
Abstract
Background:
Culturally appropriate communication training programs for a wide range of professions that can be used during infection epidemics are crucial for advance care planning implementation. Starting in 2018, the Japanese Ministry of Health, Labour and Welfare made a major policy change, and doctors, nurses, and social workers, and care managers were identified in the guidelines as the professions that promote advance care planning. Motivated by the lack of online programs for Japanese care managers, we proposed a new one-day program.
Objectives:
This study aimed to determine the changes in the positive attitude of care managers toward dying patients compared to that of nurses, which has been used in past literature as an outcome of advance care planning educational interventions, after administering the program in Japan.
Design:
Before-after comparison study.
Methods:
Care managers were recruited through our website, ACP-Piece, http://plaza.umin.ac.jp/~acp-piece/piece.html. A questionnaire survey concerning positive attitudes toward dying patients was administered before and after the program on 28 August 2021. Sixty-six subjects participated in the training and 60 participants, including 14 care managers, consented to the study and completed the questionnaire surveys before and after the program.
Results:
The Frommelt attitude toward care of the dying scores for care managers increased after the program (p-values, confidence intervals, and effect sizes: p < 0.001, −11.90 to −4.388, −1.252). After training, care managers had a significantly higher maximum score occurrence than nurses. Older care managers with advance care planning experience may have had a higher maximum score occurrence compared to younger, inexperienced participants.
Conclusion:
To our knowledge, this is the first to demonstrate the increased positive attitude scores toward dying patients after online communication training for Japanese care managers. The limitations of this study include the lack of evidence regarding reasons for score changes, long-term score changes, and effectiveness for patients and their families.
Introduction
Advance care planning (ACP) is crucial to respect the person’s wishes1,2 due to increased advance directives, 3 individual preferences for end-of-life care, 4 and patient-centered communication. 5 One of the key factors facilitating ACP is the implementation of frameworks, especially preparations for conversations among practitioners. 6
Another relevant factor affecting the implementation of ACP is the cultural background of the involved individuals. Most ACP protocols were developed in cultures that value autonomy, mainly in English-speaking countries.1,3,4 In contrast, individual autonomy is subordinate to family values and doctors’ authority in East Asian countries. 7 In Japan, for instance, many individuals refrain from clearly expressing their true intentions in a clinical setting. Consequently, healthcare providers strive to read the true ‘wishes’ of patients or their family members by conversing with them. 8 Therefore, the optimal method of implementing ACP in Japanese culture is unclear.
A review of the literature in Japan revealed the need for ACP implementation appropriate for the Japanese to facilitate the expression of individual preferences and values while improving the communication skills of healthcare providers.9–11
Some ACP programs, such as Respecting Choices, have been successfully implemented in Western countries.3,4 This motivated the Japanese Ministry of Health, Labour and Welfare to announce a ‘guideline on the decision-making process in end-of-life care’, which specify the role of care managers in promoting ACP 12 and to promote new programs on Education for Implementing End-of-Life Discussion (E-FIELD).
Attending an on-site E-FIELD program improves the attitudes of physicians, nurses, and social workers toward dying patients 13 and increases their knowledge, confidence, and the number of ACP discussions and completions by physicians, nurses, and social workers. 14
However, no effective ACP programs for Japanese care managers were available until now due to the following reasons. E-FIELD was a program emphasizing that healthcare providers working under the health insurance system make future medical care choices with patients through end-of-life discussions. However, no program emphasized that care managers working under the long-term care insurance system make future medical choices with long-term care service users through daily life support. Note that in some countries, they are called case managers, but in Japan, they are called care managers.
Previously, care managers coordinated long-term care services in the home. However, in 2018, the Japanese Ministry of Health, Labour and Welfare expanded the scope of professions that promote ACP to include care managers along with doctors, nurses, and social workers. In Japan, many care managers lack medical qualifications. Ministry of Health, Labour and Welfare statistics from the past 23 years until 2020 show that 44.2% of care workers, 11.0% life consultants, and 6.4% social workers passed the examinations for care managers, whereas only 23.9% nurses and 2.1% doctors did so. 15 Thus, care managers may feel uncomfortable discussing future healthcare choices and may not consider it their responsibility to do so. 16
Despite the growing need for online educational programs since the beginning of the coronavirus disease 2019 pandemic, no online programs with demonstrated effectiveness are available for care managers. Due to changes in the guidelines regarding care managers, we propose an online role play-based ACP communication training program specifically for care managers. We have offered this 7-h program, named ACPiece, every 2 months, since April 2020.
