
Abstract
Background:
Person-centred care requires interdisciplinary collaboration. Within palliative medicine, collaboration is further necessary to meet the increasing global demand for palliative care. One area of developing collaboration involves Emergency Medical Services. However, there remains a dearth of research exploring patient and family member perspectives on Emergency Medical Services in palliative situations.
Objectives:
To explore perspectives of South African patients and family members with palliative needs concerning Emergency Medical Services use in their care.
Design:
A qualitative design using individual semi-structured interviews was employed.
Methods:
Patients and family members with palliative care needs who had previously experienced Emergency Medical Services care for these needs were included. Verbatim transcriptions of interviews were subjected to thematic analysis with an inductive-dominant approach.
Results:
Ten interviews were conducted. One overarching theme, The Dynamic of Control, and three categories were developed: (1) Loss of control: Heavy burdens of living with chronic and end-of-life illness, (2) Maintaining control: Longings and exigencies in times of suffering, (3) Transferring control: Consequential emergency medical services influence on palliative situations.
Conclusion:
Understanding the Dynamics of Control in palliative situations is fundamental to the Emergency Medical Services’ establishment of a person-centred approach in palliative situations. Practical developments that would allow this approach include alternative care pathways, on-scene information availability, and palliative care education. Including palliative care in Emergency Medical Services education may have benefits beyond improved palliative situation management, as it encourages a cultural shift towards person-centred care.
Background
Person-centred care is “an approach that consciously adopts the perspectives of individuals, families and communities, respects and responds to their needs, values, and preferences, and sees them as participants in their own healthcare rather than just beneficiaries.” 1 This aligns with palliative care, which implements this approach in life-limiting illnesses to improve patient and family quality of life. 2
Achieving person-centred care requires interdisciplinary collaboration and exploration of perspectives to understand specific needs.1,3–5 Within palliative medicine, collaboration is further necessary to meet the increasing global demand for palliative care, 6 particularly in low-to-middle-income countries (LMICs), which contain 80% of the demand.7,8 One area of developing collaboration involves Emergency Medical Services (EMS). 9 EMS frequently intersect with palliative situations and, thus, an opportunity exists to enhance the supply of person-centred palliative care through collective efforts.10,11 Despite this developing collaboration, there remains a dearth of research exploring patient and family member perspectives on EMS in palliative situations. 9 Current evidence demonstrates positive patient and family experiences; however, such studies are rare and limited to high-income countries.12–14 Within South Africa (SA), an LMIC, studies have explored the perspectives of EMS 15 and palliative providers 16 but patient and family perspectives remain unknown.
The World Health Organization’s Global Strategy on People-Centred and Integrated Health Services has stated that context-specific research is required to promote person-centred care, as no single, best-practice model exists. 17 Thus, to fill this knowledge gap within SA and contribute to the limited international literature, the aim of this study was to explore perspectives of SA patients and family members with palliative needs concerning EMS use in their care to the ultimate end of enhancing person-centred care. For the purposes of this study, ‘palliative situation’ refers to any event involving the care of a person with palliative needs.
Methods
Design
A qualitative design using semi-structured, individual interviews was implemented. Husserlian descriptive phenomenology, which describes the lived experience of participants, provided the theoretical framework. 18
Setting
SA healthcare, including EMS, is divided into private and state sectors. 19 State healthcare is provided to all citizens by the government. Private healthcare is restricted to those with medical insurance or other financial means. Out-of-hospital emergency care is paramedic-led. 15 Palliative care is largely delivered by non-governmental organisations, which rely on volunteers. 20 Although palliative care integration among medical disciplines is improving, equitable access to palliative care remains a primary challenge.
Data collection
The interview schedule was jointly developed by all authors based on current literature and previous work by Gage et al.9,15,16 The interview schedule (Supplemental File 1) contained four questions referencing demographics, reasons for EMS use, satisfaction, and confidence with EMS. To enhance in-depth exploration of perspectives and limit biases, pre-determined prompts and probes were included.
