
Abstract
Background:
Past studies have shown mixed results on how gender and living with a spouse or partner impact advance care planning (ACP). Few if any have tested for the interaction between these two variables.
Objective:
We examined how gender and couple status interact to impact the use of ACP practices including written instructions, designating a durable power of attorney for healthcare (DPOAHC), and discussing one’s decisions with others.
Design:
We used cross-sectional data taken from the Health and Retirement Study, a longitudinal study of adults over the age of 50 in the United States.
Methods:
Data are from 632 respondents who died between the 2016 core survey and the 2018 exit survey. Participants had completed the 2016 survey and had a proxy informant complete the 2018 exit survey after their death. Generalized linear mixed models were used to test for main effects and interactions.
Results:
Women were more likely than men to designate a DPOAHC and to discuss their wishes with others. Women living without a partner were more likely than men living without a partner and coupled households to discuss their wishes with family or others.
Conclusion:
Both gender and couple status are important variables associated with ACP practices. Healthcare providers may want to reach out to women living within a coupled household and men living without a partner to ensure that they know the benefits of ACP.
Plain language summary
Why was the study done? To see if men and women living alone or with a partner were more likely to make plans for the type of medical treatment they preferred at the end of life. We examined whether they had written plans, designated someone to make decisions for them, or discussed their wishes with other family members or healthcare providers before they died.
What did the researchers do? The research team used survey data from the Health and Retirement Study in the United States on 632 people who had completed a survey in 2016 and died within two years. A family member or friend completed a survey after the person’s death reporting on their preferences for end-of-life medical care.
What did the researchers find? Women were more likely than men to designate another person to make medical decisions for them and to discuss their wishes with others. Single women were more likely than single men and people living with a partner to discuss their wishes with family or others.
What do the findings mean? Women living alone may be more likely to see the benefits of making their end-of-life medical care wishes known to others. Men living alone were the least likely to make their wishes known. Healthcare providers may want to keep these differences in mind when reaching out to patients to explain the benefits of making plans for medical treatments in the future.
Introduction
Advance care planning (ACP) is an ongoing process for individuals of any age to discuss their values and goals for future medical care. This process ensures that they receive care consistent with their values and goals. 1 The roots of ACP in the United States are often traced to the passage in 1990 of the Patient Self-Determination Act. 2 This legislation required legal documents called advance directives (ADs) to communicate decisions about end-of-life care. The most familiar types of ADs are living wills and durable power of attorney for healthcare (DPOAHC). Living wills address patient wishes regarding treatments like cardio-pulmonary resuscitation, intubation, and mechanical ventilation. DPOAHC identifies a person to make medical care decisions for patients who can no longer do so for themselves.
In the 1990s, Physician’s Orders for Life-Sustaining Treatment (POLST) began to be gradually adopted by individual states in the United States. 3 The POLST outlines the wishes of individuals regarding their medical conditions and goals of care. Unlike ADs or living wills, the POLST document is signed by a healthcare professional and follows individuals between multiple care settings such as nursing homes, clinics, and hospitals to instruct other providers with specific details regarding their wishes.
Thus, the conceptualization of ACP has evolved. Yet, knowledge of ACP by both professionals and non-professionals is often low. 4 Typically, it has been examined in older adults and those with disease specific conditions (e.g., heart failure or chronic obstructive pulmonary disease), but many are now advocating that ACP be normalized and regularly begun and reviewed at key life milestones like marriage, divorce, parenthood, and military enlistment.5,6 In spite of increased calls globally for greater education on and use of ACP4,7,8 and calls by many professional and government agencies (e.g., the American Geriatrics Society) 9 ACP is underutilized and its adoption and use is not adequate.9,10
ACP is a complex process influenced by characteristics of the individual (e.g., illness trajectories and sociodemographic factors like age, gender, and relationship status), the healthcare provider and patient relationship (e.g., physician, nurse, or social worker), and the environment in which the person lives or encounters healthcare services. However, there are many unanswered questions about the process as ACP is deeply personal, and there is no one-size-fits-all.
