
Abstract
Background:
Symptoms of emotional and physical stress near death may be related to previous experiences of trauma.
Objective:
To investigate current evidence regarding the following: (1) Is previous trauma identified in people who are dying, and if so, how? (2) How is previous trauma associated with the experience of death/dying in people with or without cognitive impairment? and (3) What palliative care interventions are available to people with previous trauma at the end of life?
Design:
This integrative review was conducted per Whittemore and Knafl’s guidelines, which involves a stepped approach, specifically (1) problem identification, (2) literature search, (3) data evaluation, (4) data analysis and (5) presentation.
Methods:
This integrative review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Electronic databases were searched in August 2021 and updated in August 2023. The articles were quality appraised, and narrative data were analysed using Grounded Theory (GT).
Results:
Of 1310 studies screened, 11 met the inclusion criteria (four qualitative and seven quantitative) conducted in Australia, Canada, Japan and the United States; and American studies accounted for 7/11 studies. Eight were focused on war veterans. Descriptive studies accounted for the majority, with only two publications testing interventions. Re-living trauma near death has additional features to a diagnosis of post-traumatic stress disorder alone, such as physical symptoms of uncontrolled, unexplained acute pain and this distress was reported in the last weeks of life.
Conclusion:
This study proposes that re-living trauma near death is a recognisable phenomenon with physical and psychological impacts that can be ameliorated with improved clinical knowledge and appropriate management as a new GT. Further research is needed to enable past trauma identification at the end of life, and trauma-informed safe interventions at the end of life are an urgent need.
Keywords
Introduction
Most people have experienced traumas across their life course, but little is known about how this may affect their experience of dying. Trauma is a psychological response to an incident or series of incidents or set of conditions that are experienced by an individual as physically or emotionally harmful or life-threatening. 1 Experiencing trauma has the potential to cause long-lasting adverse effects on the person’s functioning including mental, physical, social, emotional and spiritual well-being. 1 Causative events may include conflicts and exposure to violence, sexual violence, Adverse Childhood Experiences (ACE), fires, floods and earthquakes.1,2 In a collective summary of WHO World Mental Health Surveys in 24 countries, 70% of respondents reported experiencing trauma, with an average of 3.2 experiences per person. 3 Trauma-informed health care has developed in response to the need to provide safe access to care for trauma survivors that do not re-traumatise them.4–6
Meyerson et al. and Ganzel highlight that it is essential to be aware of the impact that trauma can have on the dying experience as trauma experiences are common and are part of the personal biographies of many people receiving palliative care.4,5 To date, trauma-informed care is not usual practice in palliative care delivery.4,5,7 Dying patients may live and die with increased chronic pain and suffering and may be re-traumatised at the end of life.4,5,8 Early palliative care has been shown to improve quality of life and mood significantly, 9 be associated with less aggressive care at the end of life and increased survival. 9 Currently, there is a gap in knowledge in providing trauma-informed palliative care,4,5,10 and in part, this may be due to a lack of recognition and understanding of dying patients with known or unknown past trauma, including those with previous post-traumatic stress disorder (PTSD).
The experience of trauma during the lifespan can progress to PTSD, a psychological disorder that occurs post-trauma. 2 PTSD can present in the following ways: intrusive symptoms, persistent avoidance, negative changes to cognition and mood, and hyperarousal/hypervigilance.1,2 Life stressors like physical and cognitive decline in older adults can result in PTSD relapse or worsening symptoms, including subjective re-experiencing of trauma.11,12 In other cases, people can experience delayed onset of PTSD and have symptoms for the first time in later life.12,13 Past trauma is also known to be missed or misinterpreted at the end of life, particularly when people are dying with cognitive impairment, delirium, dementia, pain and anxiety.4,5,14,15 Symptoms can represent first-time emergence and re-emergent experiences of trauma.5,7,12,13
Most people who experience trauma do not develop PTSD; pooled global estimates of the lifetime prevalence of PTSD are around 3.6% with a significant inter-country variation. 3 Prevalence rates of PTSD are significantly higher in conflict-affected populations. Pooled estimates in meta-analyses of conflicted-affected populations have been found to range from 15.3% to 30.6%.11,16 Trauma involving interpersonal violence, particularly sexual violence, is highly associated with PTSD development. 2
Trauma exposure adversely and disproportionally affects vulnerable members of society, including women and girls, ethnic minorities, Indigenous peoples, socioeconomically disadvantaged people and those living in areas of conflict.1,2,16,17 Women have twice the lifetime risk of developing PTSD than males, as they have a higher incidence of being victims of violence, sexual abuse and rape. 2 Trauma also has a heightened impact on children with exposure to traumatic events in childhood increasing the lifelong impacts of that and any subsequent trauma. 2 Trauma survivors often live with chronic pain, have a more significant number of medical diagnoses and report more physical and emotional ill-health than those who have not experienced trauma.8,18,19 Despite the commonality of trauma experiences, diagnosing PTSD can be complex when past trauma has not been disclosed or indeed identified. 2
A better understanding of end-of-life experiences for trauma survivors is needed, whether they have been diagnosed with PTSD, have had a history of PTSD or have had no known PTSD diagnosis.4,7,20 Improving our understanding of current experiences and practice is necessary to develop patient-centred trauma-informed care. This end-of-life care needs to be suitable for those diagnosed with PTSD, those undiagnosed who have symptoms of PTSD and those with first-time emergent or re-emergent experiences of trauma.5,7,12,13
Methods
Aim
This integrative review addressed the following research questions: (1) Is previous trauma identified in people who are dying, and if so, how? (2) How is previous trauma associated with the experience of death/dying in people with or without cognitive impairment? and (3) What palliative care interventions are available to people with previous trauma at the end of life?
