
Abstract
Background:
Caring for a family member can be demanding, particularly when caregivers experience profound distress. Supportive interventions may help prevent mental and physical illness in the caregiver. General practice plays a key role by regularly engaging with patients and caregivers, thereby being able to identify their support needs, offer talk therapy and refer to care initiatives.
Objective:
This study aimed to develop and pilot-test the Caregiver Care Model to mitigate grief reactions among caregivers in general practice.
Design:
A participatory intervention development study.
Methods:
A prototype was developed in a workshop with healthcare professionals. The prototype was refined based on a pilot-test among 40 caregivers from 5 general practice clinics and a workshop with general practitioners. The data were obtained from workshops, feedback questionnaires completed by healthcare professionals, and interviews with caregivers and general practitioners. The analysis focused on model development and mechanisms of impact.
Results:
The prototype was refined by focusing the dialogue questionnaire, minimising the grief facilitation tools and expanding the target group. The prototype seemed to accommodate the needs among caregivers by acknowledging their situation. The final model includes up to seven caregiver consultations in general practice. A dialogue questionnaire filled in by the caregiver serves as a fixed starting point and preparation for the first consultation. If needed, talk therapy in general practice or referrals to other services are used.
Conclusion:
The model offers promising support for caregivers. Its flexible structure allows for customisation. The viability of the model should be further tested.
Keywords
Background
An increasing number of patients live with severe chronic conditions due to changes in population demography and advances in healthcare. Severe illness will introduce changes in the everyday lives of the patient and the family. This situation may be demanding for family caregivers. Loss of health and daily functions may induce grief symptoms in both the patient and their relatives. Caregiving has negative impact on relatives, including impact on cortisol levels, 1 the immune system 2 and severe distress. 3 Caregivers are at risk of developing grief complications during bereavement such as a depression or a complex grief reaction with persistent severe grief symptoms.4,5 The risk factors for complications include prior mental illness and low education (caregiver-related risk factors) 4 and sudden death or loss of a child (circumstantial risk factors). 5
At the same time, the healthcare system is under pressure, and families are expected to manage the situation in their home as long as possible. Hence, the focus and energy may be on the patient’s symptoms and caregiver tasks, which have been described as ‘chronic homework’. 6 Thus, family caregivers have been shown to have unmet needs for emotional support, disease-specific knowledge, self-care and practical support. 7
General practice holds a key position in providing continuous care. 8 In primary palliative care, the primary care teams have a pivotal role in initiating and providing support for patients and their family caregivers.9,10 Prior studies have found that general practice-based interventions for caregivers to patients diagnosed with dementia can improve their mental health. 11 Additionally, talk therapy in general practice may reduce bereaved caregivers’ risk of psychiatric illness, 12 and caregivers with the highest levels of grief symptoms tend to have more contact with general practice. 13 However, even if general practitioners (GPs) perceive the provision of support for family caregivers as a core task, caregiver support is not offered in a structured way, 14 and there is a knowledge gap regarding clinical assessment and pathways of support for caregivers. 10 Hence, healthcare professionals in general practice may be able to identify family caregivers with support needs, and general practice could be an appropriate setting for targeted interventions.
A structured way of providing caregiver interventions in general practice needs to be developed in the clinical context and with involvement of caregivers and healthcare professionals to increase the usability and support the implementation.15,16 Such interventions may mitigate caregivers’ grief reactions during severe illness of their close relatives.
Therefore, our aim was to develop and pilot-test the Caregiver Care Model to mitigate complex grief reactions among caregivers in general practice.
Method
Study design
This intervention development study is based on a co-production and participatory approach, focusing on development, adaptation and rapid cycles of evaluation based on exchange between researchers and stakeholders.15–17 Caregivers and healthcare professionals participated in the development process, thereby ensuring that the intervention would fit the clinical setting. An implementation-based approach to intervention development was applied to facilitate sustainable adoption and implementation in a ‘real-world’ setting. 18
The development of the Caregiver Care Model was performed in three steps: (1) A workshop with healthcare professionals, (2) pilot testing in general practice clinics and (3) a workshop with GPs from the pilot clinics (Figure 1).