Participants were recruited through palliative care providers within the Association of Palliative Care Centres (national association of hospices with members from all SA provinces), 21 Association of Palliative Care Practitioners of South Africa (non-profit organisation comprising palliative care doctors), 22 and the University of Cape Town Division of Interdisciplinary Palliative Care and Medicine. 23 These palliative care providers identified patients and family members within their clinical practice who had made use of EMS in their care and provided these potential participants with an information and consent form. Interested patients and family members contacted C.G. directly or provided permission to the palliative care provider to be contacted. During the interviews, a summary of the information and consent form, and an opportunity for questions were provided. Verbal consent was provided by participants for both audio-recording and participation in the study.
Inclusion criteria were adult (⩾18 years old) patients with palliative needs residing in SA who had previously experienced EMS care, and family members of patients with palliative needs residing in SA who had previously experienced EMS care for the needs of their family. Exclusion criteria were patients and family members who experienced EMS care prior to developing palliative needs or who experienced EMS care outside of SA. Palliative needs were equated with those receiving palliative care at the time of EMS contact.
Interviews were performed telephonically at an agreed time. Telephonic interviews were selected as they represented the safest, least intrusive, and most widely available mode of communication, given participant health, vulnerability, and geographic distribution. 24 Interviews were performed by C.G., who is experienced in qualitative interviewing, and recorded using a cellular application. All recordings were manually transcribed verbatim by C.G. A pilot interview was not performed as the authors felt it was inappropriate, given the vulnerability of the population. Rather, the authors met to thoroughly deliberate upon the discussion schedule and interview techniques prior to data collection.
Ten interviews were held from September 2023 to March 2024 meeting recommendations for phenomenological studies. 25 No participants knew the interviewer previously, and all were aware that the study formed part of his post-graduate studies. No participants refused to participate or dropped out and no repeat interviews were conducted.
Analysis
In line with the approach of Husserlian descriptive phenomenology, inductive content analysis of the manifest data to the categorical level was originally performed. 18 However, after employing this approach, it became evident that further analysis at the latent, thematic level was required. Participants provided their perspectives through personal narratives, which contained rich, underlying meaning. Thus, thematic analysis of transcribed data was performed using the framework of Braun and Clarke with an inductive-dominant approach (Table 1). 26 As Olmos-Vega et al. 27 have discussed, qualitative research is “reactive to rich contexts” and, therefore, methodological considerations must appropriately adapt to findings within these contexts. Coding was performed using NVivo (version 14, Lumivero; Denver, Colorado, USA Figure 1). Data saturation, as detailed by Saunders et al., 28 was determined through familiarisation with the transcripts, noting repetitive comments, and a lack of additional data after the 10th interview.
Data coding procedure.

Coding tree.
Reflexivity
This study formed part of my (C.G.) post-graduate studies. During this study, I was employed as a programme coordinator at a state SA EMS college. I found the present interviews more challenging than in previous studies, as significantly more probing was required to gather in-depth answers. Furthermore, probing itself was, at times, difficult due to the emotional nature of the topics being recounted. Despite this, the discussion schedule seemed to function well, and participants appreciated the discussions. Throughout the research process, I recognised my own personal bias that SA EMS have a positive role to play in palliative situations. I attempted to limit the introduction of this bias in the interviews by refraining from asking leading questions, adhering to the discussion schedule, engaging in continuous reflexivity, and frequently debriefing with the research team. Despite my bias, some participants detailed negative experiences of EMS which challenged my assumptions and must be carefully considered.
Words cannot express my gratitude towards each participant for allowing me, a stranger, to delve into such personal moments. I trust this study will positively impact all others experiencing the heavy burdens of palliative needs.
Trustworthiness
To ensure trustworthiness, the framework of Guba was used in seeking credibility, transferability, dependability, and confirmability. 29 The following denotes methods by which these criteria were pursued:
Credibility: Interview technique was practiced and thoroughly deliberated upon. Participants were able to refuse participation. Frequent communication and debriefing sessions were held between the interviewer and the research team. Researcher triangulation was performed. Member checking, where each participant was sent a summary of the thematic analysis, was undertaken to check agreement. No subsequent changes were required as it was referred to as “accurate” and “resonating deeply.” A reflexive commentary has been included.
Transferability: A thorough description of data collection methods has been given, including the number and length of interviews, and the total time-period of data collection. Results have been compared with available literature. This study has been written according to the COnsolidated Criteria for Reporting Qualitative (COREQ) research checklist.
