
Abstract
Context:
The majority of people with serious health-related suffering in low- and middle-income countries lack access to palliative care (PC). Increased access to PC education is greatly needed.
Objectives:
This paper describes the process to adapt an advanced PC training course for a Chilean context.
Methods:
A joint team of intercultural PC educators from the US and Chile conducted a series of key informant interviews and a target audience survey to iteratively design a PC training course in Chile.
Results:
Eight key informant interviews identified a strong need for formal PC education pathways, confirmed the five central learning domains, and helped to identify potential course sub-topics. A target audience survey of 59 PC providers from across Chile confirmed a strong desire to participate in such a course.
Conclusion:
Our team of intercultural PC educators adapted an advanced PC course to the unique context of Chilean providers.
Introduction
Palliative Care (PC) is a medical specialty focused on relieving the suffering of seriously ill patients and their families. The World Health Organization has identified access to basic PC services as an ethical mandate for health systems worldwide. However, only around 14% of patients with serious health-related suffering have access to PC. 1 Additionally, nearly all comprehensive and integrated PC services exist within high-income countries as 42% of countries have no known PC services, and another 32% have only isolated PC programs. 2 A key component of increasing access to PC services is implementing high-quality and culturally adapted provider education and training. 3
Within the context of Chile, PC was first mandated as a guaranteed component of cancer care by the Explicit Health Guarantees Law in 2004. 4 This has led to the creation of 250 PC units across Chile, providing a mixture of outpatient and inpatient services. 5 These units also provide hospice and end-of-life care as an integrated part of comprehensive PC, as opposed to the more siloed model of hospice care that exists within the US and the UK. However, there is a substantial lack of formal training opportunities for clinicians that work in these units. According to a 2022 analysis of 201 of the PC units across Chile, only 33% of physicians and 23% of nurses had received any formal training in PC, defined as a diploma level or higher.5–9
The shortage of formal training is a critical barrier to the provision of high-quality PC services across Chile. Without robust, evidence-based training for clinicians, patients are unlikely to receive the physical, psychosocial and spiritual support of a comprehensive palliative care service. 10 At the undergraduate level, 86% of nursing schools and 67% of medical schools include PC as part of the mandatory curriculum, although most of the exposure is through theoretical classes, with little practical exposure. 9 Palliative care as a subspecialty was only recently recognized in Chile by the National Commission on Accreditation of Medical Subspecialties (CONACEM) in 2021. 5 To support the advancement of PC in Latin America, collaborators from Massachusetts General Hospital (Boston, USA) and Pontificia Universidad Católica de Chile worked together to create a diploma-level course for physicians with at least 2 years of PC experience. This paper outlines the strategic process with which the structure and curriculum for the course were created.
Methods
This qualitative research was conducted in Chile. It combines semi-structured interviews with PC leaders in Chile and an online structured survey of PC physicians working in PC services in different places in Chile and was conducted following the consolidated criteria for reporting qualitative research (COREQ). 11
The initial framework for the course was first adapted from the Harvard Palliative Care Education and Practice (PCEP) course. PCEP is a Continuing Medical Education course offered by the Harvard Medical School Center for Palliative Care to physicians, nurses, social workers, and other providers worldwide to enhance their communication, teaching, clinical practice, and program development skills within the context of PC.12–14 All four of the course directors for the Chile diploma program had previously taken PCEP, and unanimously agreed that it served as a strong initial structure from which to build.
To fully adapt this structure to the unique learning needs of participants, a two-part adaptation process was conducted. First, a series of key informant interviews (KIIs) with PC leaders across Chile were conducted using a semi-structured interview format. A PC leader was defined as a PC clinician with formal training in PC, and at least ten years of clinical experience or a leadership position in the field of PC.
