
Abstract
Background:
Community volunteers in palliative care (PC) have a unique position between healthcare professionals, community residents with care needs, and informal caregivers, offering complementary care and potentially playing a key signposting role. However, they need specific support in recognizing, describing, and communicating patient needs effectively, which can be transferred through training. The specific knowledge and skills required to take on this signposting role remain unclear.
Aims:
To explore (1) experiences of communication and information sharing between community volunteers and healthcare professionals and (2) the desired and required knowledge and skills volunteers need to recognize, describe, and communicate PC needs to healthcare professionals.
Methods:
A qualitative study design was used, conducting focus groups with community volunteers and healthcare professionals, and individual semi-structured interviews with community residents with PC needs and informal caregivers. Inductive thematic analysis was applied.
Results:
Seven focus groups with 15 community volunteers and 20 healthcare professionals, and 10 interviews with 6 community residents with care needs and 4 informal caregivers were conducted. Findings revealed limited contact between volunteers and professionals and a lack of mutual awareness of each other’s involvement, with professionals often distrusting volunteers as communication and collaboration partners. Perceived hierarchy made volunteers hesitant to communicate with professionals. Communication was typically one-directional, with volunteers sharing patient information. There were no established procedures for communication and information sharing. To fulfill their signposting role, volunteers need knowledge of PC needs and community resources, and strong relational, communication, and observation skills.
Conclusion:
Volunteers need extensive skills to take on their signposting role. Training programs could boost volunteers’ self-confidence by (1) increasing awareness and understanding of the community volunteer role and signposting function; (2) enhancing knowledge of PC, PC needs, and community services; (3) strengthening communication with resident’s care needs, informal caregivers, and healthcare professionals. For the sake of patient care, it is important to improve communication, relationships, and collaboration between volunteers and professionals.
Keywords
Introduction
Palliative care often reaches patients too late, leaving psychological (e.g., low mood, loss of meaning, and loss of hope) and social needs (e.g., participation in daily life, loneliness, and financial stability) unmet.1,2 From that need, community volunteers in palliative care (PC) occupy a unique position between healthcare professionals, community residents with palliative care needs, and informal caregivers. They offer care that is complementary to that provided by professionals, potentially playing an important signposting role for people with PC needs (i.e., identifying and helping to communicate their care needs and wishes to healthcare professionals). 3 Community volunteers can observe and communicate patient needs that may be overlooked by other caregivers1 –8, such as the needs and wishes of the dying person, ranging from simple preferences and concerns to anxiety, pain, discomfort, and even problems in their households. Community volunteers may require particular support in terms of knowledge and skills to recognize and describe patient needs and wishes and communicate them effectively to healthcare professionals. Such skills may be transferred through training. However, there is currently no literature on what particular knowledge and skills can best support them to optimally fulfill a signposting role.
While the primary responsibility for palliative care rests with healthcare professionals and family carers, community volunteers often play an important complementary role within this context.9,10 A substantial number of individuals receiving palliative care prefer or need to stay at home and many do not have an informal caregiver. 11 An important role can thus be played by volunteers in supporting and caring for patients in a home setting. Previous research identifies various volunteer roles in palliative care. One prominently described role, which focuses on presence, is often described as “being there” 3 or “being with” 12 and facilitates relationship building. Vanderstichelen et al., 3 described this role as offering psychological, social, and existential support to the seriously ill or dying person, focusing on nurturing relationships and addressing nonmedical needs.3,10,12 –15 This approach, combined with frequent close contact with patients, allowed volunteers to form a different kind of personal relationship with patients compared to healthcare professionals. 3 Similarly, Dodd et al. reported that such close contact and meaningful conversations enabled volunteers to connect with patients on a personal level, fostering relationship building, trust and open communication. Another role aligns more with activity-based support, referred to as “liaison” 3 or “doing for.” 12 Volunteers in this role act as a bridge between community residents with care needs, their community, and social and healthcare services, through which they notice and communicate patient needs missed by other caregivers.3,4 Social activities undertaken by volunteers can help (re)open a patient’s world, allowing them to experience a sense of normalcy and engage in daily social life more actively than before.3,12
Volunteers are not just active in specialist palliative care services, they are also well integrated in generalist palliative care settings (e.g., nursing homes, homecare nursing services, and home visiting services). 16 Among the latter, many volunteers are active as community volunteers, visiting people with care needs living at home. Such community volunteers can play an important role in contributing to the well-being and comfort of community residents and their loved ones by offering companionship, combating loneliness, and alleviating the burden on informal and professional caregivers. 17 Given these roles and the time they spend with community residents, community volunteers are well-positioned to observe and identify patient needs and wishes that healthcare professionals may sometimes miss.2,4,5,8,18
Community volunteers can relay these needs and wishes to informal caregivers and healthcare providers, ensuring that the community resident’s preferences, needs, and concerns are effectively addressed. 18 Collaboration and information sharing are strongest in settings where volunteers work directly alongside nurses. 18 However, studies show that in community homecare settings, direct contact between community volunteers and healthcare professionals can be infrequent, sporadic, or nonexistent. 18 Despite the crucial role of community volunteers to collaborate with healthcare professionals, communication, information exchange, and collaboration between community volunteers and healthcare professionals are not common or taken for granted.
In addition, studies find that volunteers in community homecare settings receive little support regarding basic palliative care knowledge and communication with healthcare professionals.5,8,18 This indicates a gap between volunteer practice and support for volunteers in community-based homecare, and a potential for higher quality and more efficient signposting of palliative care needs by these volunteers. However, there is insufficient insight into the specific knowledge and skills that community volunteers need to recognize, accurately describe, and appropriately communicate patient needs and wishes to healthcare professionals. Closing this gap could result in a more efficient identification and signposting of palliative care needs by these volunteers, more timely addressing of palliative care needs among community residents, potentially faster referrals of residents with palliative care needs, and therefore higher quality care and support for people with palliative care needs living at home.
To close this gap, it is necessary to determine where the support needs of volunteers in their signposting role lie – in terms of knowledge, skills, and empowerment – and how volunteers can be supported to maximize their potential and to feel empowered to provide support and effectively communicate care needs to healthcare professionals where needed. It is necessary to explore how volunteers interact and collaborate with healthcare professionals, community residents, and informal caregivers.