Design
This integrative review was conducted in accordance with Whittemore and Knafl’s guidelines, 21 which involves a stepped approach specifically (1) problem identification, (2) literature search, (3) data evaluation, (4) data analysis and (5) presentation. 21 A convergent integrative review was appropriate as the outcome measures of the included studies were heterogeneous and included qualitative, quantitative and mixed-methods research studies. 21 A convergent integrated approach critically synthesises all extracted data from quantitative and qualitative studies. 21 For quantitative studies, this involved qualitising the quantitative data to be used in the narrative interpretation.7,22 The review protocol was registered with PROSPERO CRD42021225037 and reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Figure 1). 23

Search outcomes PRISMA. 23
Definition of PTSD
PTSD was the term used to describe trauma responses in most papers. Although some of the papers were conducted using earlier Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) 2 diagnostic criteria, all share the elements of trauma exposure, hyper-regulation, avoidance, mood disturbance and functional impact. Studies were included if they defined PTSD using DSM-IV and DSM-5 Criteria, 2 see Table 1.
Diagnostic and Statistical Manual of Mental Disorders-5 criteria. 7 .

Search methods
Five electronic databases (APA PsycINFO, CINAHL, Medline, ProQuest and Scopus) and the Cochrane trial register, CENTRAL, were last searched in August 2023 using keywords and subject headings to capture the concepts of trauma- and stressor-related disorders, palliative care and dying. The search strategy was inclusive of identifying all relevant studies over the preceding 20 years. An expert medical librarian developed the search strategy. See Supplemental Appendix 1 for the entire record of database searches. Following the search, all studies were imported into Covidence systematic review software for independent screening by the reviewers according to predetermined inclusion/exclusion criteria (Figure 2). 24 Four reviewers screened titles and abstracts, and four reviewers screened the full-text selected studies.

Inclusion and exclusion criteria.
Data extraction
Data extracted from included studies comprised study aims, methods, samples and key findings, which are represented in the article matrix table (Table 2). 25
Article matrix table.
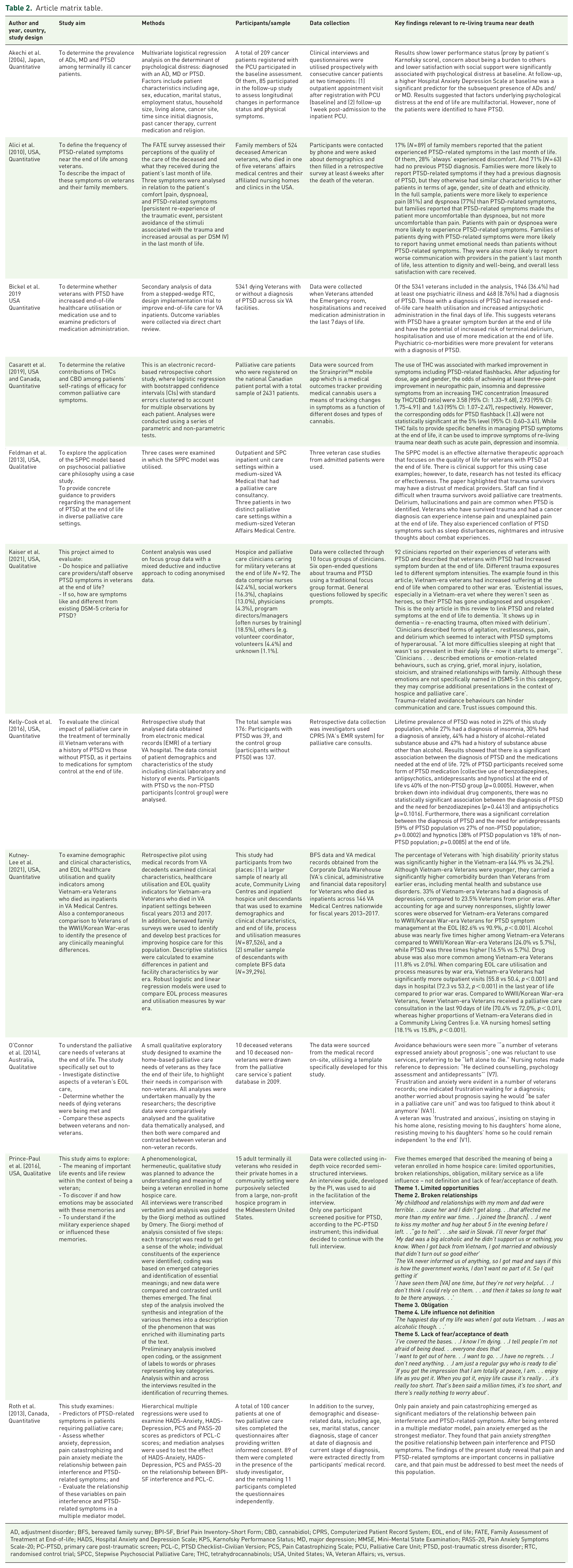
AD, adjustment disorder; BFS, bereaved family survey; BPI-SF, Brief Pain Inventory–Short Form; CBD, cannabidiol; CPRS, Computerized Patient Record System; EOL, end of life; FATE, Family Assessment of Treatment at End-of-life; HADS, Hospital Anxiety and Depression Scale; KPS, Karnofsky Performance Status; MD, major depression; MMSE, Mini-Mental State Examination; PASS-20, Pain Anxiety Symptoms Scale-20; PC-PTSD, primary care post-traumatic screen; PCL-C, PTSD Checklist–Civilian Version; PCS, Pain Catastrophizing Scale; PCU, Palliative Care Unit; PTSD, post-traumatic stress disorder; RTC, randomised control trial; SPCC, Stepwise Psychosocial Palliative Care; THC, tetrahydrocannabinols; USA, United States; VA, Veteran Affairs; vs, versus.