Two variables at the individual level of analysis, gender, and couple status, warrant further investigation as family is often cited as integral to ACP, and family dynamics are a known influence on ACP.11,12 Both are routinely used to describe the demographic make-up of the samples in studies of ACP,13–15 and studies have been done to explore their impact on the completion of ACP activities. There is still much to learn as the constructs of couple status and gender have evolved over time.11,16
Couple status has been shown to play a significant and often interrelated role in health behavior and health outcomes for several conditions like diabetes, heart failure, depression, and frailty 17 and in end-of-life decision-making. 18 There may be several reasons why women might be more engaged in ACP than men. Women have traditionally been the healthcare decision-makers and caregivers in families, with some estimating that women make 80% of healthcare decisions.19,20 Beyond engagement differences in caregiving, Perkins et al. 21 found that women and men may experience the healthcare system differently, with women more likely than men to trust the healthcare system to follow their desired wishes for end-of-life care. For example, work on couple status by Cooney et al. 12 found that divorced and widowed women were more likely to engage in ACP practices than married women. In contrast, divorced men were less likely than married men to have engaged in ACP practices. However, Cooney et al. did not test for an interaction or moderating effect between gender and couple status.
The effects of gender and marital status have been inconclusive. Some researchers reported that men are more likely than women to engage in ACP,7,13 but other researchers reported the opposite,22–25 or no gender differences. 26 Similarly, Hopp 27 found that persons who are not married but have children are more likely to have ADs and ACP discussions than those who are married and have children; other studies reported no marital status differences in ACP activities.25,26
Although gender has been historically framed dichotomously (male or female) and couple status has traditionally been framed in terms of marital status (married, divorced, or never married), these conceptualizations are evolving and require new research reflecting the changing definitions and patterns.28–30 Both gender and couple status represent two social determinants of health that need further exploration as their conceptualizations evolve, especially given few ACP studies that have used them as predictor variables or examined the statistical interaction between them. 18
In this study, we extend past research by using statistical models that test for the interaction between couple status and gender while controlling for other sociodemographic factors that have been shown to be correlated with ACP such as age, race, and socioeconomic status.13,25,29,31 We hypothesize that gender moderates the relationship between couple status and ACP activities, including having a written AD, designation of a DPOAHC, and discussion of ACP with a family member or others. Findings about gender role and couple status may help providers across settings educate patients and adapt ACP discussions to patient and family preferences. 7
Methods
Study design and sample
Data for this study are from the Health and Retirement Study (HRS), a national longitudinal cohort study of adults over the age of 50 years living in the United States funded by The National Institute on Aging (grant number NIA U01AG009740) and conducted at the University of Michigan Institute for Social Research. 32 Participants had to be over the age of 50 and living in the community (non-institutionalized) to be included in the study. If a person had a spouse or partner living in their household, that person was also included in the study. This large nationally representative study has high response rates of 70%–93% reducing the likelihood of selection bias.
We used 2016 Core Survey data from the RAND HRS Fat File and 2018 HRS Exit data. The RAND HRS Fat File combines several waves of data into an easy-to-use public data set. The HRS follows adult respondents over age 50 until their deaths. After their death, an exit survey which includes questions about ACP, is completed by a proxy informant, often a family member.
A sample of 632 respondents who died and had a proxy informant reply to each ACP outcome question were included in our analysis. Because our analysis included controlling for household poverty status, we simplified the analysis and focused only on community-dwelling adults, those who had not been in a nursing home or other institution at the time of the 2016 core interview. Approval for this secondary data analysis of the HRS data was obtained from Northeast Ohio Medical University’s Institutional Review Board.