The two Chilean course directors (OL, PP) conducted these interviews, both of whom have prior training in qualitative research methods. They did not interview leaders who worked on their own clinical team. Participants were initially identified by the Chilean course directors, and then snowball sampling was used to identify as many relevant participants as possible. Each participant was initially approached via an email invitation, followed by a video call to review the goals of the interviews. The duration of the interview was about 1 h. A semi-structured interview guide was used for each participant and included the following: a SWOT analysis (strengths, weaknesses, opportunities, and threats) of the status of PC in Chile, perceived PC educational needs of colleagues, and recommended course content for an advanced diploma-level course. These interviews were recorded, and the researchers took hand notes. The data was analyzed using a 2-step rapid qualitative inquiry. 15 This method was chosen to analyze information via a collaborative, team-based approach to identify common themes.
The next step of the adaptation process was a target audience survey sent to potential students for the course. This survey was developed based upon the responses from the KIIs. A convenience sample of participants for the target audience survey was identified by emailing current members of the Chilean Society of Palliative Medicine. The survey domains included a self-assessment of competencies in core PC topics, participants’ interest in receiving increased training in specific sub-topics, and perspectives on an ideal structure for an advanced training course. Adapted Likert scales were used for each of these three components of the survey. The combined results from parts one and two were then integrated by the team of course directors to create the final course curricula and schedule.
Results
Key informant interviews
A total of eight PC leaders from across Chile were interviewed. All eight participants noted that the national mandate for PC for cancer patients instituted in 2004 had made a significant impact on the growth of PC services. However, all of them also identified that the lack of formal training was a central barrier to the further advancement of PC services. All eight participants were supportive of the proposed plan to create a diploma-level training course to enhance the practice of providers who currently work within a PC context but have never received any formal training.
The general curricular structure of the PCEP course was proposed to participants as follows: Communication (35%), Symptom Management (25%), Psychosocial aspects of care (15%), Program Development (15%), and Teaching Principles (10%). Most participants agreed with this general composition of domains. Many of them specifically noted the importance of communication skills in practicing PC, given that it is rarely taught within medical training in Chile. Within these domains, participants were also asked to suggest potential subtopics that should be included in the course that would be most relevant to practice in Chile (Table 1).