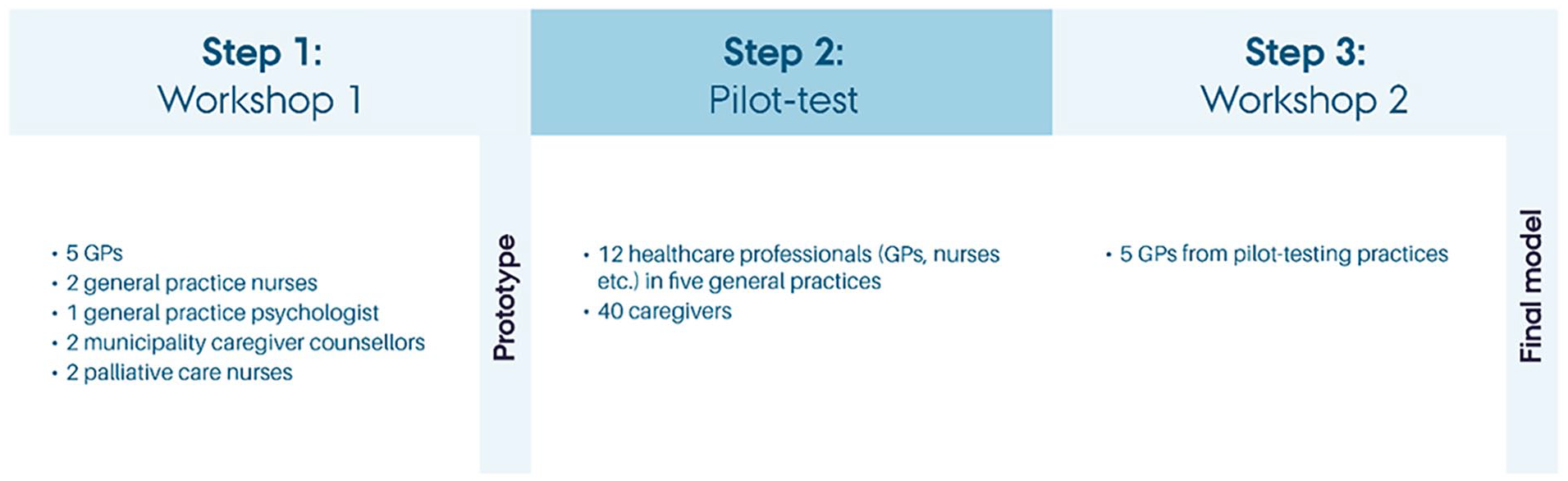
Development steps of the Caregiver Care Model.
The study was reported following the Standards of reporting qualitative research (SRQR) checklist 19 (see Supplemental File 1), the Guidance for reporting intervention development studies in health research (GUIDED) checklist 20 (see Supplemental File 2) and the Template for intervention description and replication (TIDieR) checklist 21 (see Supplemental File 3).
Setting
Danish healthcare is mainly funded by public taxes, and all residents have free-of-charge access to services. 22 The GPs are gatekeepers to the healthcare system. They are self-employed and may organise their own clinic and employ healthcare staff for selected types of clinical work. Based on the contractual agreements between the GPs and the regional authorities, GPs may provide up to seven annual talk therapy consultations to patients with mental health needs. The study is conducted in Central Denmark Region comprising cities as well as more rural areas.
The Caregiver Care Model
The model was intended to mitigate complex grief reactions among caregivers in general practice by assisting healthcare professionals in (1) identifying the caregivers’ needs and risks of complications and (2) if assessed necessary, plan and perform talk therapy to caregivers and/or refer to community-based initiatives or secondary sector. The model prototype included components inspired by (1) a needs- and risk assessment questionnaire to identify caregivers’ support needs and risks of complication developed in specialised palliative care 23 and (2) grief facilitation tools, including elements of grief theory and grief facilitation,24–26 developed from Complicated Grief Therapy (CGT). 27
Participants
In step 1, we recruited 12 healthcare professionals (GPs, general practice nurses, community caregiver counselors and palliative nurses) from the research team’s network to participate in a workshop.
In step 2, the preliminary model was tested among five general practice clinics. These clinics constitute a formal network in the Central Denmark Region, consisting of general practice clinics dedicated to quality development. We included 40 caregivers in the pilot testing. Inclusion criteria included being 18+ years of age and being a caregiver for a person with serious illness. Five of the caregivers participated in a semistructured interview. An overview of the participants from step 2 is presented in Table 1.