The program comprises brief lectures and experience-based education, such as scenario readings, videos, role plays, and group work facilitated by past ACPiece trainees who volunteer. Participation in this sustainable ACP communication training program is free.17,18
Using communication skills like repetition and silence, ACPiece helps care service users express their reserved emotions and perceive care managers as understanding partners. This is crucial in Japan, where people often do not disclose their true emotions.
ACPiece refers to these emotions as ‘pieces’. Although Japanese care managers may struggle with discussing future medical choices, they excel at listening to these emotions as they frequently work with long-term care service users. Sharing these emotions with medical professionals is vital for future medical decisions. In Japan, where individuals seldom express their medical preferences, ACPiece emphasizes ongoing discussions between patients, advocates, and care professionals that prioritize the individual’s opinions and values. 12
ACPiece offers free, practical training that incorporates ACP communication skills in participants’ actual workplaces. The program follows the empirical learning theory, emphasizing the consolidation of ACP communication skills through repeated learning and experience. 19
This study aimed to determine changes in care managers’ positive attitudes toward dying patients by conducting an online survey before and after ACPiece.
Methods
Study design and intervention
This was a pre-post comparison study. The intervention was an ACP facilitator communication training program named ACPiece, which we administered on 28 August 2021 to healthcare providers, including care managers, who were recruited through our website. 17 An online questionnaire survey on the positive attitudes toward dying patients was administered before and after the program.
The following definition of ACP was adopted from the Japan Geriatrics Society because the study was conducted while considering Japanese culture: ‘ACP is a process that supports people to make decisions paying respect to each individual as a human about their future medical and long-term care’. 8
Data collection
From 21 March to 21 April 2021, participants in the ACP communication training program were recruited through the authors’ website. 17 According to the search engine optimization tool Labo GRC ver. 5.65.274, developed by Shellware Co. in Shizuoka City, Japan, this site is consistently ranked first to fifth in Google for the Japanese search term ‘ACP Training’. This website contains information on ACP training, practical books on ACP conversation, and case studies, including information on ethical issues. Visitors directed to this site by chance or word of mouth and who wished to participate in ACPiece filled out a required Google form to provide their necessary information. All participants were approached to participate in the study on 28 August 2021.
These volunteers were asked to participate in the study before the program. Only those who agreed to participate completed a separate research Google form.
Participants entered their names, e-mail addresses, job titles or positions, region of work location in Japan, age, and ACP experience in their profession into a Google spreadsheet linked to a Google form.
Although the primary target population of our study was care managers, we also recruited other participants. We wanted to measure the care managers’ attitudes toward dying patients when they were trained with representatives of multiple professions, including citizens not involved in care activities.
Measurements
A questionnaire, the Frommelt attitude toward the care of the dying (FATCD-Form B–J) scale, referred to hereafter as the FATCD score, was used to measure the positive attitudes toward dying patients. This questionnaire consists of 30 items. 20
This questionnaire was developed by Frommelt 20 and was confirmed to be reliable and valid in Japanese by Nakai and Miyashita. 21
We selected FATCD as the outcome measure to evaluate the effectiveness of ACP education programs for the following five reasons.
(1) This questionnaire has been used previously to assess attitudes toward ACP.13,22,23 (2) A paper discussing the role of Japanese care managers in ACP highlights the communication barriers and challenges in explaining end-of-life issues. 24 (3) Outcomes of ACP education programs are not always clear. 25 (4) Care managers often face obstacles when discussing future medical decisions for terminally ill patients, 16 likely due to their lack of certification as medical professionals. 15 (5) To validate the development of the ACP Inventory for Japanese group home managers and care planners, the FATCD score was used as an external standard. 26
Thus, the FATCD score is an appropriate outcome measure for ACP educational interventions in Japanese culture.
Our sample size was calculated based on data from Miura et al. 13 who reported FATCD scores before and after E-FIELD training. With a two-tailed test at a significance level of 0.05 and power of 0.8, we arrived at a sample size of 8. We anticipate 60 participants in the training, of whom 25% will be care managers and 80% will agree to participate in the study, allowing us to obtain the required sample size.
Ethical considerations
The study was conducted in compliance with ethical guidelines for life science and medical research involving human subjects. All study participants provided informed consent online by completing a Google form linked to a Google spreadsheet. The anonymity of the participants was preserved. The study was approved by the Institutional Review Board of the National Center for Geriatrics and Gerontology (No. 1528) and conforms to the provisions of the Declaration of Helsinki (as revised in Brazil 2013).