Dependability: Thorough descriptions of research design, implementation, and data-gathering, as well as a reflexive commentary, have been presented.
Confirmability: Preliminary hypotheses held by the research team that were not demonstrated in the data have been reflected upon. Researcher triangulation and member checking were performed. Verbatim transcriptions of audio-recordings were produced.
Results
Ten participants were interviewed (Table 2). Interviews lasted between 18 and 37 min. Three categories and one overarching theme were developed (Table 3).
Interviewer and participant details.
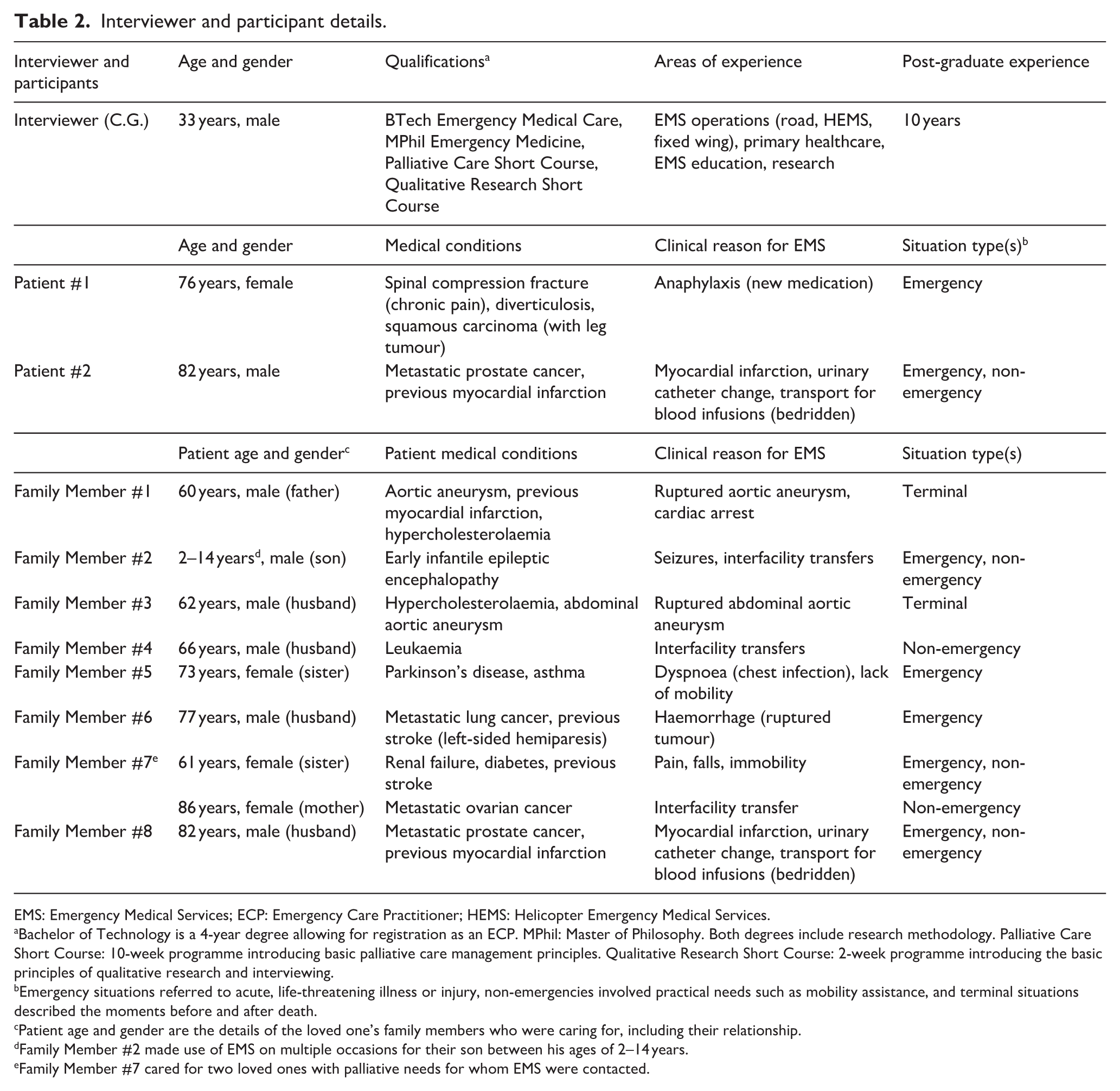
EMS: Emergency Medical Services; ECP: Emergency Care Practitioner; HEMS: Helicopter Emergency Medical Services.