Overview of participants in step 2.

GP, general practitioner.
In step 3, one GP from each of the five pilot clinics participated in a final workshop.
Data collection
The workshop in step 1 was conducted on 1 December 2021. The participants were guided through a co-production process focusing on four topics: (1) an adapted version of the caregiver questionnaire from specialised palliative care, 23 (2) tools for talk therapy for caregivers,24–26 (3) relevant target groups among caregivers and (4) feasible workflows in the clinic. The video-recorded workshop and observation notes were analysed by two researchers using a rapid analysis approach 28 to identify and resolve dilemmas and achieve consensus on the prototype.
In step 2 (1 February–17 May 2022), we pilot-tested the prototype in five general practice clinics. At a meeting, one GP from each clinic was introduced to the prototype. On registration sheets, the clinics ticked off which tools were used in each Caregiver Care consultation. A healthcare professional from each clinic participated in individual telephone interviews after 4–6 weeks and again after 10 weeks, focusing on experiences with using the prototype and barriers and facilitators for implementation. At the end of the data collection, the healthcare professionals in each clinic answered a shared, short, open-ended evaluation questionnaire, focusing on relevance of the model components and experience with target groups among caregivers. Further, they invited participating caregivers for semistructured interviews, focusing on their experiences with the prototype.
In step 3 (18 May 2022), a final workshop was conducted with one GP from each of the five pilot clinics. Based on the data from step 2, we presented preliminary suggestions for refinements and key uncertainties which were discussed at the workshop. The workshop was video-recorded, and observation notes were made. Subsequently, the researchers refined the prototype to form the final model.
Analysis
A rapid analysis, focusing on the possibilities for improving the prototype, was performed in each of the three steps to refine the model. After step 3, two researchers (AM and SHO) made a rapid qualitative analysis; data were analysed directly from the audio-recordings and compared with observation notes (from step 1 + 2 + 3), registration sheets (from step 2) and questionnaires (from step 2). This produced detailed notes and captured quotes. 28 The focus was on changes made during development, mechanisms of impact of the intervention and the final model. The findings were discussed and negotiated in the research group.
Results
First, the most significant changes from the prototype to the final model will be outlined, followed by findings of how the model may accommodate challenges and needs. Lastly, the final model will be presented.
Changes from the prototype
Several refinements were made from the prototype to the final model (Table 2). In the following, the main refinements are elaborated.
Changes from prototype to final model.

GP, general practitioner.
Dialogue questionnaire
In workshop 1, the purpose of the caregiver questionnaire was discussed. A tick-box was not considered useful. Rather, the questionnaire should facilitate a dialogue regarding help with symptom control, where to access help, communication about the illness, emotional support and previous mental health problems. Consequently, we named the tool a ‘dialogue questionnaire’ to underline the purpose of providing an overview and prioritising relevant issues for the individual caregiver. From the caregiver interviews, it was underlined that both the demands of being a caregiver and the grief reaction were at stake.
The GPs discussed especially the question addressing financial issues and disagreed about its appropriateness: Excerpt 1 (from interviews with GPs and workshop 2): A GP said: ‘I do not want to open too many aspects of the caregiver’s situation that I cannot help with [. . .]. I do not want to create expectations that I cannot fulfil’. This demonstrates that the GP was preoccupied with not promising the caregivers something that general practice would not be able to deliver. Other GPs did not agree. ‘I want to know what is overwhelming for the caregiver [. . .], I want to acknowledge their difficult situation’, a GP said. The differences among the GPs appeared both during and after the pilot-testing. This illustrates that the GPs may have different values and attitudes to their role towards caregivers.
Grief facilitation tools
One GP with extensive talk therapy experience used an overview of domains of grief facilitation, but most clinicians performed consultations and talk therapy based on the dialogue questionnaire and their clinical experience. Most GP clinics were not updated on supportive caregiver interventions in the municipality/municipalities of the caregivers, and a list of current initiatives were therefore developed. In workshop 2, a need for an overview of initiatives in patient associations and religious institutions was requested and subsequently added to the prototype.