Statistical analysis
Data from participants who agreed to the study and completed the questionnaire survey before and after the online training were analyzed. No data were missing. Continuous variables are presented as means and standard deviations and categorical variables are presented as frequencies and percentages. The p-values, 95% confidence intervals (CIs), and effect sizes for the differences in scores before and after the training are shown. The p-values of less than 0.05 were considered statistically significant. For the Cohen’s d and Cohen’s h demonstrating effect size, 27 0.2 was considered small, 0.5 medium, and 0.8 large.
Although the primary target population of this study was care managers, we compared care managers with nurses. This was because we wanted to compare nurses working under the medical insurance system with care managers working under the long-term care insurance system.
FATCD scores were compared before and after training for care managers and nurses.
Percentage of maximum score occurrence on FATCD scales before and after the training were compared between care managers and nurses. As Japanese care managers lack medical qualifications 15 and are hesitant to discuss end-of-life medical choices, 16 we hypothesized that suitable training would enhance the positive attitudes of care managers and nurses toward dying patients.
Percentage of occurrence on FATCD scores were compared separately for care managers with and without ACP experience and according to age. Positive perceptions and experience increase the ability of care professionals on their patients.28,29 We hypothesized that experience and age are related to their attitude toward ACP, which could be applicable to care managers as well. Using exploratory analysis, we identified two FATCD score distribution patterns, Pattern A and Pattern B, based on experience and age of ACP communication with patients. Pattern A includes item numbers 1, 2, 4, 6, 7, 10–20, and 27–30, while Pattern B includes 3, 5, 8, 9, and 21–26. We compared the occurrence percentage of FATCD scores for each pattern and conducted linear or nonlinear regression analysis for each.
Microsoft® Excel® 2016 MSO (version 2022) produced by Microsoft Corporation, U.S.A and EZR version 1.55 were used for statistical analyses.
Results