Bachelor of Technology is a 4-year degree allowing for registration as an ECP. MPhil: Master of Philosophy. Both degrees include research methodology. Palliative Care Short Course: 10-week programme introducing basic palliative care management principles. Qualitative Research Short Course: 2-week programme introducing the basic principles of qualitative research and interviewing.
Emergency situations referred to acute, life-threatening illness or injury, non-emergencies involved practical needs such as mobility assistance, and terminal situations described the moments before and after death.
Patient age and gender are the details of the loved one’s family members who were caring for, including their relationship.
Family Member #2 made use of EMS on multiple occasions for their son between his ages of 2–14 years.
Family Member #7 cared for two loved ones with palliative needs for whom EMS were contacted.
Theme, categories, and subcategories developed from interviews.

EMS: Emergency Medical Services.
Discussion
Below, the theme and categories are discussed with supporting participant quotes. Participants are identified as patients or family members and by number (e.g. Patient/Family Member #1).
The dynamic of control
Participants described the heavy burdens of experiencing chronic and end-of-life illness, which resulted in a sense of lost control over their lives. This loss of control produced a desire in participants to maintain what control remained in their lives, as expressed through deeply experienced longings and exigencies in times of suffering. This desire for maintaining control directly affected participants’ perspectives of EMS use in their situations. As control was fluid, dynamically shifting within situations and among involved individuals, this overarching theme of control has been termed the Dynamic of Control.
The chronic illnesses experienced by participants imposed various constraints upon them, resulting in compelled decisions and a loss of much control they previously held over their lives as life began revolving around the illnesses.
I was a credit controller for the many years that I was working and then I stopped working as a result of my husband’s illness which was really hard. – Family Member #4
This loss of control produced a yearning in participants for control to be re-established and maintained. EMS were contacted for assistance when further situational control was lost (e.g. patient deterioration) for assistance in re-establishing this control. EMS care was viewed positively when this was achieved through transferring control back to participants, and negatively when EMS failed to re-establish situational control or seized further control from participants.
They [EMS] understood, they never questioned me. . .they were so kind. – Family Member #1 I was getting so frustrated because I was worried about my husband haemorrhaging . . . [EMS are] supposed to be coming in to save his life that’s already about half an hour into after I phoned them. And this [EMS provider couldn’t drive]. I was almost ready to jump in the ambulance and try and drive it [myself]. – Family Member #6
Understanding why patients and family members with palliative needs contact EMS is fundamentally important to establishing a person-centred approach in EMS and palliative care collaborations. Commonly documented reasons for EMS interactions with palliative situations are unexpected patient deterioration, caregiver exhaustion, and distressing symptoms.10,13,30,31 Other reasons in the present study included practical needs such as mobility, planned transport, and minor procedures. Our findings suggest the Dynamic of Control explains an underlying reason for contacting EMS. The needs for autonomy, homecare, and 24/7 availability of care are practical expressions of this dynamic, while clinical situations represent the contexts in which control must be regained. Autonomy is desired to avoid losing further control. Homecare and 24/7 care availability provide comfort in the setting of their choice and knowledge that, should control be lost, it may be regained rapidly at any time. Previous studies have highlighted the suitability of EMS to meet these needs.5,32–35 A Canadian study demonstrated increased confidence among those in palliative situations simply through knowledge of EMS 24/7 availability. 13 We suggest that a reason for this confidence was a sense of increased control over an unpredictable future.
The Dynamic of Control should also inform the tone of EMS interactions in palliative situations. “[Allow] the family to. . .set the tone. . .[Give] the family time to kind of indicate where they are at in their frame of mind” (Family Member #2). This requires a perspicacious approach from EMS providers as they must be receptive to the tone set by patients and families while simultaneously deciding where to take and cede control. Typically, EMS providers take complete control of chaotic emergency situations, which is often appropriate. However, this approach may be harmful in palliative situations. In the palliative setting, the tone should be one of deference to patients and families according to their needs, regaining control where necessary and transferring it back where possible, thereby viewing patients and family members as participants in their care. This person-centred approach runs contrary to the typical EMS mindset.15,36,37 Thus, EMS should be trained in the identification of and a differing approach to palliative situations. Any EMS and palliative care collaboration should aim at a deferential, person-centred tone to meet the unique needs of this population.
