretical lens for future Public Health Palliative Care research. This concept offers a valuable framework for tracking the social changes (e.g., the creation of safe spaces) that enhance social capital and the cultural transformations (e.g., the development of compassionate cultures) to build cultural capital. For example, the emergence of “death sociability” can serve as a foundational indicator of transformation that is applicable across diverse contexts, allowing subsequent research to develop tailored impact measurements. A first step would be to map the emergence of safe spaces themselves within a community over time, using them as the primary unit of analysis to track transformation. Subsequently, once a critical mass of these spaces exists within a community and across sectors, a second stage of analysis could map the network of connections that forms between them. Such a meso-level analysis would reveal the emergent, community-wide support structure, moving beyond a traditional focus on individual relations. Future research can utilize this concept to analyze the mechanisms of social and cultural change initiated by compassionate communities and other similar initiatives.
Critical perspectives: Risks and limitations
While the creation of safe spaces and the emergence of death sociability offer significant benefits, a critical analysis reveals potential risks. The reliance on community organizations volunteers to address profound social deficits raises important questions about sustainability and the potential for health systems to offload their responsibilities onto unpaid citizens and underfunded community organizations. There is a risk that compassionate communities could become “enclaved,” serving primarily those who already possess the social capital to engage, while inadvertently excluding the most marginalized. Furthermore, the institutionalization of these initiatives, as seen in the West Island, must be carefully managed to ensure that the grassroots ethos is not co-opted by bureaucratic imperatives. Future research must vigilantly examine these power dynamics to ensure that the “realistic utopia” of community empowerment does not obscure the structural inequalities that necessitate it.
Limitations
Several factors should be considered when interpreting our findings. First, as with any comparative ethnography, this study’s deep, contextualized insights are not intended to be generalizable; their transferability to other settings should be carefully considered. The research also unfolded during the COVID-19 pandemic, which undeniably shaped participant engagement and development trajectories. Furthermore, as outlined in our protocol, 8 the ethnographic focus on collective dynamics means this study cannot offer standard evaluations or precise numbers of participants for each of the eleven compassionate programs.
A key challenge in evaluating such initiatives lies in the tension between the pressure for short-term, measurable impacts and the reality that genuine co-creation takes time to mature.6–8 This is also a well-documented issue in evaluating community engagement in public health. 48 While our philanthropic funding provided the crucial space to develop partnerships without the pressure for immediate results, the 5-year timeframe still captures only the beginning of these long-term transformations, a tension also observed in other complex intervention studies. 49
Finally, while the use of AI as a supplementary tool enhanced the analysis, we recognize its inherent limitations. The risk of the AI missing nuances or generating misinterpretations was proactively minimized, as it was only used on preliminary findings already generated by the first author. To ensure robust human oversight, the first author critically reviewed all AI-generated outputs against the original data, and the consolidated findings were presented to the action-research team and community partners for member validation before any final analytical decisions were made.
Conclusion
Building on our previous findings that successful compassionate community development depends on aligning the engagement strategy with local socio-cultural realities, 12 this article explored the transformative outcomes that resulted from such context-sensitive work. We conclude that positive social and cultural changes emerged both through grassroots, community-led empowerment that challenged professional boundaries (Centre-Sud), and via strategic institutionally-led adaptation, where an established palliative care organization embraced community expertise (West Island). The success of both pathways hinged on their ability to identify and respond to the specific social determinants of death prevalent in their local contexts.
A key unifying element was the emergence of death sociability within the safe spaces cultivated in both settings. This core conceptual contribution highlights the mechanism through which the principles of public health palliative care were realized. The open sharing of experiences around serious illness, end-of-life, loss and grief fostered vital social bonds, reframed dying as a social and relational process, and broke the death taboo in multiple settings. As an empirically grounded concept, death sociability offers a novel lens for understanding how shared vulnerability can catalyze connection, mutual support, and meaning-making across diverse populations and sectors.
Ultimately, this study underscores the transformative potential of compassionate community initiatives to address social inequities in how we live, die, and grieve. We have demonstrated that profound shifts—moving beyond medicalized views toward social understandings of death and fostering collective responsibility—can be achieved through different, yet equally effective means. For the future, recognizing how communities develop compassionate cultures, supporting the creation of safe spaces where “death sociability” can thrive, and bridging these local actions with supportive policy environments will be crucial for advancing a more equitable and human-centered approach to our collective experiences of death, dying, and grief.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524261434628 – Supplemental material for Taboo, safe spaces, and death sociability: A comparative ethnography of two compassionate communities
Supplemental material, sj-docx-1-pcr-10.1177_26323524261434628 for Taboo, safe spaces, and death sociability: A comparative ethnography of two compassionate communities by Émilie Lessard, Isabelle Marcoux, Serge Daneault, Lise Jean, Cynthia Lapointe, Dale Weil, Ghislaine Rouly, Libby Sallnow, Allan Kellehear and Antoine Boivin in Palliative Care and Social Practice
Footnotes
Acknowledgements
We extend our gratitude to Anitra Bostock, Émilie Warren, Janie Houle, Pierre Pluye, Robin Cohen, and Véronique Dubé for their contributions to the initial stages of the project. We also acknowledge the steering committee members of Communauté Compatissante Montréal (Centre-Sud) and the members of the West Island’s Community Seniors Table. Their invaluable contribution to this project is a reflection of the daily work done by community workers everywhere to improve the living conditions and well-being of their fellow human beings.
Ethical considerations
This study is approved by the research ethics board of the Centre hospitalier de l’Université de Montréal (approval certificate #18.353).
Consent to participate
Based on the ethical principle of minimal risk, we used a combination of implicit and explicit consent. Implicit verbal consent was used for observation of community activities, with participants able to refuse or remove sensitive information as they wish (no objections were raised). Explicit written consent was obtained for each participant interviewed through a standard informed consent form.
Consent for publication
Written informed consent for the publication of anonymized data was obtained from all individual participants included in the study.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project is funded by the Fondation J-L Levesque; A.B. is supported by the Canada Research Chairs program [grant number CRC-2020-00029].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
In accordance with ethical standards of the participants’ consent (approval certificate #18.353), the data that support the findings of this study are not openly available to protect confidentiality and participant’s identity. Data are located in a controlled access data storage at CRCHUM. Raw de-identified data may be made available upon reasonable request to the corresponding author*.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.