Therefore, we aim to explore (1) experiences of communication and information sharing between community volunteers and healthcare professionals and (2) the desired and required knowledge and skills for volunteers to recognize, describe, and communicate palliative care needs to healthcare professionals. Our research questions are:
(1) How do community volunteers communicate and signpost information to healthcare professionals?
(2) What do community volunteers need in terms of knowledge and skills to recognize, describe, and communicate palliative care needs?
Methods
Context
This paper is part of a broader research project that aims to develop, implement, and evaluate a training program that supports community volunteers in their signposting role. This project follows the Intervention Mapping Protocol, an intervention development approach aimed at creating behavioral change (Figure 1). 19

Different steps of the IMP. 19
The current paper covers step 1: problem statement and step 2: program outcomes and objectives, in the development of the intended training program. Step 1 is focused on determining the need for knowledge and skills of community volunteers in fulfilling a signposting role for community residents with palliative care needs, and step 2 is about translating these needs into potential training program outcomes and objectives. 19
Design
We applied a qualitative research design, conducting focus groups with community volunteers and healthcare professionals, and individual semi-structured interviews with individuals with palliative care needs and informal caregivers. Focus groups were chosen because they stimulate the exchange of views and opinions through discussion and allow mutual differences or similarities to drive the conversation and salient themes to emerge. 20 Considering the fragile health of individuals with palliative care needs and the personal and potentially sensitive nature of the topic, individual interviews were considered a more suitable method of information gathering for residents with care needs and informal caregivers as they respect their individual experiences. The use of semi-structured interviews makes it possible to treat these cases discretely and allows participants to speak freely. This article follows the Consolidated criteria for reporting qualitative research (COREQ) guidelines for reporting qualitative research. 21 Supplemental Appendix I shows the application of the checklist to this study.
Setting
Samana is a nonprofit association that operates in Flanders (the northern part of Belgium). This organization is committed to supporting community residents with chronic diseases in need of care and their informal caregivers. 22 The organization operates independently of professional services and, with the help of more than 25,000 volunteers, facilitates a range of activities across multiple domains, including community work, holiday programs, training initiatives, buddy programs, and informal caregiver support. 22 In the domain of community work, groups of volunteers, active in over 1100 local communities, conduct home visits and organize gatherings for individuals with chronic illnesses, those in need of care, and informal caregivers within their neighborhoods. 22 Local departments of Samana strive for a good match between the volunteers and the local residents with chronic and/or palliative care needs.
Participants and sample selection
Our participants initially included (1) community volunteers who visit people with chronic illness and palliative care needs at home in their community (referred to as volunteers throughout the rest of this paper), (2) healthcare professionals, and (3) people with palliative care needs living at home (referred to as community residents throughout the rest of this paper). Due to COVID-19 restrictions and resulting difficulties in recruiting people with palliative care needs, (4) informal caregivers were added to our target population to get additional perspectives on the involvement and contribution of volunteers in their homes and care. Targeted healthcare professionals included general practitioners, psychologists, nurses, social workers, and moral counselors (who provide support addressing moral and existential questions). Table 1 provides an overview of the inclusion criteria.
Sample and inclusion criteria.
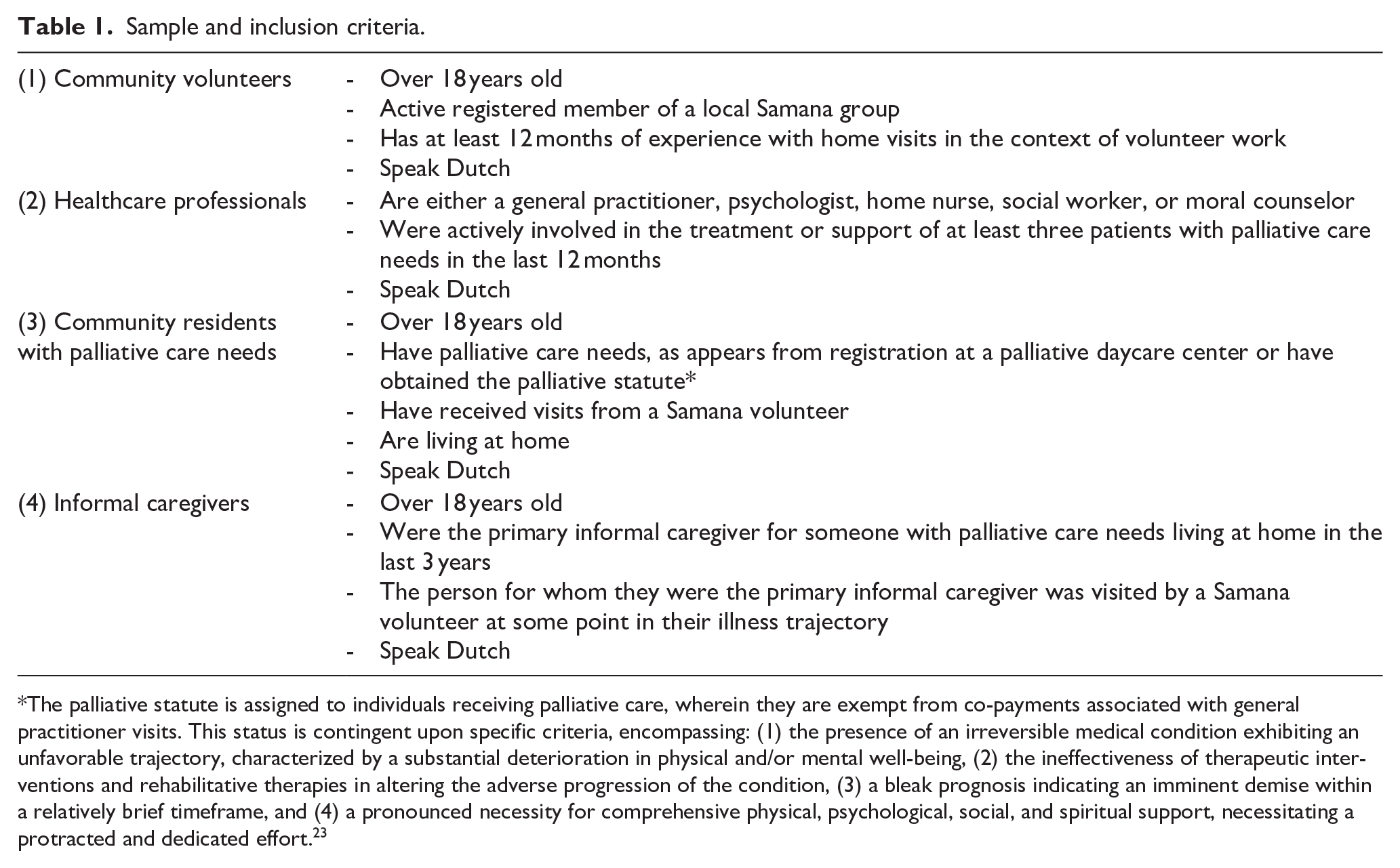
The palliative statute is assigned to individuals receiving palliative care, wherein they are exempt from co-payments associated with general practitioner visits. This status is contingent upon specific criteria, encompassing: (1) the presence of an irreversible medical condition exhibiting an unfavorable trajectory, characterized by a substantial deterioration in physical and/or mental well-being, (2) the ineffectiveness of therapeutic interventions and rehabilitative therapies in altering the adverse progression of the condition, (3) a bleak prognosis indicating an imminent demise within a relatively brief timeframe, and (4) a pronounced necessity for comprehensive physical, psychological, social, and spiritual support, necessitating a protracted and dedicated effort. 23
Participants of this study were recruited in Flanders, Belgium. First, community volunteers were recruited through local Samana groups in Flanders, and the recruitment process was facilitated by the educational officer of Samana in the province of Oost-Vlaanderen. Second, healthcare professionals were recruited through various channels in Flanders: (1) general practitioners were recruited from local general practitioner networks, (2) psychologists were recruited from dedicated palliative care services (i.e., palliative care units, palliative daycare centers, and palliative homecare teams), (3) homecare nurses were recruited from homecare nursing services, (4) social workers were recruited from local public centers for societal well-being and hospitals’ social services, and (5) moral counselors were recruited via the palliative homecare teams, hospitals, and a liberal humanist association. Third, community residents with palliative care needs and informal caregivers were recruited through the five Flemish palliative daycare centers, the six Flemish informal care associations, and by snowball sampling through the participating Samana community volunteers. The coordinators of these organizations facilitated recruitment for this study and contacted potential participants via mail. An information letter was sent, detailing the study and requesting their participation in the study. The letter also requested their consent to share their contact information with the researchers, and they were informed about pseudonymization and confidentiality regarding participation in the study. Contact details of willing participants were then shared with the executive investigator, who in turn contacted the participants by phone to plan the focus group or interview. Participants signed a written informed consent (Supplemental Appendix II) form before participating.