Target group
The target group of the intervention was discussed continuously during the development process. The healthcare professionals articulated a need for targeting not only caregivers to terminally ill people but also caregivers to patients with more chronic trajectories: Excerpt 2 (from workshops and interviews with healthcare professionals): During discussions of the definition of the target group (caregivers) of the intervention, the professionals’ immediate response was caregivers to terminally ill patients. However, already in the first workshop, a consensus was reached to focus on caregivers earlier in the patient trajectory, in order to prevent severe conditions for the caregiver. Later, during interviews based on piloting, it was articulated that more chronic trajectories, e.g., in the case of dementia, are fatiguing for the caregivers. Rather, the focus should be on situations where the everyday lives of both patients and caregivers are changed dramatically.
When piloting caregivers to patients with severe somatic illnesses were recruited, but throughout the development phase, it became evident that the inclusion criteria should be broadened to include caregivers to people with psychiatric illness: Excerpt 3 (from workshop 2): The GPs discussed their pilot-testing experiences with the target group. A GP expressed frustration about excluding caregivers to people with psychiatric illness: ‘It is just as hard being a caregiver for someone with a mental disorder. Just as disabling and intrusive in everyday life [as being a caregiver to a person with somatic illness]’. Further, the GPs experienced a much greater need among caregivers to people with mental illness due to a larger taboo and less support elsewhere (e.g., patient associations and hospital departments).
Consequently, a model also targeting caregivers to patients with mental illness would be desirable.
How to accommodate challenges and needs
Acknowledging being a caregiver
In the interviews with the caregivers, the acknowledgement of the hardship of being a caregiver was highly valued. From the caregivers’ point of view, this recognition is often not visible. They expressed that they do not expect or experience that attention is being directed to their needs as caregivers, neither from the healthcare system nor from friends and family. When experiencing an interest in their situation from healthcare professionals through the Caregiver Care Model, some caregivers found that this attention increased their awareness of their own well-being.
Excerpt 4 (from interview with caregiver): Bertha’s husband had been suffering from Parkinson’s disease for more than ten years when she was invited to participate in the intervention. Through the years, her husband’s disease had progressed and increasingly affected their life. ‘We used to play croquet, but after a while he could not do it anymore. He easily falls. And now I have also resigned from participating in playing in club events and tournaments’. Bertha explains that her tasks as caregiver has gradually increased as her husband’s condition has deteriorated, and now she feels ’locked in the house’ as it is difficult to leave him alone to go to the supermarket or have a cup of coffee with their neighbour. ‘I have not really realized how tough it is for me’, she explains and starts crying when she talks about the questionnaire that she had to fill out before the consultation. ‘It is still difficult to talk about. It was all these issues that emerged. It was the questions in the questionnaire. . . then I realized it. All those things. . .that it was in fact a little tough. I haven’t thought about how I was feeling at all for a long time. How do I actually feel? I was to talk to my GP about it. Now it is already easier to talk about’.
In this case, the act of asking, even in the form of a questionnaire, in itself had a profound effect on Bertha. Whether it was the questionnaire, a consultation with the GP or nurse, or just being asked about participating, the caregivers expressed that this form of acknowledgement of their hardship and suffering was an essential part of the intervention.
Preparing for the consultation
The interviews with the healthcare professionals also focused on the impact of model. Due to the dialogue questionnaire, the healthcare professionals found that the caregivers were generally better prepared; the caregivers had reflected upon aspects of their caregiving situation and were therefore better prepared to engage in a dialogue with the healthcare professionals. Consequently, consultations could provide greater impact.
Variation across clinics
In the workshops and interviews with GPs, it was repeatedly highlighted that the clinics varied in terms of geographic location, which influenced their perceived need for providing improved care for caregivers. In remote areas, the longer distance and waiting times to private-practice psychologists and specialised care were perceived to cause a greater demand for improvements in caring for caregivers in primary care.
The final model
The final model is described by its workflow and content.
Workflow
The caregivers are identified in the clinic and provided with a dialogue questionnaire to complete at home. They bring the dialogue questionnaire for the first consultation as a fixed starting point for dialogue about their needs for support and risk of complex grief reactions. The subsequent contacts depend on the individual care plan and could include talk therapy in the clinic, information about local municipal or civil society initiatives or advise to contact the clinic in case of increased need. The healthcare professionals may use the facilitating questions to facilitate grief reactions and/or the list for local initiatives in case of need for referral for support. In the pilot-test, 13 of the 40 caregivers received talk therapy at the clinic. Three were referred to local initiatives or psychologists.