Data analysis
Strauss and Corbin’s approach to coding was used within Grounded Theory (GT) methodology to analyse the narrative data.26,27 Historically, the integrative review method 21 and GT methodology 28 have been used successfully to build nursing knowledge and inform research, practice and policy initiatives. The ATLAs.ti 23 Computor-Aided Qualitative Data Analsis software was used to support data analysis. 27 Three stages of coding were applied, guided by GT methodological traditions. 26 Firstly, open coding was used to fracture the data to distinguish ‘basic conceptual units’ found in the data and organises codes into categories. 29 Once the codes were categorised, axial coding was applied to the data. This step takes the categorised codes and creates a mechanism through which interactions among them can be worked out. 29 Drawing on the data and constant comparison helps ensure the proposed connections demonstrate sustained resonance under interrogation. 29 After axial coding had clarified core categories linked to subcategories, selective coding builds ‘a conceptual framework from which to generate the new GT’ (p. 129) 29 was applied to the data. Networks represented the relationships developed using constant comparison 27 as an essential step demonstrating the transparency of interpretations.
Results
Description of studies
A total of 1581 studies were identified by database searching and exported to Covidence software for removing duplicates (n = 271) and screening (Table 2 – Article matrix table). Around 1176 studies were removed after title and abstract screening due to being out of scope. The full texts of the remaining 136 studies were then screened, and reasons were provided for exclusion. The full-text versions of six publications were not available from any source, including directly from publishers or libraries. As a result, they were excluded. A total of 11 studies were included: four qualitative designs included in-depth interviews, 30 a case study, 31 retrospective data extraction from the clinical record, 32 and an observational study using focus groups and qualitative content analysis. 33 Seven were quantitative in design, including a medical record review,34–37 prospective38,39 and retrospective 40 clinical cohort studies. The studies were conducted in Australia (n = 1), 32 Canada (n = 1), 39 Japan (n = 1) 38 and the United States (n = 7). One study used a medical outcomes tracker and could not provide details of the participant’s country of origin. 40
This review represents 96,505 participants. The sample size varied widely across the studies (from three participants in a case study, 31 to 87,526 in a 5-year study using national hospital datasets). 36 Seven studies included participants with diagnosed PTSD31,33–37,39 and four inferred the existence of PTSD based on responses or clusters of symptoms.30,32,38,40 Of the 11 studies, eight were focused on war veterans, which addressed trauma-informed palliative care for veterans,30–37 pharmaceutical treatment for those with and without PTSD, 40 a comparison of end-of-life care for veterans of the Vietnam War and World War 1/Korean War34,36 and veterans descendants, including bereaved family’s perceptions. 37 One study explored clinicians’ perceptions of end-of-life care for veterans. 33 Three studies were not focused on veterans; one study investigated the self-reported impact of medicinal cannabis on palliative care symptoms, including PTSD-related intrusive symptoms such as flashbacks, 40 one examined psychological distress among cancer patients, 38 and the third explored the relationship between pain and PTSD symptoms in palliative care. 39 Only two studies explored interventions.31,40 Feldman et al. 31 undertook a case series evaluation of a three-step graded intervention process for a veteran population. Casarett et al. 40 studied the self-reported benefits of medical cannabis for common palliative care symptoms, including flashbacks, pain, insomnia and dyspnoea, in a retrospective analysis of a medical outcome tracker for medicinal cannabis users.
Quality appraisal
The Quality Appraisal for primary studies assessed the risk of bias in the included studies. Overall, the methodological quality of retained studies was fair. Quality appraisal was conducted using the Mixed Methods Appraisal Tool (MMAT) Hong et al. (2018). 25 (Table 3).
Results of Quality Appraisal of primary studies.

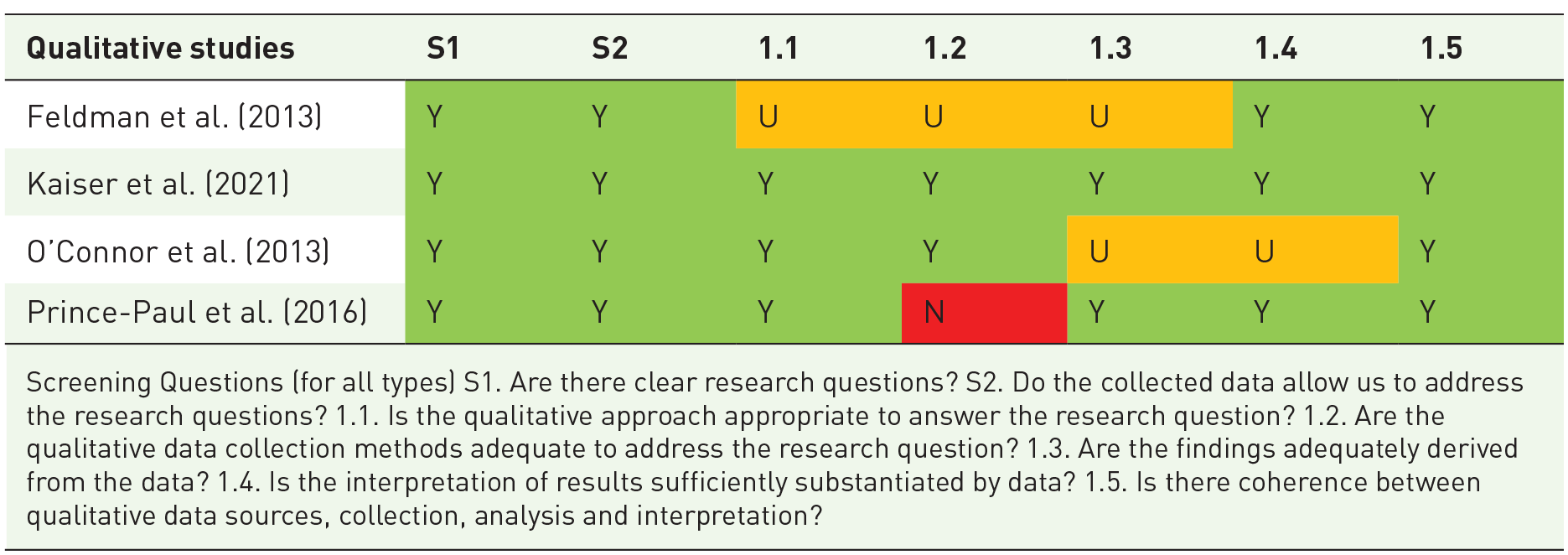
Screening Questions (for all types) S1. Are there clear research questions? S2. Do the collected data allow us to address the research questions? 1.1. Is the qualitative approach appropriate to answer the research question? 1.2. Are the qualitative data collection methods adequate to address the research question? 1.3. Are the findings adequately derived from the data? 1.4. Is the interpretation of results sufficiently substantiated by data? 1.5. Is there coherence between qualitative data sources, collection, analysis and interpretation?