Loss of control: Heavy burdens of living with chronic and end-of-life illness
When questioned regarding their circumstances, participants detailed heavy burdens they live(d) with due to chronic and end-of-life illness, which resulted in a perceived loss of control of their lives. These burdens may be categorised as: (a) Dealing with death, dying, and suffering; (b) Difficult decisions concerning care; and (c) Necessitated lifestyle changes.
Dealing with death, dying, and suffering
Many participants recounted strong, negative emotions when faced with personal suffering or when witnessing the suffering and, in some cases, the death of a loved one. Feelings of loneliness, weariness, desperation, and pain were prominent.
It’s not easy to do this at home because it’s basically just you. . .and you’re watching them die. . .I had to call the ambulance, I was alone. . .there was nobody. – Family Member #6 So then unfortunately she got a stroke. . .and she was in a coma for three weeks. That was quite painful. . .And then it’s the pain of watching somebody slowly dying. – Family Member #7
Providing care for a dying loved one has been described as one of the most stressful human experiences. 38 Thus, caregiver exhaustion is a frequently cited reason for EMS assistance in palliative situations. 9 Caregiver pain is likewise involved, as witnessing a loved one suffer is itself painful. This relates to the palliative care concept of “Total Pain.”39,40 In this holistic view, pain is not a purely physical phenomenon but also psychological, social, and spiritual. While some patients in this study experienced excruciating physical pain, many family members experienced other aspects of pain.
SA EMS providers are trained principally in physical pain management through pharmacological means and have described difficulty in handling family members in palliative situations due to a lack of agreement concerning care. 15 Thus, EMS providers may see family members as interfering with their management, leading them to take complete situational control. This fails to recognise the family member suffering and denies their need for control. The concepts of “Total Pain,” inclusion of family members, and an understanding of the Dynamic of Control, therefore, are important for EMS providers in palliative situations.
Difficult decisions concerning care
Participants shared various challenging decisions imposed upon them involving the place of care, level of intervention, withholding, and withdrawing of care. In some instances, these decisions resulted in conflict, feelings of regret, and insecurity. For example, one participant decided against resuscitation during her father’s cardiac arrest and was left asking, “What did I do? What if he was ok?” (Family Member #1).
She was very upset about everything. . .didn’t want treatment. . .But I could not have left her there, not being able to breathe, I couldn’t do it. – Family Member #5 They put her on the ventilator and. . .next time I will not allow someone to go on the ventilator. . .But the moment when they phoned me to say she’s in a coma we need to do something you allow and say ok please look do whatever to save the person. – Family Member #7
Conflict between patients and family members in palliative situations is not uncommon.5,30,33 Deliberating upon life and death choices may be overwhelming for both patients and family members, adding to the burdens of these situations. Complete control over decision-making may be ceded to healthcare providers, displaying profound trust in them. This may be a relief to some, but contribute to a sense of helplessness for others. Identifying these differing situations requires insight from EMS providers to enact a deferential tone.
One suggested method of ameliorating these decision-making challenges has been advanced care planning.14,37,41 Advance care plans allow patients and family members to make crucial healthcare decisions for future eventualities prior to stressful moments of suffering, enhancing their sense of control. 42 Despite their potential benefit, advance care plans are not common in SA, and where they are in place, EMS providers often lack access to this information. 15 A recommended mechanism for information availability has been the development of a palliative care booklet that patients would have in their homes. 16 We recommend this booklet contain information regarding patient condition and treatment, care goals, desired place of care, advance care plans, and contact details of involved healthcare providers.
Necessitated lifestyle changes
Other burdens of living with chronic and end-of-life illness involved necessitated lifestyle changes. Changes were required concerning work, retirement, finances, and priorities. Furthermore, because of various illnesses, participants noted the necessity of continual healthcare use.