Content
The final model consisted of up to seven individual face-to-face consultations (20–30 min) in general practice based on the following tools: (1) a dialogue questionnaire completed by caregivers to facilitate dialogue regarding support needs, (2) facilitating questions for healthcare professionals to use in talk therapy and (3) an overview of local initiatives for healthcare professionals when additional support was needed (Table 3).
Logic model of the final Caregiver Care Model.

In the short term, the caregivers will receive targeted support, be acknowledged for their difficult situation and their social networks will be activated. In the medium term, the model is intended to improve emotional regulation and coping strategies, whereby preparation of grief reactions will be improved, and the risk of complex grief reactions will be reduced (Table 3).
Discussion
Main findings
We developed the Caregiver Care Model to mitigate grief reactions among caregivers during severe illness and prevent complex grief reactions. The prototype was refined by renaming and focusing the dialogue questionnaire, minimising the grief facilitation tools and expanding the target group. The model seemed to accommodate the needs among caregivers by acknowledging their situation and providing targeted support to the individual caregiver. Further, the model may be more relevant in remote areas with poorer access to specialised services. The final model includes up to seven caregiver consultations in general practice. A dialogue questionnaire filled in by the caregiver serves as a fixed starting point and preparation for the first consultation. If needed, talk therapy in general practice or referrals to services outside general practice are used.
What this study adds
When developing interventions such as the Caregiver Care Model, it should be acknowledged that caregivers often expect themselves to handle the hardships of caregiving as merely a condition of life that must be managed. At the same time, when they experience need for help and support from the healthcare system, they may hesitate to seek help, since they navigate their use of the healthcare system according to a moral ambition to be ‘a good citizen’ who is able to manage life independently. 31 The Caregiver Care Model works in this tension between something that should be handled by caregivers themselves and something that needs an intervention when the ‘chronic homework’ 6 of caregivers becomes too demanding.
In a recent systematic review, the most expressed needs of caregivers were emotional. 7 For their emotional needs, they preferred professional support, open and honest communication and availability of the health professional. 7 This is in line with the purpose of the Caregiver Care Model of provision of targeted caregiver support. 10 A scoping review highlights general practice as well-positioned to support caregivers and describes identification, assessment and referral if needed as key issues of caregiver support. 10 The Caregiver Care Model includes all aspects and may provide new findings to close the knowledge gap regarding how to perform this important task. The current study is promising, especially regarding how to use an assessment tool to systematically map the support needs of caregivers in order to engage in dialogue with the caregiver and thereby mitigate grief reactions and prevent complex grief reactions.
In the Caregiver Care Model, the caregivers’ needs and risks of complications were explored using a dialogue questionnaire adapted from an assessment tool from specialised palliative care. 23 It was considered relevant and usable in a general practice setting, and it was to a larger degree related to the caregiver than the disease stage or diagnosis of the patient. Compared to another needs assessment tool used in general practice, the Caregiver Support Needs Assessment Tool (CSNAT),32–34 the dialogue questionnaire was usable to facilitate dialogue regarding care issues and grief reactions, whereas the domains of CSNAT focus on terminal illness and carer issues. 32 Furthermore, barriers for using CSNAT include reflections about introducing the questionnaire too soon or too late, according to the patient’s disease stage.34,35 However, in this general practice population study, the dialogue questionnaire was perceived to be relevant for all distressed caregivers due to significant impact on the patient’s illness on the everyday life of the caregiver. Further, healthcare professionals presumed that the Caregiver Care Model would be highly relevant for all, including caregivers to patients with mental health issues.
The material provided in the Caregiver Care Model to address grief facilitation was inspired by CGT 27 and adapted to a general practice setting.24–26 The material was directed at caregiving rather than bereavement and scaled down to a brief version focusing on the general practice setting. The short face-to-face teaching about the material in the model to only one GP per clinic was not sufficient for healthcare professionals to use them in consultations, even if they had access to written material. Even if the intention was to introduce overarching domains and basic grief theory, such as the Dual-Process Model, 29 more thorough education seemed necessary for implementation.