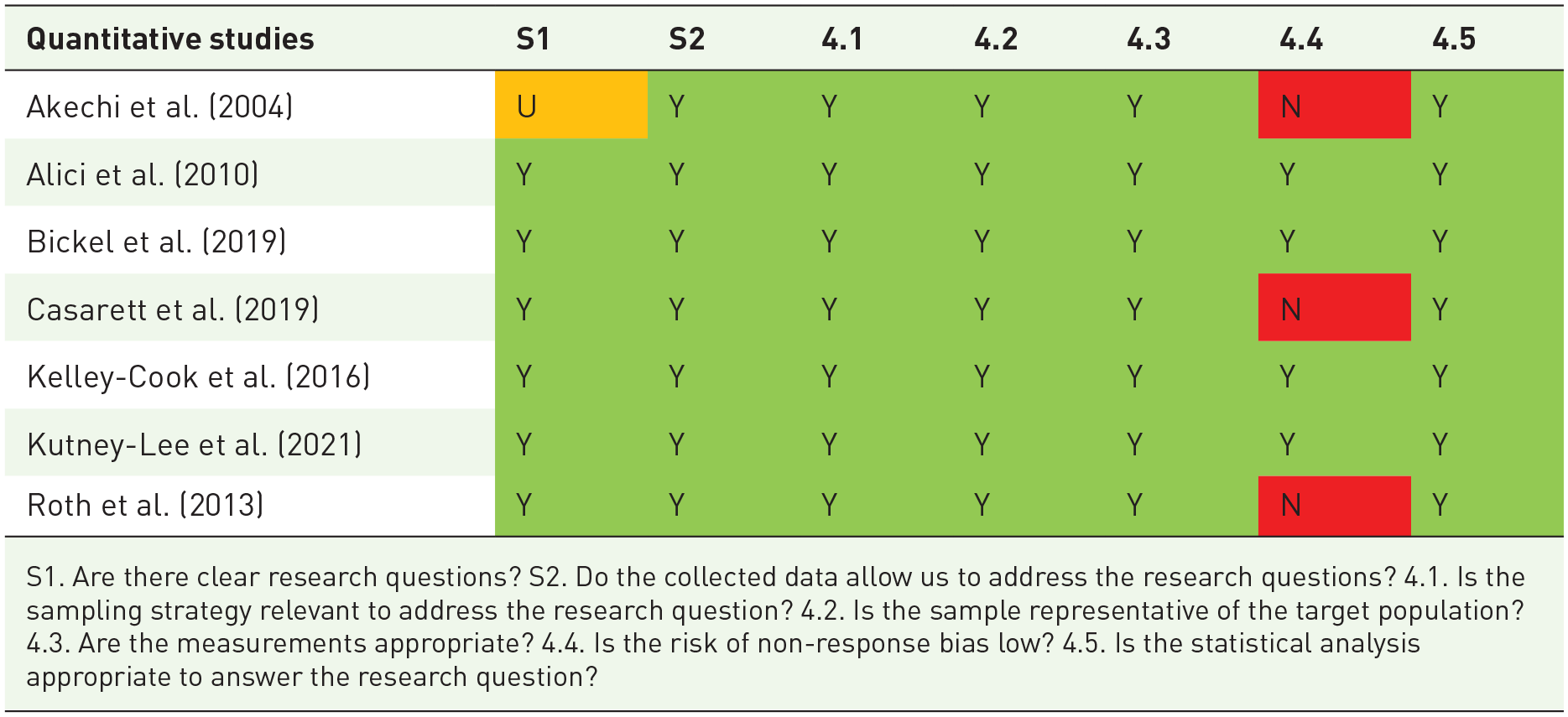
S1. Are there clear research questions? S2. Do the collected data allow us to address the research questions? 4.1. Is the sampling strategy relevant to address the research question? 4.2. Is the sample representative of the target population? 4.3. Are the measurements appropriate? 4.4. Is the risk of non-response bias low? 4.5. Is the statistical analysis appropriate to answer the research question?


Three levels of assessment quality scores


Narrative results
The GT developed from this review is as follows: Re-living trauma near death is a recognisable phenomenon with additional physical and psychological impacts that can be ameliorated with improved clinical knowledge and appropriate management.
This theory is supported by three core categories (Table 4). (1) Additional features help clinicians identify patients who are re-living trauma near death; (2) re-living trauma happens in the last weeks of life and is associated with increased healthcare needs and can include cognitive impairment; and (3) experiences of end-of-life care can be improved for trauma survivors who are re-living trauma near death. Each of the core categories will now be presented, with supporting concepts developed during the data extractions and narrative analysis of the original studies.
Grounded Theory: Re-living trauma near death is a recognisable phenomenon with additional physical and psychological impacts that can be ameliorated with improved clinical knowledge and appropriate management.

PTSD, post-traumatic stress disorder.
Additional features help clinicians identify patients who are re-living trauma near death
This category revealed additional features that were not explained by a diagnosis of PTSD that may assist clinicians in identifying patients who may be re-living trauma near death.30–36,38,39 Re-living trauma near death may represent a specific expression of PTSD-related symptoms, including a combination of specific intrusive symptoms, hyperarousal, avoidance, and negative cognitive and emotional symptoms associated with PTSD. Additional features included increased end-of-life physical symptoms that have a co-relationship with trauma exposure. Included symptoms are unexplained severe pain or dyspnoea, intensification of PTSD-related presentations including avoidance behaviours, negative cognitive symptoms leading to mistrust, hyperarousal and related sleep disorders. These symptoms were described as reflecting a late emergence of trauma symptoms, or an increasing intensity of pre-existing trauma symptoms for the dying person.