Variables
The three main ACP outcome variables from the 2018 exit interviews included answers to three separate questions: whether the descendent had written instructions about treatment or care at the time of death (yes/no), had made legal arrangements for a specific person to make decisions about their healthcare (DPOAHC, yes/no), and had discussed their wishes with their family or others (yes/no). These variables were not mutually exclusive, a participant could have done none, one, two, or all three of these ACP activities.
All demographic variables were from the 2016 Rand Fat file. The two main predictor variables included gender (male or female) and whether the respondent lived in a coupled household (yes or no). In this wave of data, gender only included a dichotomous variable. Coupled households were comprised of married respondents and those living with a partner in 2016. We controlled for age, years of education, poverty status (yes/no), and race and ethnicity (Hispanic, non-Hispanic Black, non-Hispanic White, and non-Hispanic other race/ethnicity) in our multivariate models.
Data analysis
Chi-square tests were performed to examine bivariate relationships and generalized linear mixed models were used for the multivariate analysis (SAS version 9.4 Glimmix procedure by the SAS Institute in Cary, North Carolina). This allowed us to adjust for the variation within households since more than one person from a household could be included (12 cases included both partners from a household who died within the 2-year period). Unstandardized coefficients and standard errors are reported for each model.
The reporting of this study conforms to the STROBE guidelines for cross-sectional studies 33 (Supplemental File).
Results
The sample included 632 respondents with complete data who had died within 2 years of the 2016 biennial survey. As shown in Table 1, a greater proportion of men were living with a partner than were women (68% vs 28%, p < 0.0001) at the time of the 2016 survey, as one might expect. About 19% of the sample identified as non-Hispanic Black and 9% as Hispanic. Men were more likely than women to have 16 or more years of education (20% vs 13%, p = 0.02) but had a similar mean level of education (12 years). Men were less likely than women to have a household income below the poverty level (12% vs 21%, p = 0.002).
Characteristics of respondents by gender from the 2016 Health and Retirement Study biennial survey.
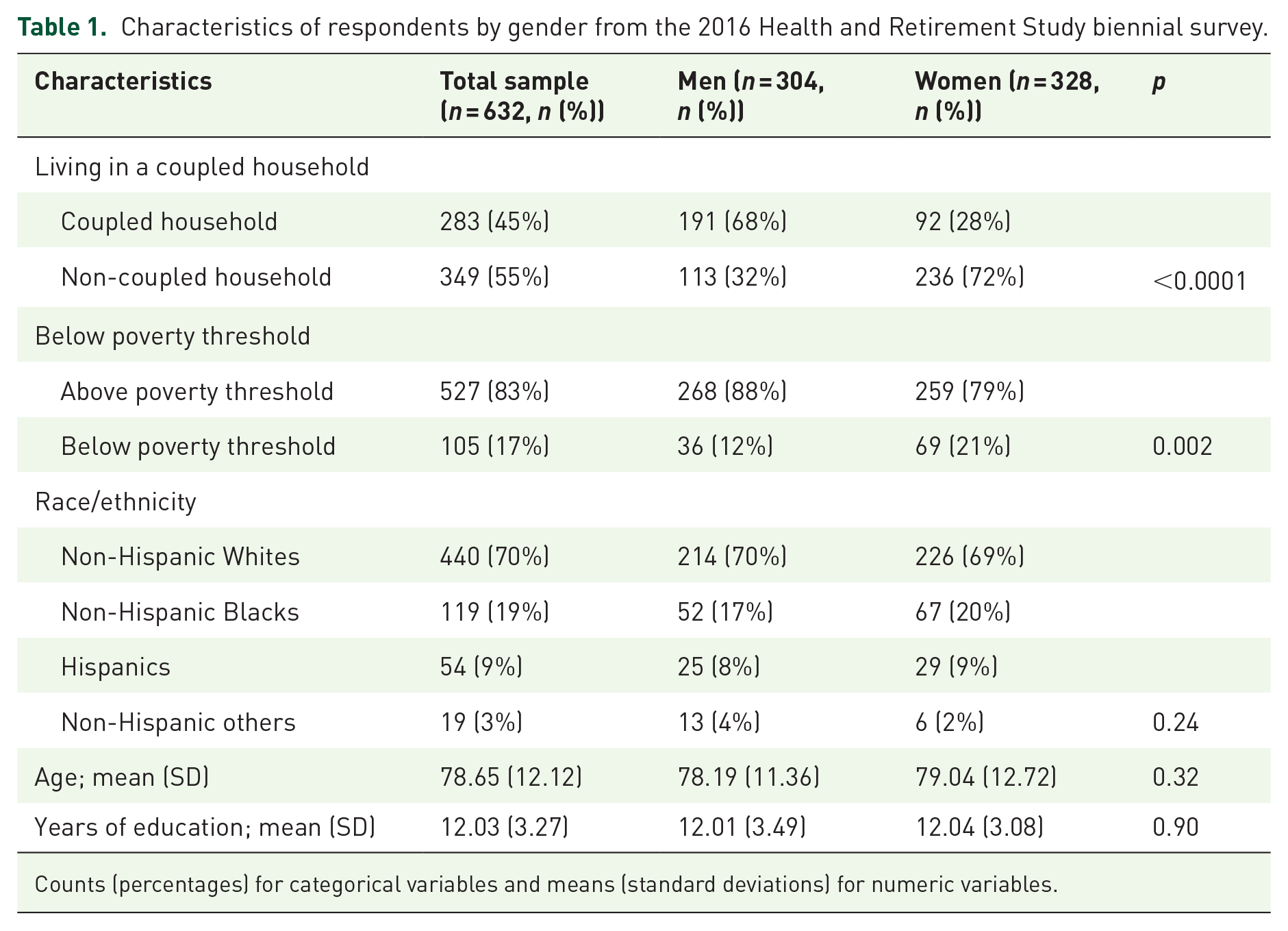
Counts (percentages) for categorical variables and means (standard deviations) for numeric variables.
Although there were no significant gender differences in having written instructions (see Table 2), women were more likely than men to have designated a DPOAHC (70% vs 60%, p = 0.007) and to have discussed their wishes for care with a family member (66% vs 57%, p = 0.02). When examining those in a coupled household, there were no significant differences in having written instructions nor in discussing ACP wishes. In contrast, respondents living in a non-coupled household were significantly more likely to have designated a DPOAHC compared to those living in a coupled household (69% vs 60%, p = 0.01).