A list of facilitating questions for use in talk therapy24–26 was immediately useful for clinicians for inspiration and to provide a structure for talk therapy, and a list of local initiatives for referral with contact information was requested. In the workflow of general practice with very short time for the healthcare professionals to prepare before each consultation, these tools were appropriate. The rapid pace in general practice may also be a reason why it was useful for caregivers to fill in the dialogue questionnaire prior to the consultation. Thus, it provided the caregivers time to reflect upon their situation and to engage in dialogue based on these reflections. The usefulness of preparing patients before consultations in general practice is also found elsewhere. 36
Strengths and limitations
An important strength of this study is the co-production and participatory approach16,17 that allowed us to develop a model that is tailored for the end-users and the existing workflow in general practice. The study also has limitations. The participating test clinics represented a selected group of GPs with a particular interest in quality development. Exploring the feasibility of the model in different clinics could add new perspectives. Also, in this study, we used an implementation-based approach to intervention development, 18 which influenced the decisions of making the model simpler and, at the same time, more flexible for healthcare professionals to use. An efficiency-based approach, 18 on the other hand, would probably have led to another final model, where the teaching session was extended in order for healthcare professionals to understand and adopt the various talk therapy tools. However, this was not within the scope of our study and would also challenge sustainable adoption and implementation of the model.
Relevance for clinical practice
Using the Caregiver Care Model may help caregivers be able to accommodate the hardships of caregiving and provide a legitimate entry point for receiving support from the healthcare system. The flexible model is suitable for the workflow in general practice and appropriate for a broad target group of caregivers. Moreover, the model is not restricted regarding either the problem (e.g. diagnosis, timeframe, severity of illness, age), or the solution (e.g. recognition of suffering, talk therapy in general practice, more practical help, referral to civil society-based support groups or other external actors). However, the flipside of flexibility may be that it becomes difficult to define and legitimise caregivers’ need for care and support. Hence, proactive identification of the needs and risks of caregivers is key in the prevention of complicated grief reactions, and education of healthcare professionals to manage grief reactions during caregiving and enable caregivers to deal with the situation is necessary. By using the approach of the Caregiver Care Model in general practice, GPs and staff may be able to address the needs and concerns of caregivers to enable targeted support, which holds the potential to prevent complex grief reactions.
Further research
A feasibility study is warranted to assess whether the model is implementable for caregivers and healthcare professionals. The model was particularly successful regarding the fixed tool (the ‘dialogue questionnaire’), whereas the flexible tools of grief facilitation demand further training of healthcare professional. Hence, there is a need for future studies on grief facilitation in general practice that includes training of healthcare professionals.
Conclusion
The Caregiver Care Model offers promising support to caregivers experiencing distress by mitigating mental and physical health problems. Its flexible structure allows for customisation. However, it is imperative to conduct further testing of the model to assess its feasibility and effectiveness.
Acknowledging the demanding position of family caregivers and addressing caregivers’ needs for support using the Caregiver Care Model may be a way to reach out to a broad group of caregivers through general practice in order to support caregivers, mitigate grief reactions and potentially prevent complex grief reactions.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524241272103 – Supplemental material for How to support caregivers in general practice: development of the Caregiver Care Model
Supplemental material, sj-docx-1-pcr-10.1177_26323524241272103 for How to support caregivers in general practice: development of the Caregiver Care Model by Anna Mygind, Sara Marie Hebsgaard Offersen, Mai-Britt Guldin, Kaj S. Christensen and Mette Kjærgaard Nielsen in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524241272103 – Supplemental material for How to support caregivers in general practice: development of the Caregiver Care Model
Supplemental material, sj-docx-2-pcr-10.1177_26323524241272103 for How to support caregivers in general practice: development of the Caregiver Care Model by Anna Mygind, Sara Marie Hebsgaard Offersen, Mai-Britt Guldin, Kaj S. Christensen and Mette Kjærgaard Nielsen in Palliative Care and Social Practice
Supplemental Material
sj-docx-3-pcr-10.1177_26323524241272103 – Supplemental material for How to support caregivers in general practice: development of the Caregiver Care Model
Supplemental material, sj-docx-3-pcr-10.1177_26323524241272103 for How to support caregivers in general practice: development of the Caregiver Care Model by Anna Mygind, Sara Marie Hebsgaard Offersen, Mai-Britt Guldin, Kaj S. Christensen and Mette Kjærgaard Nielsen in Palliative Care and Social Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.