Impact on end-of-life physical symptoms
Increased acute pain and dyspnoea
Physical symptoms such as acute pain and dyspnoea are not included in PTSD-related diagnostic criteria but were described as potential features of re-living trauma near death. Three of the included studies provided evidence that re-living trauma near death was associated with increased acute pain.31,37,39 Feldman et al. 31 described a new approach to treatment for individuals with PTSD at the end of life and identified three veterans with a diagnosis of terminal cancer admitted to a palliative care inpatient unit who experienced newly uncontrolled pain. They documented relationships between PTSD-related symptoms and acute pain crises. Emotional and physical pain were connected, with nightmares resulting in worsening pain crises the following morning. 31 Roth et al. 39 found that patients with a terminal cancer diagnosis transitioning to palliative care experienced co-occurrence of physical pain and emotional response to pain including PTSD symptoms. When patients worried about or feared cancer pain, their PTSD-related symptoms were triggered. 39 This interaction of pain symptoms was further emphasised in a separate study of family members’ perceptions of the frequency and impact of PTSD-related symptoms in veterans at end-of-life. 37 They found that pain had a bidirectional relationship with PTSD. Trauma affected the extent of pain reported by patients, and patients with pain experienced more symptoms of PTSD than those without pain. 37
Alici et al. 37 found that increased distress with dyspnoea was an additional feature of re-living trauma near death. There was also a bidirectional relationship between dyspnoea and PTSD-related symptoms. 37 Dyspnoea increased PTSD symptoms such as anxiety, and these symptoms adversely affected dyspnoea. This observation was a significant finding, as dyspnoea, along with pain, are symptoms that can cause high levels of distress for those dying. 37 Although PTSD-related symptoms were common at the end of life, family members reported that pain and dyspnoea occurred more frequently, 37 though, in comparison with PTSD symptoms, the pain was more likely to be rated as having a more significant impact than dyspnoea symptoms.
Intensification of PTSD-related symptoms and disorders
PTSD-related features of intrusive symptoms, persistent avoidance, negative alterations in cognition and mood, and alterations in arousal and reactivity were intensified when re-living trauma near death. 33 The presence of other factors such as substance use disorders, mood, anxiety disorders, risky behaviours and self-harm increased PTSD symptoms for trauma survivors. 33
Persistent avoidance, resistance to care and mistrust of authority
Mistrust of others is not included in the PTSD diagnostic criteria; however, it is a feature of re-living trauma near death. Four of the included studies31–33,39 showed evidence of avoidance behaviour that reduced access to palliative care at end-of-life. In an Australian retrospective study, O’Connor et al. 32 compared the home-based palliative care needs of 10 veterans to 10 non-veterans facing dying and found that some veterans avoided conversations with clinicians. 32 Two male veterans were reluctant to engage with services and avoided interventions like counselling, psychosocial assessment and antidepressant medication. 32 One veteran was unwilling to access services and expressed a wish to be ‘left alone to die’ (p. 138). 32 Similarly, Roth et al. 39 found that when PTSD-related symptoms were triggered by cancer pain, avoidance behaviours and psychological symptoms increased. Kaiser et al. 33 found that resistance to care was a feature of re-living trauma near death and was common in dying veterans. In their case studies evaluating the Stepwise Psychosocial Palliative Care (SPPC) model, Feldman et al. 31 found that one veteran with terminal cancer ‘coped with stressful topics by avoiding them’ (p. 240). Feldman et al. 31 also found that clinicians in the palliative care inpatient unit found it challenging to accept when patients declined medical care. Staff experienced emotional reactions like anger and frustration when a 65-year-old veteran with lung cancer refused all future care, including palliative care. 31 Notably, the male veteran previously referred to had not disclosed his history of trauma. When he refused care, including palliative care, the psychologist did a chart audit of his medical record, and a history of PTSD was identified. 31 This then initiated the trauma-informed palliative care SPPC model, which improved his symptom management.
Three of the included studies provided evidence of mistrust of medical providers and authority.30,31,33 Kaiser et al. 33 and Feldman et al. 31 found that palliative care clinicians perceived that trust issues impeded veterans’ engagement. Several interviewees in the study by Prince-Paul et al. 30 emphasised their mistrust and experience of unfulfilled promises by the United States Department of Veterans Affairs. O’Connor et al. 32 found that frustration and anxiety were evident in the records of several deceased Australian veterans. One veteran worried about his prognosis and stated that he would feel safer in an inpatient palliative care unit and that he did not have the energy to think about it anymore. 32
On occasion, some patients addressed trauma through increased engagement. Kaiser et al. 33 found that some clinicians reported the opposite of avoidance, describing veterans as being eager to share stories about medals and certificates and connect with others from the military. Other American war veterans chose to be cared for in the hospice programme as they felt the comradery and increased dignity of dying with their fellow servicemen. Others were proud of being veterans and liked to talk about their experiences. 33
Intrusive symptoms and alterations in arousal and reactivity
Four studies30,31,33,35 found that participants experienced increased sleep disturbance and increased psychological distress. Prince-Paul et al. 30 found exposure to ACE was associated with an increased risk of further trauma exposure later in life. In their study of the views of clinicians, Kaiser et al. 33 noted that some dying veterans had additional trauma-related presentations that aligned with traditional PTSD symptom clusters. Moral injury, family avoidance with or without fractured relationships, and isolation aligned with negative alterations in cognition and mood, pain, agitation, restlessness, cognitive issues and risky behaviours aligned with hyperarousal. 33
A retrospective study authored by Kelley-Cook et al. 34 compared the use of benzodiazepines, hypnotics, antidepressants and antipsychotic medications for terminally ill veterans with a history of PTSD (n = 28) to those without PTSD (n = 55). PTSD-related symptoms were often associated with a history of insomnia and other sleep disturbances such as obstructive sleep apnoea and restless leg syndrome. 34 In their national study of health care utilisation and medication use at the end of life, Bickel et al. 35 found that veterans with PTSD, compared to veterans without PTSD, were more likely to be prescribed antipsychotic medication, potentially increasing their risk of terminal delirium.