Bivariate relationships between gender, couple status and frequency reporting written advance care planning (ACP) instructions, durable power of attorney for healthcare (DPOAHC), and ACP discussions with family members or others (n = 632).
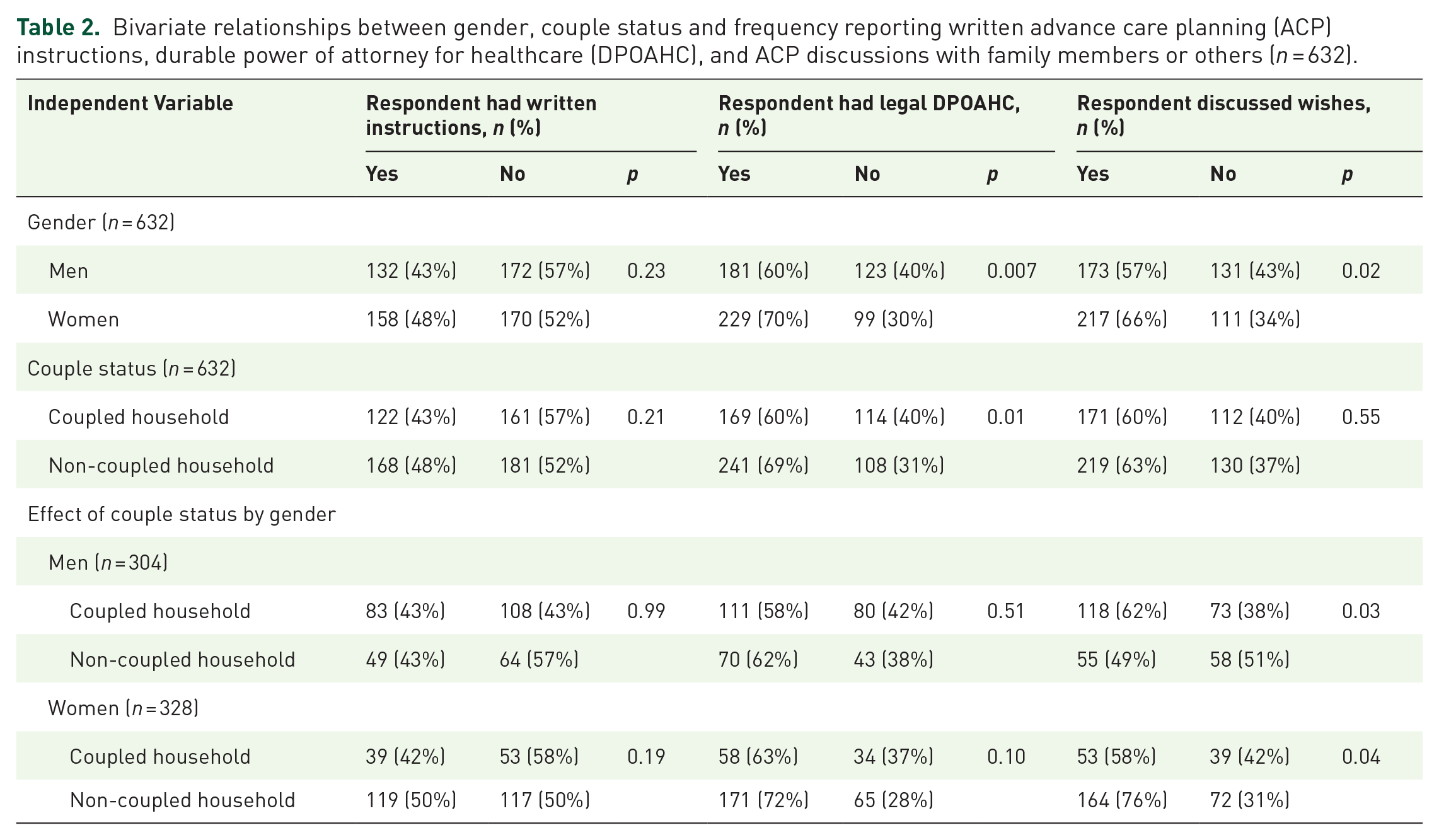
The only interaction between gender and couple status was for discussing one’s wishes. Men living in coupled households were more likely to discuss their wishes than men living in non-coupled households (62% vs 49%, p = 0.03). The opposite was true for women: women living in a non-coupled household were more likely than women living in a coupled household to discuss their wishes with family or others (76% vs 58%, p = 0.04).
To test this moderating effect, mixed models were performed while adjusting for other demographic variables (see Table 3). The models supported the bivariate findings; women were more likely than men to designate a DPOAHC (estimate = 0.52, standard error = 0.20, p = 0.008) and discuss their wishes with others (estimate = 0.49, standard error = 0.18, p = 0.008). There were no statistically significant differences in ACP practices between those living in a coupled versus a non-coupled household when adjusting for gender and other demographic variables.
Multivariate models of the impact of gender and couple status on three types of advance care planning (N = 632).