Data collection
Data was collected between November 2020 and June 2022. All focus groups took place online due to COVID-19 restrictions. With the exception of one final focus group, all other focus groups were kept internally homogeneous with regard to the participant group (community volunteers or healthcare professionals) to fully capture the perspectives of each participant group. One heterogeneous focus group was held to explore differences and interactions between community volunteers and healthcare professionals. People with palliative care needs living at home and informal caregivers were invited to participate in individual semi-structured interviews. All interviews were conducted in person, except for one with an informal caregiver and one with a person with palliative care needs living at home who were interviewed online. No interviews involved patient-caregiver pairs. Semi-structured interviews were conducted by S.V.S.; focus groups were moderated by S.V. and K.C. (See Supplemental Appendix III profile sketch of researchers involved). S.V.S., S.V., and K.C. made field notes during and shortly after the interviews or focus groups. Each participant in the focus groups and interviews was asked to fill out a short, written questionnaire (Supplemental Appendix IV) to capture their demographic characteristics, including sex, age, (current or last) occupation, location, and education. Topic guides for both interviews and focus groups, consisting of open questions and a set of prompts for each question, were developed and iteratively reviewed by the research team, consisting of sociologists (postdoc S.V., professor K.C., professor L.D.), a psychologist PhD researcher (S.V.S.), and an adult educational scientist (professor S.D.). All topic guides (Supplemental Appendix V) focused on the following key topics: volunteer role, relationship between volunteer and community resident, collaboration and communication between community volunteers and healthcare professionals, and experiences with volunteers. Participants were given the option to review their transcripts afterward upon request; however, the researchers received no such requests. In Supplemental Appendix VI, a reflection by the executive researcher (S.V.S.) can be found on the influence of her background, role, and position during data collection and data analysis.
Data processing
The interviews and focus groups were audiotaped and transcribed verbatim. All data were pseudonymized before processing, in accordance with the provisions of the law on personal data protection (GDPR). Transcripts were processed in MS Word and in NVivo, a software package for qualitative data analysis. 16 The demographic questionnaires were processed in Excel.
Data analysis
This qualitative research is driven by a social constructivist epistemology, recognizing the impact of contextual factors on interpersonal actions, viewing reality as dynamic and socially constructed, and interpreting human realities as shared and co-constructed meanings. Inductive qualitative thematic analysis was chosen to analyze the data because there is little literature on the research topic.24,25 The following iterative coding methods were used: (1) familiarization of data, (2) generating initial codes, (3) combining codes into themes, (4) reviewing themes, (5) determining the significance of themes, and (6) reporting of findings. 24 The analysis began with reading the transcripts by two authors (S.V.S., S.V.) to gain a global understanding of the content of the data. The data were coded by S.V.S. and S.V. and the coding framework was discussed on various occasions (weekly meetings between S.V.S. and S.V., and project group meetings every 6 weeks) and validated by all other authors. Generating initial codes includes identifying, naming, categorizing, and describing phenomena within the texts.24 –26 Both coders independently conducted a primary analysis of five transcripts (generating initial codes) and compared them with each other. S.V.S. then combined codes into themes. The identified initial codes were refined, merged, reduced, and related to each other.24 –26 SVS established relationships between the different codes to establish an overarching conceptual scheme with provisional themes and subthemes, which was discussed, reviewed, and validated by the authors (S.V., K.C., L.D., and S.D.). The final agreed-upon coding scheme was then applied to all transcripts. S.V.S. and S.V. independently used the conceptual coding scheme on the same interview transcripts to check for the validity and coherence of the codes and themes. The conceptual coding scheme was tested as such for multiple transcripts and adjusted where necessary by the project group until the researchers arrived at a coding scheme that represented each coder’s insights and was considered valid by the project group. Finally, this coding scheme was applied to the transcripts in a final coding round. The coding scheme (including main themes and subthemes) and associated quotes were structured into a table and used to create our final analysis. Data was analyzed in Dutch and the themes were brought together in a structured story in which the most important findings are written down. Only selected quotes included in this paper were translated into English. Theoretical saturation was defined at the point where new insights no longer added relevant changes or new information to the identified knowledge and skills of community volunteers to recognize, describe, and communicate palliative care needs.