Re-living trauma near death can coexist with dementia and cognitive impairment
Two of the included studies described links between re-living trauma near death and cognitive impairment. Kaiser et al. 33 found a link between re-living trauma near death and dementia. Clinicians in this study reported observations in people who had dementia or cognitive impairment at the end of life that are consistent with re-living traumatic events. 33 Re-experiencing trauma can co-occur with dementia and delirium. 33 Palliative care clinicians included in focus groups described forms of agitation, restlessness and delirium, which were thought to be hyperarousal symptoms of PTSD. 33 There can be an iatrogenic relationship between re-living trauma and cognitive and perceptual impairment. 31 Feldman et al. 31 described the case of one veteran who experienced end-of-life hallucinations that were caused by a combination of antipsychotics and pain relief.
Related conditions, including substance use disorder
Co-morbid psychiatric disorders and substance use disorders were described in the reviewed research. In a study of 5341 veterans receiving end-of-life care in US-based Veteran Administration hospitals, 36.5% of veterans with PTSD also had anxiety disorders, compared to 12.5% without diagnosed PTSD; 21.4% of veterans with PTSD and 4.8% of those without PTSD had major depressive disorder. 35 Substance use disorder is not included in the DSM-5 criteria for the diagnosis of PTSD. 2 The clinicians in the study by Kaiser et al. 33 cited substance use disorder as a potential additional presentation for dying veterans who are trauma survivors. In Bickel et al.’s 35 national study, alcohol abuse was reported among 10.7% of veterans with PTSD and 3.4% of those without PTSD; 11.8% had a drug-use disorder (excluding nicotine and alcohol) compared with 2.9% of veterans without PTSD. In their pilot study, Kelley-Cook et al. 34 compared terminally ill Vietnam veterans with or without PTSD at the end of life and found that 44% of veterans with a history of PTSD had a history of alcohol-related substance abuse, and 47% had a history of substance abuse other than alcohol.
Kelly-Cook et al. 34 proposed that medication use for people with PTSD is likely to differ from those without PTSD, reflecting their greater vulnerability to re-experiencing and other PTSD symptoms. Kutney-Lee et al. 36 studied terminally ill Vietnam veterans and compared them to dying veterans from World War 2 and the Korean War campaigns and found that alcohol abuse rates among Vietnam-era veterans were five times that of other veterans.
In the interview study by Prince-Paul et al., 30 one veteran at the end of life commented that he tried to heal past transgressions by attending Alcoholics Anonymous. Another talked about being an alcoholic when he returned from the Vietnam War. 30
Re-living trauma near death requires increased healthcare utilisation
Increased healthcare utilisation and medications in the last weeks of life
Two of the included studies34,35 found that patients re-living trauma near death had increased health care utilisation and use of end-of-life medication in the last days/weeks of life. When comparing Vietnam veterans with or without PTSD, Kelley-Cook et al. 34 found that veterans with PTSD were more likely to attend outpatient mental health services. They also found that there was a significant association between a diagnosis of PTSD and increased use of antidepressants and hypnotic medication at the end of life. 34 Bickel et al. 35 found that American veterans with PTSD did have increased healthcare utilisation and medication use in the final 12 months of life. Healthcare use included significantly more United States Department of Veterans Affairs hospital admissions and emergency room visits, longer stays and an increased use of invasive treatments. 35 The latter may have reflected the fact that the cohort with PTSD was younger than the cohort without PTSD (mean age 65.4 and 70.1 years, respectively). 35 Significantly, the cohort with PTSD also received increased symptom-relieving opioids, benzodiazepines and antipsychotic medications within the last 48 h and the last 7 days of life. This suggests that trauma survivors have increased symptoms and suffering at the end of life and thus require more medication to manage these symptoms. 35
In the included studies, there was evidence of symptoms increasing for people who were re-living trauma near death. Alici et al. 37 found that family members reported observing symptoms of PTSD and pain in the last months of life. Furthermore, they discovered that in the last month of life, these descriptions of re-living trauma seemed to be associated with decreased comfort. 37 O’Connor et al., 32 who compared veterans to non-veterans and their health utilisation at the end of life, found that rates of hospitalisation varied among the 20 participants. Veterans, however, had more hospital admissions and had more significant contact with health professionals than their non-veteran counterparts. 32
Experiences of end-of-life care can be improved for trauma survivors who are re-living trauma near death
Five of the included studies provide evidence that trauma survivors and their families have unmet needs at the end of life.31,33,35,37,38 Alici et al. 37 found that family members were more likely to have unmet needs when their loved one was a veteran with PTSD. Family members reported that the clinician’s communication was poorer and that they paid less attention to the patient’s dignity. Family members also described ‘less satisfaction’ with their overall care delivery. Kaiser et al. 33 found that clinicians observed unmet needs from family members caring for veterans at the end of life and recommended education about PTSD at the end of life for families, providers and veterans. 33
Akechi et al. 38 found that none of the patients were referred to a psychiatrist during the study period despite 16.3% of participants having an adjustment disorder at baseline, highlighting this as an unmet need. Feldman et al. 31 found that palliative care staff had unmet educational needs as they were uncertain how to communicate with patients who refused care, including palliative care. Kaiser et al. 33 found that clinicians wanted more education and resources to understand PTSD at the end of life better. Clinicians wanted to learn how to identify past trauma, improve assessment skills, communication skills, symptom management and support family members. 33
Enablers of better end-of-life care for trauma survivors
Receiving palliative care
Palliative care seemed to be effective when it was available and provided.31,37 Feldman et al. 31 and Alici et al. 37 both reported the benefit of clinical palliative care services for dying veterans with PTSD. Alici et al. 37 surveyed family members of veterans who had died in a United States Department of Veterans Affairs hospital; family members of people with PTSD symptoms reported that those who had received a palliative care consult had lower ratings of discomfort due to PTSD-related symptoms.