I’m divorced and remarried. My first marriage didn’t survive the trauma of [son’s] disability. So yeah, that was that was quite difficult. . .my dad has chosen to retire. . .and he pays half of [son’s] fees. . .This places a further financial burden upon him as he has had to take this into account and tailor his retirement due to this factor. – Family Member #2
While many lifestyle changes were negative, one participant, despite being bedridden, described his situation as the “happiest time of my life” as he was otherwise “blessed with good health” and maintained a happy marriage (Patient #2). This demonstrates the need for EMS providers to understand the dynamics of a given palliative situation to maintain a deferential tone. However, EMS providers, internationally and in SA, have expressed difficulties in approaching palliative situations due to EMS cultural and system constraints.15,37,43 EMS providers may be unable to allow those with palliative needs to set the tone with the current lack of support structures. A recent study allocated various methods of support at micro-, meso-, and macro-levels, including EMS provider palliative care training (micro), developing guidelines for palliative care provision (meso), and including EMS in national palliative care policies (macro). 41 We recommend these measures in the SA setting; however, a preparatory cultural shift among SA EMS will likely be necessary. 16
Maintaining control: Longings and exigencies in times of suffering
The heavy burdens experienced by participants resulted in deeply intuited longings and exigencies which were related to their underlying desire to maintain what control remained in their difficult situations: (a) Desire to be treated as human beings and (b) Readily accessible care.
Desire to be treated as persons
Participants longed for a person-centred approach from healthcare providers. For example, describing a positive experience, one participant said, “They’re [hospice staff] very kind and they took an interest in me as a person which I found really endearing” (Patient #1). The desire for this approach was also evidenced in participants’ positive reflections upon receiving compassionate care, being listened to, and involved in decision-making.
They [EMS] were very kind and caring . . . and made everyone feel very comfortable. – Family Member #5 But the way they [EMS] treated me . . . I can only speak of great patience from them. . .with real dignity and respect. – Family Member #3
Studies in Canada, 13 Australia, 14 and New Zealand 12 have demonstrated the desires of patients and families with palliative needs for person-centred care. These studies also demonstrated the desire of many with palliative needs to be cared for in their homes and avoid hospital conveyance. The same is true in SA. For example, a study in Soweto found home to be the preferred place of death in 67% (n = 126) of patients with advanced cancer. 44
To fulfil this desire, and so cede control to patients and family members through respect of autonomy, alternative care pathways for EMS require development. Participants in the present study reacted positively when alternative care pathways were used. EMS provided homecare without conveyance (Family Member #8), transported a patient to hospice (Family Member #4), and transported a patient home from hospice (Patient #2). Facilitating patient desires in this manner represents a practical means by which a person-centred approach may be achieved. Typically, EMS involvement results in hospital conveyance, particularly in LMICs, which frequently use EMS solely for transportation. 45 This was demonstrated in a large Western Cape (province of SA) study, which found that 98% (n = 240,730) of patients managed by EMS were transported to a hospital despite 83% (n = 199,062) of these not having received any EMS treatment. 46 In palliative situations, this is inappropriate as it imposes the EMS system upon patients and families rather than adjusting the system to meet their desires.
Readily accessible care
An important exigency identified by participants to maintain control in palliative situations was the availability of additional support as and when needed, particularly when their home treatment was insufficient. EMS fulfilled this requirement through 24/7 availability and rapid response times. This provided participants with an increased sense of control as, in the not unlikely event of losing situational control, for example through patient deterioration, control could be readily re-established through EMS at any time of day or night.
Very, very reassuring to know that we have an excellent, locally based paramedic service here which gives great peace of mind for me to know that if our doctor is not available, we immediately have the paramedics on call, and they are here literally within five minutes. – Family Member #8
Access to healthcare comprises several dimensions: (1) Availability: the balance of supply and demand, (2) Accessibility: the location of services in relation to clients including transport needs, (3) Accommodation: the way services facilitate clients, (4) Affordability: the cost of services relative to clients’ purchasing power, and (5) Acceptability: clients’ attitudes towards services. 47 From the current study, patients and family members have found EMS valuable regarding Accessibility (transport) and Accommodation (24/7 availability, homecare).