Ethical considerations
The research protocol was approved by the Medical Ethics Committee of the Ghent university Hospital on November 10, 2020 (B.U.N.: B6702020000359). The data was coded using pseudonyms (Supplemental Appendix VII), maintaining a link with the participants.
Results
Fourteen community volunteers and 18 healthcare professionals took part in a total of seven focus groups. Focus groups lasted between 60 and 90 min. Six interviews were held with community residents with palliative care. Four interviews were held with informal caregivers. Interviews lasted between 45 and 90 min. The recruited informal caregivers had no personal relationship with the participating residents. Table 2 gives an overview of the characteristics of participants in focus groups and interviews.
Characteristics of participants in focus groups and interviews.

Among healthcare professionals: 5 nurses (27.78%), 4 general practitioners (22.22%), 4 moral counselors (22.22%), 2 psychologists (11.11%), 2 social workers (11.11%), and 1 palliative care network coordinator (5.56%).
Table 3 gives an overview of the conceptual scheme that was constructed from the data.
Conceptual scheme.
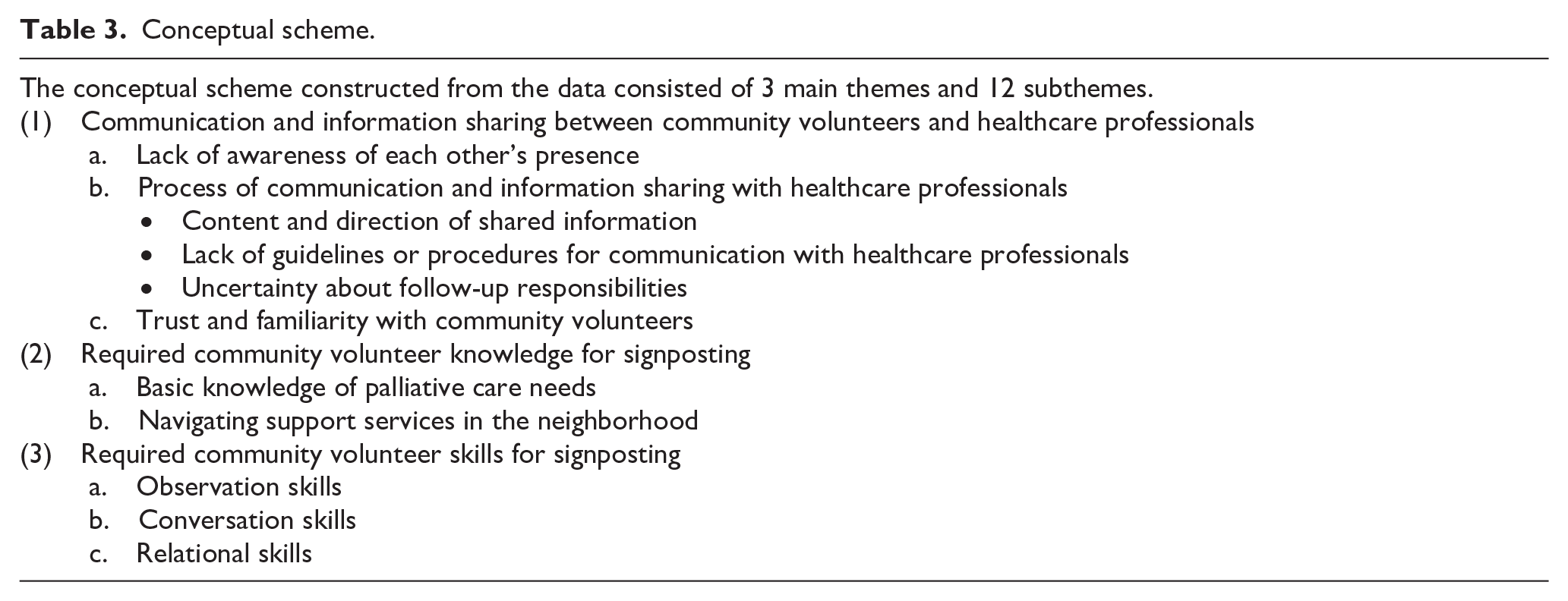
Communication and information sharing between community volunteers and healthcare professionals
This theme contains three subthemes: (a) lack of awareness of each other’s involvement, (b) process of communication with professionals, and (c) trust and familiarity.
Lack of awareness of each other’s presence
Participants from each target group (community volunteers, healthcare professionals, informal caregivers, and community residents) indicated that there was hardly any contact or collaboration between community volunteers and healthcare professionals. A community resident reported: “There is zero contact between my general practitioner and my volunteer, including nurses. According to my feeling, there is no collaboration” (IV-CR3). Similarly, an informal caregiver said: “The nurses and general practitioner maintain frequent contact, but our volunteer is a bit disconnected from these parties. While the volunteer is in very close contact with to us, I think there is no contact with healthcare professionals” (IV-IC2).
Community volunteers and healthcare professionals visited community residents at different times, preventing interaction between the two. As one community resident indicated: “Everyone visits me at a different time. For example, the nurses often come very early in the morning or during evening while the volunteer comes in the afternoon” (IV-CR5). Community volunteers therefore often stay under the radar of healthcare professionals. A community volunteer said: “I don’t know which professionals are involved or who visits the patient. I have no idea who all is involved in the care process. I haven’t met the other people involved” (FG2-CV3).
This lack of awareness between community volunteers and healthcare professionals regarding each other’s involvement in the eyes of participants led to missed opportunities for collaboration. In addition, healthcare professionals are often not aware of the volunteers’ roles, responsibilities, and potential contributions to the care process. A healthcare professional stated: “While performing my duties as general practitioner, I have never met a volunteer. In fact, I do not know of their existence, and I don’t immediately think of them as potential partners to collaborate with” (MFG-HCP2).