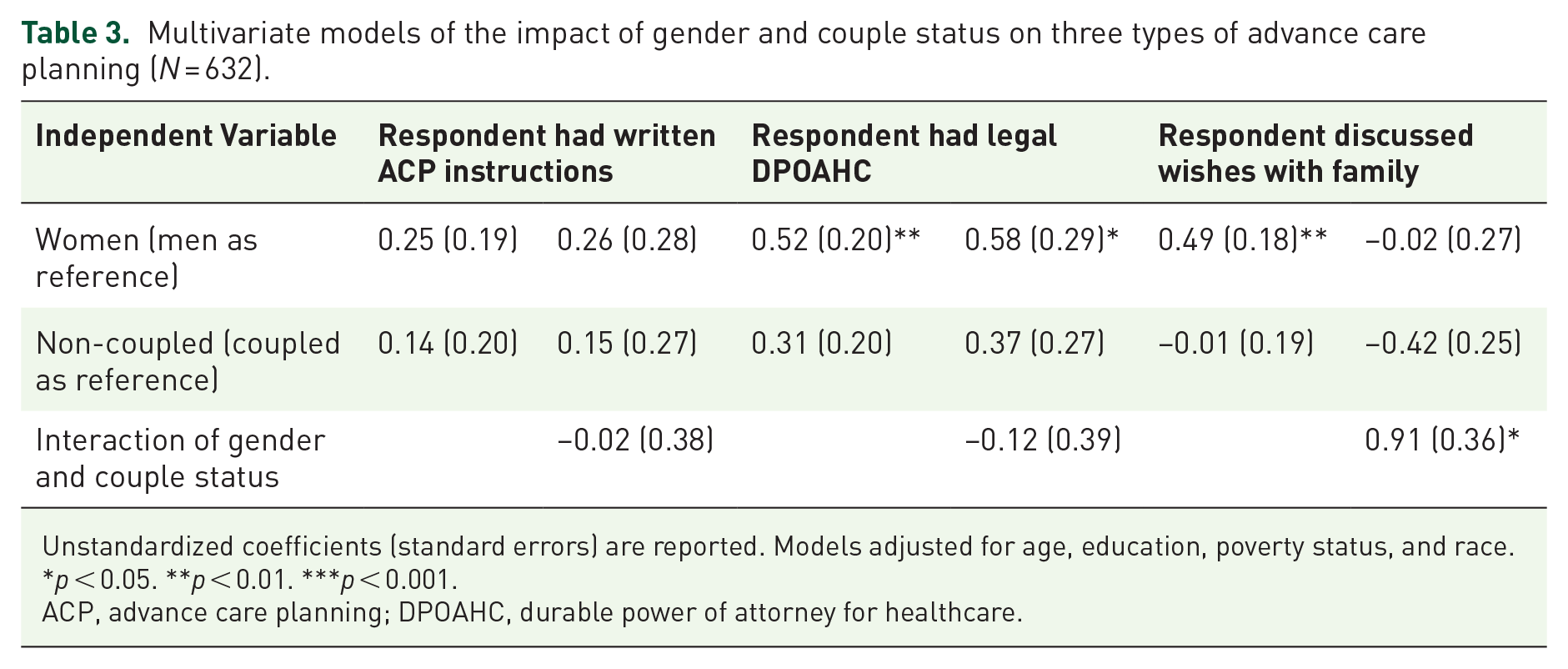
Unstandardized coefficients (standard errors) are reported. Models adjusted for age, education, poverty status, and race.
p < 0.05. **p < 0.01. ***p < 0.001.
ACP, advance care planning; DPOAHC, durable power of attorney for healthcare.
In the models including an interaction term for gender and couple status, the interactions were nonsignificant in predicting ACP written instructions or designating a DPOAHC. However, women in a non-coupled household were significantly more likely than the other three groups to discuss their ACP wishes with family members or others (estimate = 0.91, standard error = 0.36, p = 0.012).
Discussion
In this study of ACP practices, we found that gender and couple status are key demographic factors that contribute to the type of ACP in which people engage. Specifically, women are more likely than men to designate a DPOAHC and to discuss their wishes with others, but not more likely to complete an AD. This was particularly true for women in non-coupled households. Women living without a partner were more likely than any other group to discuss their wishes with family or others. Our results support Cooney et al.’s 12 finding that married women were less likely than their unmarried counterparts to engage in ACP and that married men engaged in more ACP than unmarried men. Our study extends their findings by formally testing the interaction between gender and couple status. Notably, there was no significant interaction between gender and couple status in predicting having an AD or designating a DPOAHC.