Training was administered to 66 participants, and 60 participants consented to the study and completed online questionnaire surveys before and after the training. Two care managers, three nurses, and one pharmacist did not consent to the study and did not complete the questionnaires. The response rate for the questionnaire survey was 90.9%, with an acceptable margin of error of 4% at 95% CI. Table 1 lists the characteristics of the 60 ACP training participants included in the study.
Characteristics of ACP training participants.
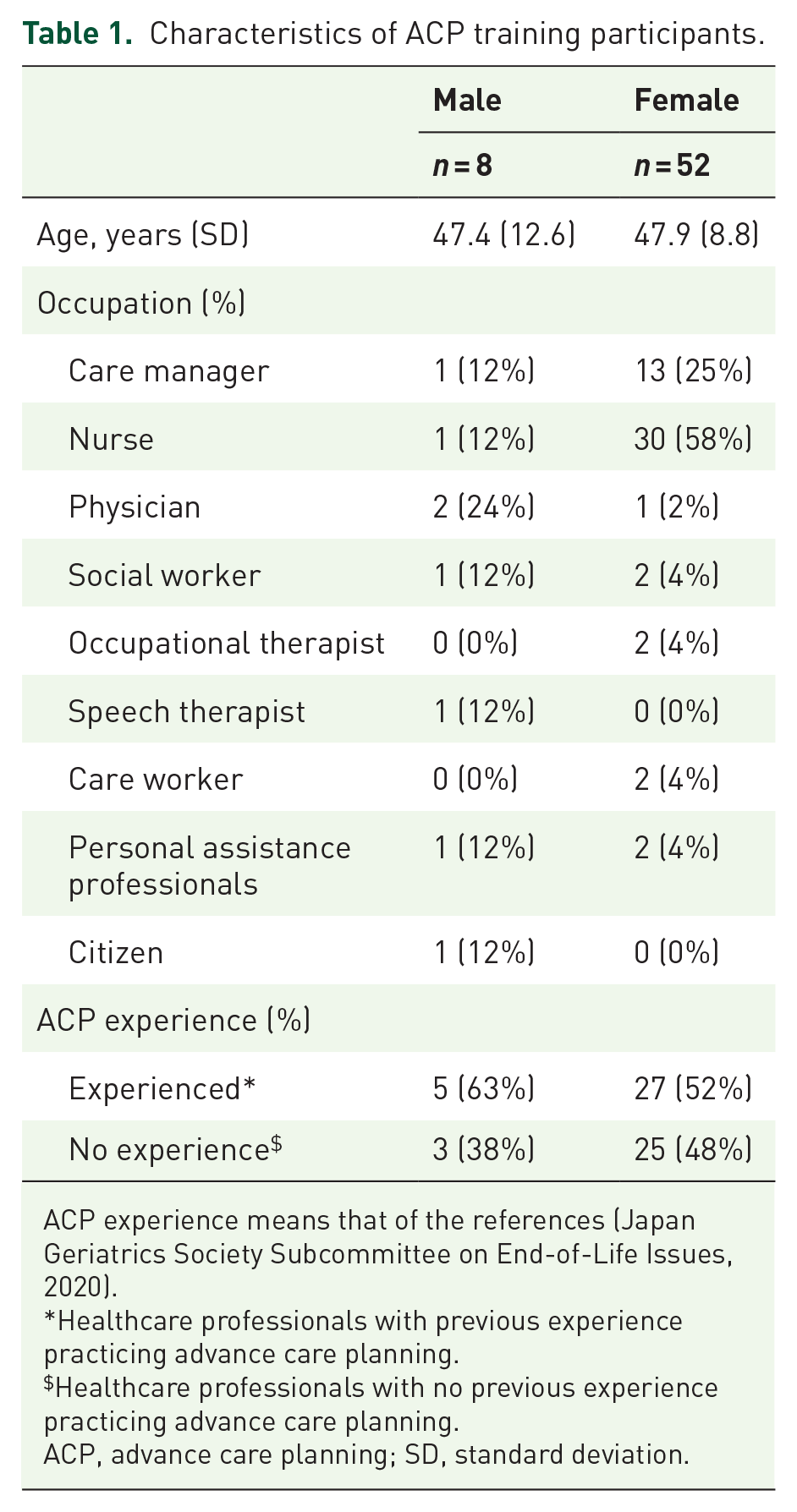
ACP experience means that of the references (Japan Geriatrics Society Subcommittee on End-of-Life Issues, 2020).
Healthcare professionals with previous experience practicing advance care planning.
Healthcare professionals with no previous experience practicing advance care planning.
ACP, advance care planning; SD, standard deviation.
The distributions of the FATCD scores were examined. A calculated Shapiro–Wilk p-value was assigned: 0.77 for the pre-FATCD score, 0.13 for the post-FATCD score. All of the scores were normally distributed.
One-day online ACP communication training program was implemented. Contents of the program are listed in Table 2.
Contents of ACP communication training programs.

ACP, advance care planning.
Changes in FATCD scores before and after training are shown in Table 3. The FATCD scores for care managers increased after the program (p-values, 95% CIs, and effect sizes: p < 0.001, −11.90 to −4.388, −1.252). Post-hoc power analysis based on a two-tailed test with a significance level of 0.05 and 14 care managers showed a power of 0.99, indicating a high level of power.
Changes in FATCD scores before and after training.

FATCD score means Frommelt attitude toward the care of dying scale (FATCD-Form B–J). FATCD scores increased before and after ACP communication training (p-value, 95% CI, Cohen’s d: p < 0.001, −11.90 to −4.388, −1.252). All participants and nurses were noted as well as care managers.
ACP, advance care planning; CI, confidence interval; FATCD, Frommelt attitude toward care of the dying; SD, standard deviation.
FATCD-Form B–J.
p < 0.05. **p < 0.01.
Percentage of maximum score occurrence on FATCD scales before and after the training between care managers and nurses are shown in Table 4. Percentage of maximum score occurrence on FATCD scales after training for care managers was statistically significantly higher than that for nurses (p-values, 95% CIs, and effect sizes: p = 0.0012, −0.153 to −0.042, −0.236).
Percentage and number of the maximum FATCD score occurrence before and after training between care managers and nurses.