Healthcare professionals reported that they engaged with one another during multidisciplinary patient consultations, fostering awareness of each other’s involvement, roles, and tasks, but that volunteers do not participate in these consultations: “I see other care providers at multidisciplinary meetings. This way you know who is involved and you can also put a face to it. If the patient talks about a specific nurse, you also know who it is. Volunteers are not present” (FG5-HCP1).
Process of communication and information sharing with healthcare professionals
Content and direction of shared information
When describing information shared between community volunteers and healthcare professionals, participants reported information communicated by community volunteers to healthcare professionals. This information entailed updates regarding changes in the patient’s condition, including both physical and emotional aspects, as well as the patient’s wishes and needs. A community volunteer explained it this way: “I will speak to a general practitioner if I am concerned about the community resident that I am visiting. If I suspect that someone can no longer live independently, I will discuss this with the doctor” (FG2-CV2). In the same line, a healthcare professional reported: “A volunteer will contact a healthcare professional to communicate concerns about the patient’s well-being or a change in care needs” (FG6-HCP2). Other information that was shared related to community residents’ financial difficulties and problems such as neglect, social isolation, or conflict among residents personally. Information was not reported to be shared by healthcare professionals with community volunteers, and healthcare professionals were reported as not typically providing feedback or updates to community volunteers. This one-way communication highlighted a gap in the bidirectional exchange of information, as healthcare professionals did not typically provide feedback or update volunteers. A community volunteer mentioned: “The communication is rather one-sided. For example, if I report a concern about someone’s health, I do not receive any further updates on the progress or what has been done about it” (FG2-CV3).
Community volunteers described how privacy laws and regulations impact information sharing between them and healthcare professionals. These regulations apply to medical records or electronic data exchange among healthcare professionals. Community volunteers noted that these privacy rules often prevent healthcare professionals from sharing relevant information with them, even though such information could be beneficial for the care they provide. A community volunteer stated: “The privacy law limits general practitioners to give feedback to volunteers regarding the people we visit. They are not always allowed to share all information with us, even though this would be very relevant to us” (FG1-CV2).
Healthcare professionals indicated their commitment to confidentiality. They explained that information shared in confidence by a community resident with care needs cannot be freely disclosed to community volunteers, to uphold principles of privacy and confidentiality. The same applies to information shared in confidence by a community resident with a community volunteer; it does not always flow through to the professional due to the confidential content.
Lack of guidelines or procedures for communication with healthcare professionals
Community volunteers reported that their organization does not provide guidelines or procedures for communication and information sharing with healthcare professionals. Instead, volunteers developed their own strategies for identifying and addressing care or support needs. When volunteers observe specific needs, they seek approval from residents with care needs or informal caregivers before sharing this information with healthcare professionals. A community volunteer reported: “Before I discuss anything with the general practitioner, I always first consult with the resident to get their permission” (FG2-CV1).
Volunteers indicated it was possible to discuss difficulties and doubts regarding communication with healthcare professionals with other volunteers in their group. A community volunteer explained it as follows: “For sensitive matters such as neglect and hygiene, I will discuss this with my core group. Due to the complexity of this matter, the coordinator of the core group will sometimes take over and also report this need or concern to the involved healthcare professionals” (FG3-CV3). Volunteers reported that the group coordinator and other volunteers advised each other on the best ways to communicate identified needs. In exceptional cases, the coordinator may take over the communication with healthcare professionals or relevant care services.
Uncertainty about follow-up responsibilities
Both community volunteers and healthcare professionals agreed that when a community volunteer signposted identified needs toward a healthcare professional, the responsibility for follow-up lies with the healthcare provider or care service involved. However, some volunteers noted that the boundaries of their own responsibilities are unclear due to the absence of a formal role description regarding communication and follow-up. A participating community volunteer stated: “When volunteers report something to a professional, it stops there for them and it is up to the professional to follow up. Of course, this is an unwritten rule, so it is not always clear where your responsibility stops” (FG1-CV2).
Trust and familiarity with community volunteers
Community volunteers sometimes faced resistance from healthcare professionals, mainly due to a lack of trust and awareness about each other’s involvement, roles, and responsibilities. This lack of awareness extended to not understanding the potential value they could have for each other or how they might collaborate in the context of patient care. A community volunteer stated: “Volunteers often remain under the radar and are usually forgotten as an involved and valuable party. We are often not accepted and trusted in the input we provide” (MFG-CV1).
Both community volunteers and healthcare professionals highlighted the importance of getting to know each other and familiarizing themselves with each other’s roles, functions, and responsibilities to enhance mutual appreciation, communication, and collaboration. A healthcare professional described it as follows: “It is important that volunteers and healthcare providers get to know each other. Connections must be sought between both parties. This way they can appreciate each other, and potential resistance and mistrust will decrease, making cooperation possible” (MFG-HCP2).
Community volunteers and healthcare professionals noted that the working relationship between them affects mutual communication and collaboration. They stressed that healthcare professionals’ better understanding of volunteers’ roles, functions, and responsibilities is crucial for fostering mutual appreciation. Community volunteers highlighted that positive relationships or previous successful collaborations with healthcare professionals facilitate better communication and information sharing. Two community volunteers described this positive impact as follows: “A good relationship with healthcare providers has a positive effect. It is easier to report or discuss matters if you already know certain healthcare providers and have a good contact with them. For example, I have a very good relationship with a social worker and I find it easier to report certain difficulties or needs of the patient towards her” (FG1-CV3), and “Previous positive collaborations between volunteers and healthcare professionals can positively influence the communication process. If a previous collaboration went well, it is also easy to contact each other again in the future. You can also better estimate what you can do for each other” (FG2-CV1).
Required volunteer knowledge for signposting
This theme contains two subthemes: (a) palliative care needs and (b) care services in the neighborhood.