Four included studies31,33,37,40 suggested further benefits of trauma-informed palliative care. Kaiser et al. 33 found that some clinicians expressed interest in learning more about trauma and its effects on dying veterans. In the same study, hospice and palliative care clinicians spoke about the importance of identifying past trauma and suggested universal screening be used to increase the chance of identification. 33 Alici et al. 37 found that family members identified PTSD-related symptoms more quickly if a diagnosis of PTSD had been made. However, since 63 of the 89 patients observed to have PTSD-related symptoms did not have a previous PTSD diagnosis, family members were sometimes left having to puzzle out symptoms without a frame for understanding them. 37
Benefit of medications for symptom management
There was a lack of evidence of specific pharmacotherapies that could support trauma survivors as they die, and all studies were observational. The only medication studied in relation to PTSD-related flashbacks at the end of life was cannabis. Using an internationally used self-report app connected to a portal, Casarett et al. 40 explored the relative contribution of tetrahydrocannabinol (THC) and cannabidiol (CBD) to patients’ self-rating of efficacy for common palliative care symptoms. They chose to look at common palliative care symptoms such as neuropathic pain, anorexia, anxiety symptoms, depression symptoms, insomnia and PTSD-related flashbacks. 40 Higher doses of THC, relative to CBD, were associated with a marked improvement in symptoms, including PTSD-related flashbacks. 40 The findings from this study have increased relevance to this review as both increased pain31,37,39 and sleep disturbances31,33,34 have been identified as additional features of re-living trauma near death, both of which cannabis was effective in managing. 40
Application of the SPCC model
There was a notable lack of palliative care interventions for those who are re-living trauma near death. Only one specific palliative care intervention for trauma survivors was identified. Feldman et al. 31 derived case-study-informed evidence that supports the pilot of the SPPC model. 31 This model reportedly improves access to effective palliative care for dying veterans with PTSD. Feldman’s model of care is based on palliative care philosophy and recognises that assessing for trauma can re-traumatise, so the first two steps are trauma sensitive rather than directly trauma treating. 31 The model has three stages or steps. Stage 1 ‘Palliate Immediate Discomfort and Provide Social Supports’. If this is ineffective, the clinicians must progress to Stage 2, ‘Provide Psychoeducation and Enhance Coping Skills’. If this stage is ineffective, clinicians progress to Stage 3, ‘Treat Specific Trauma Issues’. 31 In the case studies used to explore this model, environmental changes could reduce the triggering of PTSD-related symptoms. 31 One Veteran’s PTSD-related symptoms were triggered by traffic noise. His TV was always left on to combat this, and his door was shut. 31
Discussion
This study reveals new synthesised knowledge regarding the identification of trauma experiences near death. Findings should be interpreted with caution, as only 11 studies met the inclusion criteria. This review has highlighted that re-living trauma near death is a recognisable phenomenon with physical and psychological impacts30–40 that can be ameliorated with improved clinician knowledge30,33–37,39 and appropriate management.30,31,33–37,40 Additional features that are not included in a diagnosis of PTSD, such as intense unexplained acute pain,31,37,39 can help clinicians identify patients who are re-living trauma near death. These additional features that can occur in the last weeks of life are associated with increased healthcare utilisation and increased use of end-of-life medications and may coexist with cognitive and perceptual impairment.33–37 Additional features also include refusing all care, including palliative care, as an avoidance and mistrust response and staff-splitting behaviours.5,31
The positive interventions highlighted that stepwise communication was effective when trauma survivors had limited time to live, were fatigued or were unwilling to engage in trauma therapy, but this was a single case study with only three participants. 31 Elsewhere, Meyerson et al. 5 discussed trauma-informed care approaches in palliative care settings again for dying patients who were too fatigued or unwilling to engage in trauma therapy at this time in their lives. Meyerson et al. 5 provide examples of how trauma-informed hospice and palliative care can ameliorate distress and PTSD symptoms at the end of life. They provide recommendations for all palliative care teams on how to elicit and respond to a history of trauma. 5 If palliative care teams are not aware of a history of trauma, they may not pick up on contextual cues, and appropriate referrals may not be made, resulting in increased suffering and a delay in both curative treatment and palliative care. 5
To date, trauma-informed care is not the usual practice in palliative care delivery.4,5,7,10 Timely palliative care has been shown to improve quality of life and mood significantly 9 ; patients experience less aggressive care at the end of life and survive longer. 9 Yet, dying patients who have experienced trauma may live and die with increased chronic pain, severe unexplained acute pain and increased suffering and may be re-traumatised at the end of life.4,5,8,31,37,39 As has been discussed, the use of palliative care in general seems helpful for people re-living trauma at the end of life, as specific approaches show promise. Stepwise communication was effective when trauma survivors had limited time to live, were fatigued or were unwilling to engage in trauma therapy, but this was a single case study with only three participants. 31
Multiple knowledge gaps impede clinical responses to the challenge of care provision for people re-living trauma at the end of life. Clinicians are not adequately trained in how to provide trauma-informed palliative care. 10 There is also a lack of awareness of the commonality of trauma experiences and PTSD in dying patients.4,5,20 Lastly, there is incomplete knowledge of the significant impact that trauma has on dying experiences.4,5 These issues likely exacerbate palliative care teams not adequately seeking a history of trauma in their patients, missing contextual cues and opportunities for appropriate referrals, and resulting in increased suffering and delays in care-focused responses to these issues. 5 A lack of awareness, screening tools, trauma-informed practices and related specific educational interventions contribute to the unmet needs in clinical practice for this high-risk patient group.14,20
Our review highlights other significant gaps in the literature regarding re-living trauma near death in relation to specific populations and essential outcomes. Current published research concentrates on trauma-affected North American male war veterans.30,31,33–37 Studies including women and girls, who are twice as likely to have a history of trauma, are urgently needed.1,2 Indigenous populations, including those from Australia, are often trauma survivors and at risk of developing multiple related co-morbidities.2,17,41–46 These issues, and the pervasive inequity of care provision that many minority groups face, compound the challenges of understanding and meeting needs relating to trauma experiences at the end of life.2,17,41–46 Additionally, the impact of trauma causes other than war and combat requires attention. 2 There is also a lack of understanding about predictive risk factors for re-living trauma near death: for example, are certain types of trauma experiences associated with increased risk of re-living trauma near death? Does a diagnosis of PTSD during the life course increase the risk of re-living trauma near death? Does psychological therapy for PTSD decrease risks, and does a dementia diagnosis increase your chance of re-living trauma near death?