Our findings are also consistent with other literature showing that women are more likely than men to discuss their care preferences.15,23–25,34 Women’s greater role in caregiving for a spouse or parent35,36 and greater healthcare decision-making within families, 20 may motivate them to seek out information and engage in ACP. Because women live longer than men and are often caregivers for spouses and parents, they may have experienced more end-of-life decision-making, both with and without ACP tools.13,35,37,38
Women who outlive their spouses or have been without a partner throughout most of their adult lives have different social support systems than married women 39 and may be more aware of possible health outcomes and feel greater vulnerability, leading to greater use of ACP practices. It is also possible that women who are not in a couple relationship may feel more empowered or independent in their decision-making without the traditional societal and cultural expectations for decision-making within a heterosexual relationship. 40 The benefits and drawbacks of living without a partner need further exploration.
Limitations and strengths
This study was limited by a dichotomous measure of gender in the HRS data. Future research should explore how evolving definitions of gender identity, including nonbinary and transgender categories, may impact ACP practices. Similarly, more nuanced measures of the nature and type of couple, one’s history of couple status, and experiences with health events and caregiving would provide a deeper understanding of ACP differences based on couple status. 12 Although past studies have generally shown a positive impact of marriage on health and well-being, 41 the studies have not focused on their impact on healthcare decision-making at the end-of-life. Other limitations include the use of survey data that is susceptible to respondents giving socially desirable answers and the use of exit data provided by a proxy informant who may not have been fully aware of the decedent’s actual wishes and end-of-life care completion.
This study is also limited as data were drawn from those living in the United States where ACP is more prevalent than other parts of the world. 7 Geographic differences based on care access, legislation, and ACP knowledge are vastly different across the world. The generalizability of this study is limited to older adults in the United States willing to participate in a longitudinal study and not in a nursing home in 2016. In order to include poverty status as a control variable, we were unable to include those living in a nursing home.
Previous work on ACP and couple status relied on older data such as 2012 HRS Exit data 12 and smaller populations as in the Wisconsin Longitudinal Study exit data in 2004 from individuals graduating high school in 1957. 42 The strengths of the current study include the use of more recent data and the exploration of possible interactions between gender and couple status associated with ACP practices.
Conclusion
The literature has traditionally focused on chronic diseases and health conditions that disproportionately impact women but is often lacking in studies that more generally examine healthcare decision-making, and, more specifically, ACP practices. 43 We have shown that gender and couple status interact with one another to predict who is most likely to engage in ACP practices. Examining women’s roles in healthcare decision-making as it relates to their relationships, changes in their relationship status, and caregiving experiences over their lifespans will help us better understand the healthcare choices women make and who is most likely to engage in ACP practices. In addition, it is critical to consider the shifting and blending of societal gender and couple status roles and how that may alter healthcare decisions in the future.
For healthcare providers, especially within the field of palliative care, it is important to stay current with ACP data and trends and be aware of patients who are most at risk of not engaging fully in ACP such as males living without a partner or coupled females. Intentional time and effort should be made to educate and encourage these patients to explore ACP options. Framing ACP to ensure the patients’ wishes are met when they can no longer voice them, and sharing with them the benefits of ACP may help patients see the value of these practices. Palliative care providers play a crucial role in initiating ACP conversations that patients sometimes are reluctant to start and then ensuring that the care team is aware of the patient’s wishes as they navigate the healthcare system.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524241287221 – Supplemental material for Gender and couple status differences in advance care planning: a cross-sectional study
Supplemental material, sj-docx-1-pcr-10.1177_26323524241287221 for Gender and couple status differences in advance care planning: a cross-sectional study by Kristin R. Baughman, Ruth Ludwick, Ashley Audi and Laura Harlan in Palliative Care and Social Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.