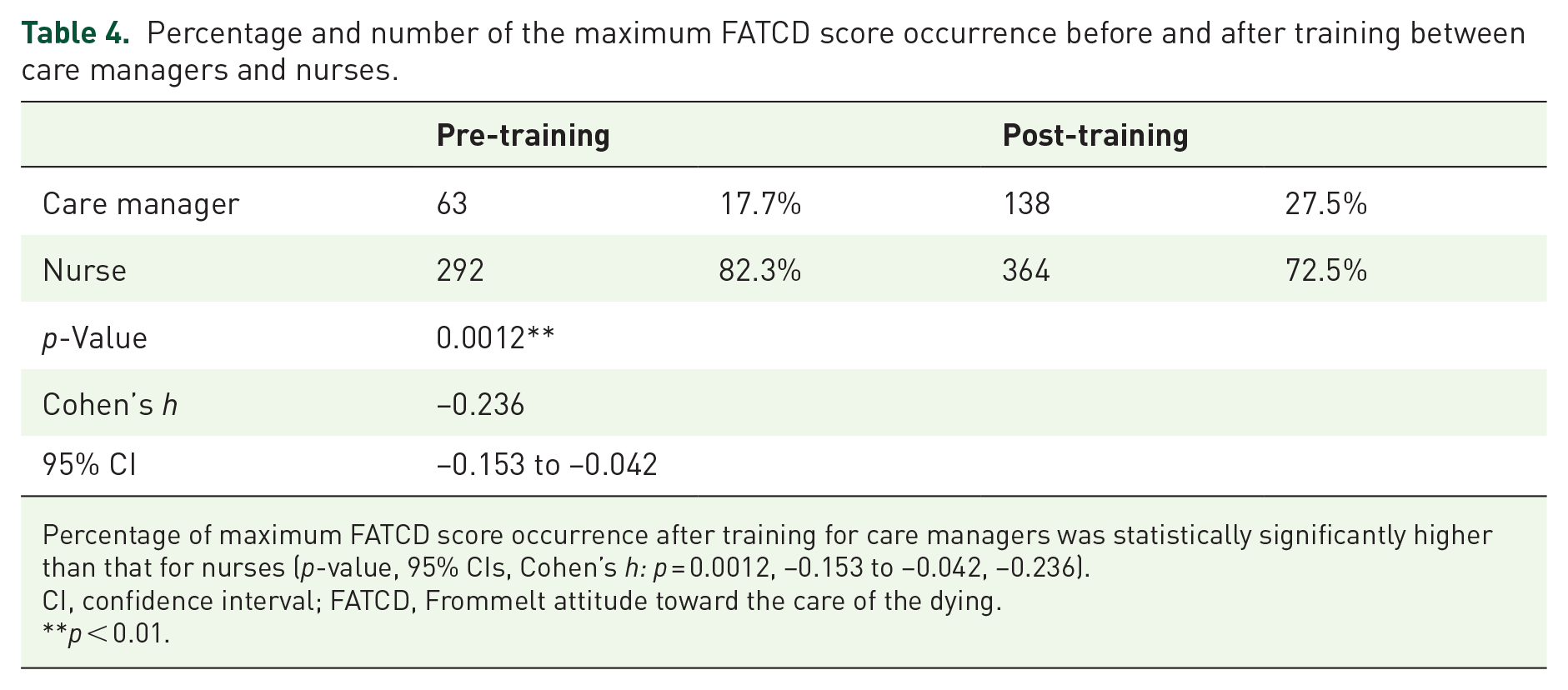
Percentage of maximum FATCD score occurrence after training for care managers was statistically significantly higher than that for nurses (p-value, 95% CIs, Cohen’s h: p = 0.0012, −0.153 to −0.042, −0.236).
CI, confidence interval; FATCD, Frommelt attitude toward the care of the dying.
**p < 0.01.
Percentage of occurrence on FATCD scores before and after the training with and without ACP experience and according to age for care manager are shown in Figure 1. Linear or nonlinear regression analysis revealed a linear increase on FATCD scores for care managers with ACP experience or aged more than 50 years after training.

Relationship between ACP experience or age and the percentage of FATCD score occurrence for care managers. FATCD scores denote the Frommelt attitude toward the care of the dying scores. The x-axis denotes the FATCD score of 1–5, and the y-axis denotes the percentage of occurrences of a FATCD score of 1–5. A and B are two typologies of FATCD score emergence patterns in 14 care managers. Note that Pattern A contains 20 item numbers, 1, 2, 4, 6–7, 10–20, 27–30 and Pattern B included 10 item numbers, 3, 5, 8–9, 21–26. Linear or nonlinear regression analysis was performed for each pattern. Before and after denote before and after training. Ex and noex denote with and without previous ACP experience. Over 50 and under 50 denote over and under 50 years old. Black closed circles, triangles, diamonds, and squares denote four combinations: (1) FATCD score distribution pattern A or B, (2) pre- or post-training, (3) with or without ACP experience, and (4) age over or under 50 years. Solid and dotted lines denote linear and nonlinear regression polynomial approximation curves. The square of R is the coefficient of determination. Regression equations were also presented. Linear or nonlinear regression analysis revealed a linear increase in percentage of FATCD score occurrences for care managers with ACP experience or age 50 or older after training. Thus, care managers with advance care planning experience and aged more than 50 years might have had a higher percentage of maximum FATCD score occurrence after the training than those with no experience and aged less than 50 years.