Basic knowledge of palliative care needs
Community volunteers, informal caregivers, and healthcare professionals highlighted the importance of community volunteers having basic knowledge about palliative care needs for community volunteers to respond and take up their signposting role. A community volunteer said: “I think volunteers need some training regarding general palliative care. Knowledge about palliative care is necessary to understand what palliative care is and what kind of needs palliative patients are faced with” (FG2-CV2). In the same line, an informal caregiver expressed: “It is important that volunteers are aware of the diagnosis of the person they are visiting and what the impact is. If they know something about the symptoms of a certain disease, the prognosis and the associated care needs, that is a plus. If someone is deteriorating more and more, it is good to know what someone needs so that they can respond better” (IV-IC1). According to healthcare professionals, this basic palliative care knowledge included knowledge of the different types of palliative care needs, the organization of palliative care in Flanders, pain and symptom management, advanced care planning, possible wishes regarding death and the circumstances of death, and grief and loss. A healthcare professional reported: “It is important that volunteers have a basic knowledge of the organization of palliative care in Flanders and possible care needs that may arise in a palliative process. A basic knowledge of this will help them to recognize these care needs in their volunteers, in the people they visit. These are physical, social, emotional and existential care needs” (FG4-HCP2). Another healthcare professional reported: “It would be interesting if they have some background about pain and symptom control, and have some knowledge about possible wishes and circumstances of death. This will also help volunteers to respond appropriately if a patient would express their wishes towards them” (FG4-HCP1). In addition, healthcare professionals indicated that a basic understanding of these topics is sufficient but that community volunteers are not expected to become experts: “It is important that community volunteers develop a basic understanding of palliative care and care needs. The intention is absolutely not for them to become experts in this field” (FG5-HCP1).
Navigating support services in the neighborhood
Both community volunteers and healthcare professionals suggested it was important for volunteers to have a basic knowledge of available social and healthcare services in the area of the community resident they visited. This knowledge was considered valuable in helping community volunteers assess what needs to be flagged or what information to signpost to healthcare professionals. A community volunteer explained: “It would be helpful for us volunteers to have access to a list of organizations or healthcare professionals to contact in case of questions or difficulties. Right now, sometimes it is unclear and we lack knowledge about who to turn to or what organizations are active in the neighborhood” (FG3-CV1). A healthcare professional also indicated that this knowledge can contribute to more effective signposting: “Volunteers should be aware of where to signpost identified care needs, without the expectation that they possess knowledge of the entire social landscape. Having knowledge of key care organizations and facilities in the area adds value and facilitates quicker and more adequate signposting” (FG6-HCP1).
Required volunteer skills for signposting
This theme contains three subthemes: (a) observational skills, (b) conversation skills, and (c) relational skills.
Observational skills
Healthcare professionals highlighted that strong observational skills are a valuable asset for community volunteers; volunteers did not report on this topic. Professionals noted that due to the significant time volunteers spend with community residents, they can detect changes in the environment, physical condition, or emotional state that other healthcare professionals might overlook. These observations can offer valuable insights into the quality of life of the residents. A healthcare professional described it as follows: “A volunteer has time and can observe whether a patient is becoming more in need of help. Based on observations, an estimate can be made as to whether the situation is still livable” (MFG-HCP1). Another healthcare professional highlighted that the psychological bond and the time volunteers and residents spend together may have a positive impact on observing care needs: “Community volunteers are psychologically closer to the patient, which can ensure that patients are more likely to share sensitivities or difficulties with this volunteer. They have time to observe changes in environment, physical condition and emotional state. This is not always possible during a short contact moment with a healthcare professional. Volunteers can act as the eyes and ears of the experts” (FG6-HCP2).
Conversation skills
Community volunteers and healthcare professionals agreed that good conversation skills, including listening and communication abilities, are crucial. These skills help volunteers connect with community residents and their loved ones, build trust, and assess their needs.
Healthcare professionals did not specify what these conversation skills should include. According to community volunteers, effective conversation skills involve active listening, understanding the content being communicated, and using open-ended questions. They stressed the importance of being sensitive to what a community resident with care needs wishes or hesitates to express and adapting communication to the resident’s pace. A community volunteer reported the following: “For me, listening is the most important skill a volunteer should have. You must be able to listen actively. You have to concentrate and connect with the patient’s story. You have to try to understand what is being said and be able to respond appropriately, always taking into account the patient’s pace” (FG2-CV2). Similarly, an informal caregiver said: “It is mainly that listening, listening is indeed important; it’s a key skill volunteers must have. They need to listen carefully and respond appropriately to the emotions and concerns we share” (IV-IC3).
Community volunteers, healthcare professionals, and community residents indicated the importance of asking open, non-threatening, and clarifying questions. A community volunteer said: “A volunteer must be able to ask the right questions in a conversation in a non-threatening way. By asking the right questions you can find out relevant things about someone’s quality of life” (FG3-CV1). A community resident stresses the importance of being attentive to what a patient does or does not want to share, he described it as follows: “People sometimes don’t know what to do or what to ask. They see you as something special and think they have to constantly ask how you are doing and whether I understand everything. Constantly asking ‘How are you?’ and ‘How are you feeling?’. Why do they always have to ask that? It’s not going well. I have cancer. Sometimes it’s better not to ask questions or just ask about what I did today. Sometimes you have to approach us as if we are not sick” (IV-CR2).
Finally, healthcare professionals indicated the importance of exploring care needs during communication with community residents. A participating healthcare professional stated: “A volunteer must be able to further explore care needs through communication. By asking open questions and asking additional questions, a volunteer can make a better assessment of the care needs of residents.” Another healthcare professional stressed the need to offer help and care resources respectfully: “As a volunteer you must be able to respond appropriately to the complex situations you find yourself in during home visits. If the community resident would benefit from extra help according to the volunteer, it is important to discuss this in a respectful manner” (MFG-HCP1).
Relational skills
In addition to observational and communication skills, community volunteers and healthcare professionals highlighted the importance of relational skills. Community volunteers discussed several key relational skills, including being present for the person with care needs and their loved ones, providing companionship, responding empathetically, building trust, connecting with the community resident’s living environment and informal caregivers, and balancing distance with closeness. A community volunteer said the following: “A volunteer must have an open and non-judgmental attitude towards the patient’s story and living environment. In a conversation with a patient or informal caregiver, it is important to follow their story and not overload them with your own conclusions, personal opinions or assumptions” (FG3-CV1). In the same line, an informal caregiver reported: “My husband loved to travel and enjoyed reading. Our volunteer knew this and would read to him from books or the newspaper. They would also look through photo albums of trips we had taken and talk for hours. I think it’s very important for a volunteer to connect with the interests and living environment of those they visit. By doing these things, other topics gradually start to be shared like suffering or certain concerns about the future” (IV-IC4). In addition, the importance of creating a safe environment was discussed so that community residents with care needs can share their stories in a safe context, at their own pace. A community volunteer reported: “As a volunteer, it is important to connect with the living environment of the community resident and create a safe space. You need to be able to sense when to bring up certain topics and when to hold back. This of course also depends on the level of trust and something like that has to grow” (FG2-CV4). A community resident also discussed the importance of creating a safe environment: “Over time, a sense of trust developed between me and my volunteer. She shares things about herself, and I share things about myself. That trust wasn’t there from the start, it takes time to grow. As a volunteer, you should be able to create an atmosphere where it feels safe to share and ask things, but that doesn’t happen over one night” (IV-CR5). Healthcare professionals indicated that it is crucial for community volunteers to manage the emotions of community residents with care needs and their loved ones effectively, and to respond appropriately. A healthcare professional reported: “Community volunteers must be able to deal with the emotions and tensions they encounter with the patients they visit. Anticipating and responding adequately to the behavior and emotions of the patient and his family will contribute to a better relationship between both parties” (FG5-HCP2).