Transferring control: Consequential EMS influence on palliative situations
Given the heavy burdens resulting in a loss of participant control over their lives, and the resultant deeply felt desire to re-establish and maintain control, EMS involvement was significantly consequential, whether positive or negative. EMS, in many instances, gained situational control and transferred this back to participants, thereby (a) fulfilling the desires for compassion and reassurance, which resulted in (b) high regard for EMS. However, when EMS failed to transfer control, participants experienced (c) amplified needs resulting from poor EMS care.
Fulfilling the desires for compassion and reassurance
In most cases, EMS providers fulfilled participant desires for person-centred care through compassion and reassurance, which restored a sense of control over stressful circumstances. Participants described the dignity and empathy with which EMS providers treated them and the comfort, security, and confidence this provided. The fulfillment of these deeply experienced desires brought some participants to tears as they recounted “extraordinary” EMS care that “doesn’t get better” (Patient #1), demonstrating the significant impact EMS have in palliative situations.
. . . those [EMS providers] actually cried with me. They were absolutely amazing . . . Such empathy for people that they don’t know. Just, I mean, it touches you very deeply. – Family Member #4 . . . they just make you feel that . . . you’re in good hands . . . your stress level usually goes down upon their [EMS] arrival and then when they are so calming and competent and efficient and kind it just takes your stress level down you know. Still a highly stressful situation, but they just make it easier, in a big way. – Family Member #8
A further way in which EMS providers delivered person-centred care was through proactive assistance, which went beyond their required duties. For example, several participants mentioned EMS providers waiting at hospitals to assist in the admission process and provide updates on their loved one’s condition. Other studies have also noted the compassionate and proactive care EMS providers deliver in palliative situations.12,13 SA palliative providers have, likewise, expressed feelings of reassurance when EMS provide assistance. 16 Moreover, many EMS providers have found the provision of person-centred care fulfilling.48,49
High regard for EMS
As a result of these fulfilled needs, most participants held EMS in high regard, expressing gratitude, praise, and satisfaction. Further demonstrating the consequential nature of EMS care in palliative situations, one participant expressed lasting memories from her experience.
That actually brings tears to my eyes . . . I find it’s extraordinary that I’m still here thanks to [EMS provider]. This is very overwhelming for me to hear that you know [him]. – Patient #1 My experience I’ll never forget it . . . I remember it as yesterday the way they cared about me. – Family Member #3
Juhrmann et al. found that EMS had a revered public identity due to their ability to fix crises, which aligns with the views of participants in the present study. 14 SA palliative care providers also hold EMS in high regard. 16 Given this common positive view of EMS among patients, family members, and palliative care providers, it appears reasonable that EMS and palliative care collaboration is pursued in SA.
Amplified needs resulting from poor EMS care
While EMS were held in high regard overall, some participants experienced poor care from EMS, resulting in the deepening, rather than fulfilling, of their needs. These participants expressed frustration, disappointment, and increased stress when poor care was received.
I was actually horrified. I thought [husband] was going to bleed to death. And [EMS are] moaning about this and that . . . I was very disappointed. – Family Member #6
Poor EMS care was characterised by failure to gain situational control, thus precluding the re-establishment of patient and family control. In these situations, EMS providers failed to allow those under their care to set the tone. This was demonstrated in the case of Family Member #2, who recalled EMS providers approaching her son’s worrying seizure activity in a playful rather than professional manner.
But they came and they sort of they treated him and they you know tried to get him stable but there was quite a lot of. . .joking and bantering going on while they were trying to stabilize him. – Family Member #2
In the case of Family Member #6, EMS providers were unable (or unwilling) to access her home due to difficult terrain and the presence of dogs on the property: “They [were] too scared to do anything.” Because of these perceived EMS failures, participants experienced a sense of incredulity at the treatment they received. Both instances were highly stressful and out of their control, requiring trust in the EMS. Their expectation was for EMS to regain control and provide reassurance, however, they were left feeling “ambivalent” and “shocked” about these “bizarre,” “surreal” circumstances. In these cases, EMS worsened patient and family burdens through an inappropriate tone and betraying trust. This may be avoided through understanding the Dynamics of Control and the heavy burdens which patients and families carry.