This review also demonstrates the challenges of understanding and responding to trauma experiences at the end of life when these experiences are complicated by other co-morbid conditions. The impacts of ageing and disability on trauma experiences at the end of life are poorly understood. Ageing and its predictable association with reduced mobility and increased disability can decrease a sense of control and increase stress for older people who are trauma survivors. 14 Reduced mobility and increased disability can also lead to feelings of vulnerability that lead to re-emergence or exacerbation of PTSD symptoms. 5 Cognitive impairments such as delirium, and dementia or even the heightened distress of physical pain at the end of life may also lead to mental health issues, including PTSD being overlooked or under-appreciated. 14 In 2021, the leading cause of death for Australian adult females was dementia. 46 However, people with dementia and cognitive impairment continue to be under-represented in end-of-life care research and the receipt of specialist palliative care.30,38,39,47–50 The link between trauma and the development of cognitive impairment like dementia highlights the urgent need to understand better the coexistence of these issues near dying.43,45 The more intense trauma experienced, the greater the risk of developing dementia later in life.4,43,45 Whether this relationship also affects the risks of re-living trauma near death remains unknown. As noted by Kaiser et al., 33 re-living trauma near death can coexist with dementia and/or delirium. The typical exclusion of people with cognitive impairment from end-of-life research needs to be urgently redressed to better understand the impacts of the emerging links between these issues in this vulnerable population, and determine the most appropriate clinical responses to their needs.
Implications for research
Firstly, there is an urgent need to fill research gaps, including how to identify re-living trauma near death for those with or without cognitive impairment. Currently, a validated tool has not been developed and tested for assessing trauma history for patients at the end of life.4,5,37 Secondly, there is an urgent need to fill education and knowledge gaps for clinicians to provide evidence-based trauma-informed practice to support trauma survivors as they die. Prospective studies are needed in the last weeks of life to capture re-living trauma near death.
Implications for practice
This review highlighted that a range of presentations, in conjunction with a known or suspected history of trauma, can be interpreted as ‘trauma cues’ as a constructive clinical activity to better meet patient needs by identifying re-living trauma near death. The ‘trauma cues’ identified in this review include acute severe unexplained pain and dyspnoea.31,39
Limitations of articles included in the review
The research followed a clear and transparent review process, but there are several limitations to point out. Only 11 studies met the inclusion criteria for this review, which identifies that this is an emerging focus for clinicians and researchers. The study designs were heterogeneous, qualitative and quantitative, with participant numbers ranging from 3 to 8752. Findings should be interpreted with caution as only 5/11 had a low risk of bias,33–37 and the majority of participants were war veterans (8/11)30–37 mostly from North America (7/11).30,31,33–37 All 11 studies used PTSD either directly (7/11)31,33–37,39 or indirectly (4/11).30,32,38,40 Only two were intervention studies (graded communication and medical cannabis).31,40
Paradigmatic factors confound attempts to draw coherent conclusions. Most of the studies were conducted in America, and subjects were mostly male military veterans; therefore, possible cultural differences may not be evident. In this review, prospective studies excluded participants with cognitive impairment. None of the studies addressed the experiences of people who did not speak the country’s majority language.
The studies draw strongly on record reviews in veteran hospitals. Most of the studies were descriptive, and few engaged with the experiences of consumers; few interviewed persons dying or undertook case or ethnographic analyses of dying people. As most of the studies were of veterans, most were of older men. Few studies explored interventions.
Conclusion
The findings suggest that re-living trauma near death has additional features that a diagnosis of PTSD cannot explain. These additional features include physical symptoms of severe unexplained pain and dyspnoea, exacerbation of PTSD symptoms even in the absence of a prior PTSD diagnosis, and this happens in the last weeks of life. Further examination that can apprise past trauma identification and trauma-informed interventions is urgently needed to reduce suffering at the end of life for trauma survivors. This examination needs to include participants from all trauma types, including participants with cognitive impairment and women.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524241277851 – Supplemental material for Re-living trauma near death: an integrative review using Grounded Theory narrative analysis
Supplemental material, sj-docx-1-pcr-10.1177_26323524241277851 for Re-living trauma near death: an integrative review using Grounded Theory narrative analysis by Nikki Johnston, Michael Chapman, Jo Gibson, Catherine Paterson, Murray Turner, Karen Strickland, Wai-Man Liu, Christine Phillips and Kasia Bail in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524241277851 – Supplemental material for Re-living trauma near death: an integrative review using Grounded Theory narrative analysis
Supplemental material, sj-docx-2-pcr-10.1177_26323524241277851 for Re-living trauma near death: an integrative review using Grounded Theory narrative analysis by Nikki Johnston, Michael Chapman, Jo Gibson, Catherine Paterson, Murray Turner, Karen Strickland, Wai-Man Liu, Christine Phillips and Kasia Bail in Palliative Care and Social Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.