Discussion
Main findings
The study highlights significant gaps in communication and collaboration between community volunteers and healthcare professionals in the care of community residents with palliative care needs, revealing several key areas for improvement and integration. First, communication or information sharing between community volunteers and healthcare professionals is sporadic, infrequent, or nonexistent. They often lack awareness of each other’s involvement and healthcare professionals are not familiar with the role and added value of community volunteers in the care process of community residents with palliative care needs. Communication tends to be unidirectional, from community volunteers to healthcare professionals, the latter questioning community volunteers as valuable communication partners. Second, our study highlights the necessity for community volunteers to understand various palliative care needs, have basic knowledge of available community resources, and possess strong relational, communication, and observation skills. Finally, community volunteers should also pay attention to changes in community residents’ physical environment or emotional state and communicate their role effectively to healthcare professionals, seeking to understand how they can collaborate to support the individual’s care needs.
Interpretation
Contact between volunteers and healthcare professionals is missing, but very much needed
Due to the perceived hierarchy and lack of collaboration, community volunteers face multiple barriers in signposting identified needs. These findings are consistent with earlier research indicating that a disconnect between stakeholders within the healthcare system impedes successful signposting. 27 Interprofessional collaboration can facilitate smoother collaboration, communication, and information sharing.28,29 However, based on our findings, prerequisites such as willingness to collaborate, communication skills, and mutual trust are possibly insufficiently met.
Our study shows that the bridge between community volunteers and healthcare professionals to achieve good signposting is missing. Inviting community volunteers to participate in multidisciplinary consultations when relevant is one option to bring both parties closer, however, practical implementation may be difficult due to privacy laws, organizational culture, and internal rules that may shun community volunteers altogether.29,30 In addition, there is a risk in professionalizing volunteers as their unique contribution lies in their non-healthcare provider status; something which volunteers have been shown to be averse to. 30 Our study highlights instead the importance of providing community volunteers with communication tools and increasing their self-confidence to effectively introduce themselves to healthcare professionals and signpost care needs. In addition, it is important to create awareness among healthcare professionals about the added value of community volunteers and the unique contribution they can make. Experiences from specialized palliative care can help create this awareness because in this context there is already a tradition in which volunteers and healthcare professionals work together effectively.31,32 Palliative care networks in Flanders could better focus on sharing and promoting positive experiences of healthcare professional–volunteer collaboration, especially since there is already a long tradition of cooperation within these networks.
Importance of role clarity and discussing this role with healthcare professionals
We found that community volunteers are not always aware of their contribution to palliative care and potential signposting roles. Earlier research showed that a lack of clarity about the purpose of the volunteer role may affect the potential or success of signposting by generating distrust or uncertainty among patients and healthcare professionals about volunteers’ ability and the sustainability of volunteers to undertake a role and function in general practice.27,32 –34 Awareness of the volunteer role, its complementarity, and a sense of shared responsibility between healthcare professionals and volunteers can contribute to better volunteer-professional collaboration.27,32 –34 This complementarity can be better utilized when volunteers are visible and known to the healthcare professionals in the care network of the community residents, and by encouraging communication, making task agreements, exchanging information, and forming networks between volunteers and healthcare professionals.19,27 –30 Based on the results of this study, to facilitate volunteer-professional collaboration, community volunteers and healthcare professionals should discuss their roles and agree on what they can mean for each other and how they can best collaborate and communicate. One important study finding in this regard is that the community volunteer role boundaries are sometimes unclear. It is therefore crucial to define and demarcate the boundaries of the community volunteer role on the policy level to prevent professionalization and avoid unnecessary interference of community volunteers in the care process. Coordinators can negotiate these boundaries with their volunteers.
The need for adequate training, supervision, and a community of practice
While attention is sometimes paid to referrals in volunteer training modules (e.g., “Compassionate Neighbors,” 35 “Compassionate Communities Connectors,”36,37 “NavCare/EU Navigate,”38,39 “EASE,” 40 or “iLIVE” 41 ), signposting is not systematically embedded in any palliative care volunteer training or support initiatives. Brunton et al. 27 demonstrated that signposting can be hindered by a lack of training and skills development. Even individuals who are willing to expand their roles may feel ill-equipped to accurately assess patients’ needs and effectively direct them to sources of assistance.27,42 In addition, respondents of this qualitative study indicated a need for supervision to help them take up their signposting role and the possibility to exchange experiences and knowledge with other volunteers. This is in line with previous research,27,43 which highlights the importance of ensuring sufficient supervision and training to help those in signposting roles to feel supported.27,42 –44 Volunteers desire ongoing education and a chance to be connected with others who understand the difficulties of their role. 35
Research has shown that community volunteers receive the least supervision and rate their supervision the lowest in comparison to other volunteers in palliative care.8,18 While community home care is entirely volunteer-run at the local level, the lack of supervision or guidance from the organization may signal a need for structural support and training interventions.8,18 It is therefore appropriate to organize fixed supervision moments for community volunteers. This requires the presence, availability, and approachability of healthcare professionals and frequent contact between them. A community of practice in which community volunteers can share their knowledge, expertise, and experiences, and learn from each other can also help them deal with the problems and challenges in their encounter.