It has been previously hypothesised that EMS palliative care education would develop more well-rounded EMS providers, not only improving their palliative situation management, but also their management in general. 16 We suggest this development would occur by stimulating the needed cultural shift within EMS towards a person-centred approach, which palliative care espouses. 2 Person-centred approaches are valuable in all healthcare situations and are associated with high-performing systems, improved outcomes, increased provider satisfaction, and financial strength.50,51
The current SA EMS approach may be described as system-centred, imposing itself upon patients in a “one-size-fits-all” manner. For example, EMS systems frequently implement hospital conveyance regardless of context, case severity, or patient wishes.16,46 In palliative situations, this approach often leads to conflict with patients and families, worsening their situations. This system-centred approach denies the heavy burdens patients and families suffer, fails to enact a deferential tone, and seizes control where it should be transferred. Other negative consequences include increased strain on already overfull hospitals with limited resources and amplified healthcare system costs. 11 Thus, we strongly recommend palliative care education for EMS, not only for improvement in palliative situations, but as a catalyst for EMS cultural change, thereby benefiting patients, family members, EMS providers, and healthcare systems in their entirety.
Limitations
The sampling strategy employed resulted in a relatively homogenous participant demographic, making use of, primarily, private EMS. Self-selection bias cannot be excluded as participation was voluntary. However, participants were broadly distributed across SA, experiencing a range of palliative situations, resulting in various perspectives which were discussed in view of similar studies in differing contexts. While the transferability of specific participant emotions and needs may be limited, the general principles drawn (e.g. deferential tone) remain vital. Telephonic interviews limit interactions with participants by prohibiting the use of non-verbal cues, which may create difficulty in establishing rapport, thereby limiting the depth of answers provided by participants. Despite these potential concerns, telephonic interviews remained the safest way to approach this population, and no difficulties were experienced in establishing rapport, resulting in open conversations for which participants expressed appreciation. Although the discussion schedule was not pilot tested, steps were taken to ensure its credibility and dependability. The rationale for this approach has been clearly explained to support dependability. To ensure credibility, the discussion schedule was informed by prior qualitative interviews on this topic15,16 and developed collaboratively by an experienced qualitative research team. Ongoing debriefing sessions and positive feedback through member checking confirmed the discussion schedule’s appropriateness and effectiveness.
Conclusion
The aim of this study was to gather perspectives of SA patients and family members with palliative needs concerning EMS use in their care. One overarching theme, the Dynamic of Control, and three categories were developed: (1) Loss of control: Heavy burdens of living with chronic and end-of-life illness, (2) Maintaining control: Longings and exigencies in times of suffering, (3) Transferring control: Consequential EMS influence on palliative situations. Participants described a loss of control over their lives and a subsequent longing to maintain what control remained. EMS care was viewed positively when this longing was satisfied and negatively when further control was seized. Understanding this Dynamic of Control is fundamental to the EMS establishment of a person-centred, deferential tone in palliative situations. Including palliative care in EMS education may have far-reaching benefits beyond improved palliative situation management, as it challenges the current system-centred approach and encourages a cultural shift towards person-centred care.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251409346 – Supplemental material for The dynamic of control: A qualitative analysis of the perspectives of patients and family members with palliative care needs on Emergency Medical Services
Supplemental material, sj-docx-1-pcr-10.1177_26323524251409346 for The dynamic of control: A qualitative analysis of the perspectives of patients and family members with palliative care needs on Emergency Medical Services by Caleb Hanson Gage, Liz Gwyther and Willem Stassen in Palliative Care and Social Practice
Footnotes
Acknowledgements
The authors would like to acknowledge and sincerely thank each participant for their invaluable input into this study. We also thank Dr. Julia Ambler, Dr. Shannon Odell, Dr. René Krause, Dr. Katya Evans, Dr. Jennie Morgan, Dr. Danielle Lincoln, Sr. Kerene Payne, and Sr. Francois De Marcy Pugin for their assistance in participant recruitment.
Ethical considerations
This study was performed in accordance with the Declaration of Helsinki and ethical approval was provided by the University of Cape Town’s Human Research Ethics Committee (HREC Reference Number: 221/2023) on 4 April 2023.
Consent to participate
All participants provided verbal consent to participate in the study.
Consent for publication
Informed consent for publication was provided by participants.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analysed in this study may be made available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.