Discussion
To our knowledge, this is the first to demonstrate the increased positive attitude scores toward dying patients, after online communication training, not only among nurses but also among care managers, especially those aged 50 years or older with ACP experience.
The most important finding of this study was the increased positive attitude scores toward dying patients after training for care managers. The role of care managers in ACP was previously emphasized in a guideline on the decision-making process, 12 but no clear evidence supported this guideline. Unlike our study, those of Miura et al., 13 Hamayoshi et al., 23 and Tanaka et al. 30 did not focus on care managers.
The second important finding of this study is the increased positive attitude toward dying patients as an outcome. Previous literature also examined the positivity of attitudes toward dying patients as an outcome, but without statistically significant results. 30 A previous study demonstrated training effects on the positive attitude toward dying patients as an outcome for medical professionals but not for care managers.13,23 Increased positive attitudes alone do not guarantee that care managers will play a role in ACP, but they are an important change.
The third important finding may be that sustainable, free, hands-on training, in which anyone can participate as both trainer and trainee, reveals an increase in positive attitudes. Unlike the studies of Miura et al., 13 Hamayoshi et al., 23 and Tanaka et al., 30 in our study, a trainee from a previous training program served as the trainer for the ACP communication intervention.
A particularly interesting finding of this study was the feasibility of online training, where realistic communication may be difficult when practicing serious dialogs about ACP. Unlike the studies of Miura et al., 13 Hamayoshi et al., 23 , and Tanaka et al., 30 in our study, the ACP communication training was conducted online.
The limitations of this study include (1) the small number of participants, (2) the self-selection bias of participants interested in ACP communication, (3) unclear reasons for FATCD score changes, (4) the unknown long-term effects of ACP communication, and (5) the lack of evidence regarding effectiveness for patients and their families. Concerning the third limitation, we considered that a mere day of training might improve knowledge scores, although the attitude scores would be difficult to improve and the reason for the improvement would be unclear. According to the free-text statements of the trainees of the participants in this study related to the questionnaire, or according to the opinions of the trainers, who were care managers, the following four reasons could have potentially improved positive attitudes toward dying patients, despite the shortness of the one-day version program.
(1) Hands-on sessions, accounting for more than 90% of the sessions; (2) stepping up from easy to difficult communication skills; (3) rather encouraging communication failures in training; (4) emphasis on understanding the lives, relationships, and values of the people involved as well as their medical choices. However, these four reasons have not reached theoretical saturation as a qualitative study. Concerning the fourth limitation, we considered that long-term changes in the attitude toward dying patients should be identified similar to previous studies. 23
Conclusion
We proposed a one-day version of an online role play-based ACP communication training program, named ACPiece, for various participants, most of whom were connected to the healthcare sector. Their responses to the accompanying questionnaires revealed that such a program has the potential to improve the positivity of care managers’ attitudes toward their dying patients.
Our clinical research has implications for the upcoming steps in clinical practice and research, such as why a one-day version of this program improved the positive attitude toward dying patients, whether the positive attitude of the care managers persists over time, and whether changes in the attitude of the care managers have implications for care service users.
In the future, we should conduct the following three studies. First, a qualitative study with interviews should be conducted to determine why the FATCD scores changed before and after the ACPiece program. This study is currently ongoing. Second, long-term changes in the positive attitude of the care managers toward dying patients after the ACPiece program should be determined. This study is currently under revision by the Research Ethics Committee. Third, care managers, who have completed the ACPiece training program, should aim to administer ACP to patients and their families to assess the outcomes of this program. We have launched a clinical trial named ‘Implementation of Advance Care Planning by Care Managers: A Multi-Institutional Pre- and Post-Pilot Comparative Study’ (Trial ID UMIN000048573) and posted its details on the internet. 31 The interventionists in the trial were care managers who had undergone repeated ACPiece communication training, and the primary endpoint was the patients’ ACP engagement. The trial is currently ongoing.