Recommendations for policy, practice, and future research
To facilitate collaboration, information sharing, and signposting, it is crucial to assess and evaluate the involvement of community volunteers in the care trajectories of patients with palliative care needs living at home. To reduce mistrust and perceived hierarchy, actions can include intervision sessions for volunteers to facilitate peer support, volunteer role clarification workshops for healthcare professionals, communication guidelines to enhance information exchange and collaboration, and including volunteers in interdisciplinary meetings. Policy can play an active role in stimulating and facilitating the structural integration of community volunteers into multidisciplinary consultation about community residents with palliative or chronic care needs. Volunteer coordinators, who have a close relationship with community volunteers or are community volunteers themselves, can play a key role in defining the core competencies for community volunteers and can facilitate the organization of training while avoiding professionalization of volunteers. In addition, community development initiatives that support people faced with serious illness, family caregiving, death, and loss (e.g., Compassionate Community programs) often rely on volunteers and other informal support networks to support and connect people with care and support needs to neighborhood resources and health services.45 –47 Such initiatives should consider both (1) supporting their volunteers in developing the knowledge and skills necessary to identify and communicate needs among their community members, and (2) to raise awareness and recognition among healthcare professionals of the presence, role, and value of volunteers as care network members. By acknowledging volunteers as valuable communication and collaboration partners, healthcare professionals are more likely to address the needs conveyed by them.
Future research should focus on the development and evaluation of a community of practice and a training program for community volunteers that focuses on strengthening knowledge and skills with regard to their signaling function. The self-confidence of community volunteers will be enhanced when they are explicitly valued for their work when they are provided tools that assist them in effective communication and signposting, and having channels to exchange experiences with fellow volunteers. Future research should also investigate how volunteer-professional dynamics influence patient-care outcomes, more specifically how communication gaps impact patients’ quality of care. Given that our results indicated one-directional communication from community volunteers to healthcare professionals, it may be valuable to study how professionals can better involve community volunteers in the patient-care trajectory and how they can effectively provide feedback to volunteers.
Strengths and limitations
This study is the first, to our knowledge, to systematically describe the desired knowledge and skills for community volunteers to recognize, describe, and communicate palliative care needs to healthcare professionals. This study complements the existing literature about community volunteering in palliative care and enhances our understanding of communication and information sharing between community volunteers and healthcare professionals. The strength of the study lies in the inclusion of multi-stakeholder perspectives. The same core topics emerged from interviews and focus groups with all participant groups, indicating the relevance and importance of the findings. An exception relates to the themes of information sharing and collaboration between volunteers and healthcare professionals, informal caregivers and community residents stated that was not existent, resulting in no input on the content, the direction of shared information, communication guidelines, procedures, or follow-up responsibilities.
First, this study is limited to a unique form of community volunteering, and we should therefore take care in generalizing these insights. Although different forms of community-based volunteering can benefit from the findings of this study, they should adapt them thoughtfully to their specific contexts. The second limitation relates to recruitment. The COVID-19 pandemic had a negative impact on the recruitment of residents, informal caregivers, and volunteers. Most volunteering activities within Samana were canceled during this time, and community volunteers were prohibited from conducting home visits for most of 2020 and 2021 due to COVID-19 guidelines. Home visits resumed in early 2021, but many residents with palliative care needs who had previously received home visits have since passed away. When visits restarted, volunteers were matched with new community residents, but their experience was too brief to include in the study. As a result, additional interviews were conducted with informal caregivers to capture the perspectives of deceased residents through their accounts. Third, next to recruitment challenges, a self-selection selection bias is likely. Participants were recruited through intermediaries (e.g., an educational employee at Samana, a homecare nurse at Wit-Gele Kruis, and a palliative network coordinator). While this was necessary for identifying participants, it limited control over the recruitment process, leaving us unaware of how many people were contacted, the nonresponse rate, or the reasons for nonparticipation. This likely resulted in an overrepresentation of highly motivated community volunteers, while community residents with palliative care needs and informal caregivers with negative experiences may have been less likely to participate. Another limitation regarding recruitment relates to the extent to which volunteers perceive the individuals they visit as having palliative care needs and are aware of their own contribution to palliative care. Consequently, a group of volunteers who do not immediately recognize themselves in the description of our target group may therefore not have been reached. However, these volunteers are indeed eligible and may have unique insights that were likely missed in this study. An additional limitation due to the COVID-19 pandemic was the necessity of conducting focus groups online. While moderators ensured each participant participated actively in the discussions, the virtual format nonetheless may have discouraged more reserved participants from openly sharing their experiences, meaning that some relevant insights may not have been captured. Despite the researchers’ efforts to include the views and experiences of multiple stakeholders, the results show an overrepresentation of input from community volunteers and healthcare professionals, as opposed to community residents and informal caregivers. Community residents and informal caregivers probably found it more difficult to reflect on collaboration, communication, knowledge, and skills. This may be because these topics were further removed from their own experiences. Face-to-face interviews may also have allowed more in-depth exploration of these topics than was currently achieved via digital interviews.
Conclusion
To effectively recognize, describe, and communicate patient palliative needs and wishes, volunteers require specific skills and knowledge, which can be acquired through training. Based on the findings of this study, a training program for volunteers should focus on (1) increasing awareness and knowledge of the community volunteer role and the signposting function; (2) increasing knowledge about palliative care, palliative care needs, and access to care services; (3) strengthening and improving communication with community residents (and relatives); and (4) strengthening and improving communication with caregivers. The next step of this research project is the development of a training program in which community volunteers can share their knowledge and experiences, and learn from each other to better deal with the problems and challenges in their volunteer work.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251334184 – Supplemental material for What knowledge and skills are needed for community volunteers to take on a signposting role in community-based palliative care? A qualitative study
Supplemental material, sj-docx-1-pcr-10.1177_26323524251334184 for What knowledge and skills are needed for community volunteers to take on a signposting role in community-based palliative care? A qualitative study by Sabet Van Steenbergen, Steven Vanderstichelen, Luc Deliens, Sarah Dury and Kenneth Chambaere in Palliative Care and Social Practice
Footnotes
Ethical considerations
The research protocol was approved by the Medical Ethics Committee of the Ghent university Hospital on November 10, 2020 (B.U.N.: B6702020000359).
Consent to participate
Participants signed a written informed consent form before participating.
Consent for publication
Participants signed a written informed consent form before participating.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of a larger research project “Attentive visitors’ in-home care: development and pilot testing of a volunteer training in assessment and communication of psychological, social and existential care needs,” funder by Kom op tegen Kanker (Grant number PSC 17/6/19 – 000140946) and the Flemish Research Fund (FWO) under Grant number 1200424N.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data of this study is kept by the first author and is available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.