Suggested sub-topics from KIIs.

Target audience survey
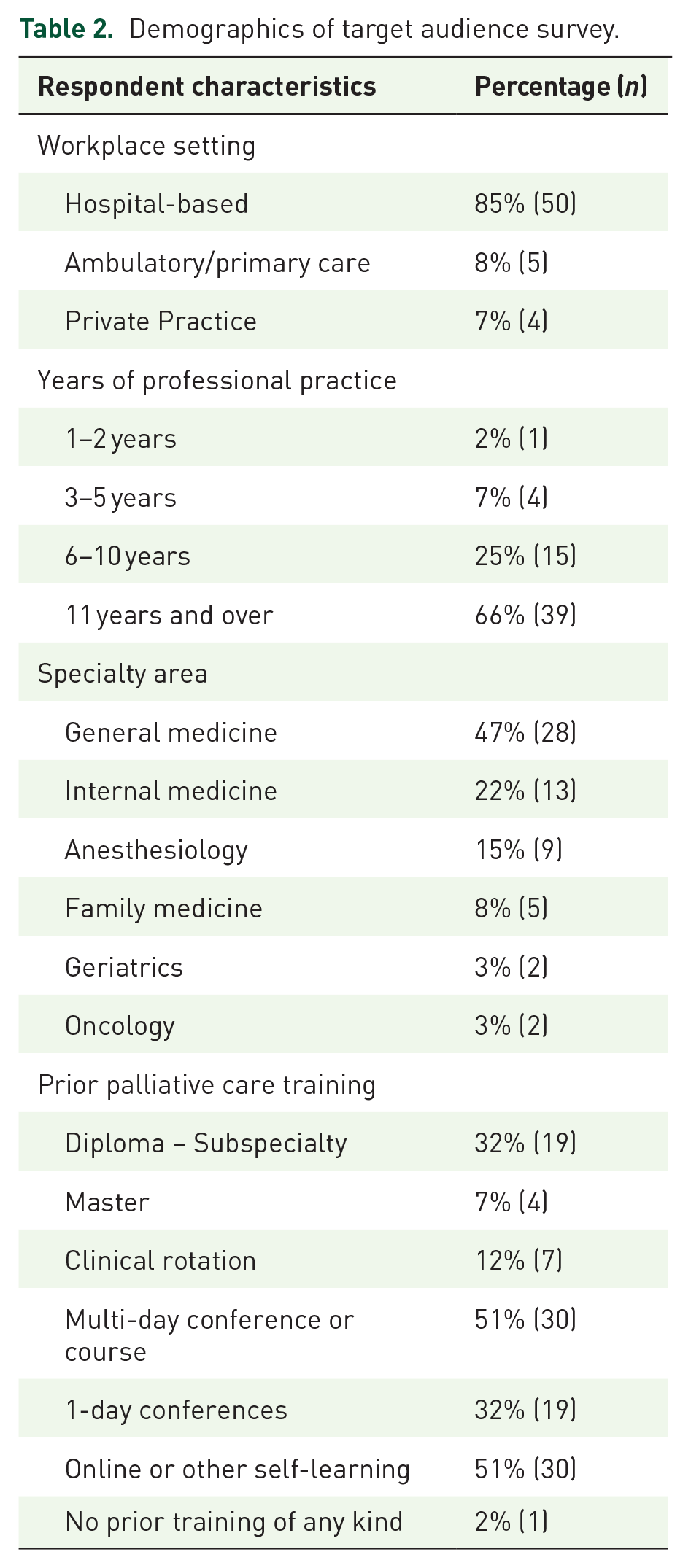
Of the 78 members that received an email, a total of 59 members answered the survey, with a response rate of 76%. Ninety-two percent (n = 54) had been practicing PC for more than 6 years. Fifty-three percent (n = 31) of respondents reported having received formal, in-person training resulting in a diploma or higher. The other 47% (n = 28) reported that their only prior PC training was either a short online course or attending an academic conference (Table 2).
Demographics of target audience survey.
In this survey, participants reported a high degree of confidence in the five identified core domains of PC practice, ranging from a mean of 5.2 (program development) to 5.8 (ability to communicate with patients and families) on a 1–7 scale. They also reported a strong interest in learning more about each of the 17 suggested sub-topics (maximum 4.5, minimum 4.1 on a scale of 1–5), with chemical coping, euthanasia, physician-aid in dying, and palliative sedation, having the highest scores. Lastly, participants reported a strong interest in utilizing a hybrid course structure, including asynchronous online learning (4.5), virtual case discussions (4.4) and virtual group discussions (4.3) on a scale of 1–5.
Diploma changes
With the gathered information, the international collaboration team defined the contents and educational strategies of the new diploma. Multiple content areas were either added, removed or adapted based on the findings from the KIIs and target audience surveys (Table 3). Further details, including the rationale for these changes, are included in the discussion section below.
Comparison of the contents of the original PC program and adapted PC course.

Discussion
This paper reports the results of a two-step, mixed methods process to create a high-quality PC education program specifically adapted to the context of PC providers in Chile. This adaptation process was iterative and was also co-led by an equal team of PC educators from two countries (two from Chile and two from the United States).
Several key changes were made to the course content via this two-step adaptation process. Though the core themes and general composition of the course remained the same, many of the more specific areas of focus were modified. For example, though the communication session focused on how to respond to requests for miracles was maintained, a second session on the theology of miracles within the predominantly Catholic culture of Chile was also added. Additionally, managing complex family dynamics was maintained, but with a specific focus on the commonly encountered ‘conspiracy of silence’ where families and clinicians silently agree not to discuss prognosis with an elderly patient. New sessions focused on PC for non-oncology patients as well as how to effectively integrate PC into primary care were also added, as these reflect recent policy initiatives from the Chilean Ministry of Health to expand PC services beyond oncology.
Other content areas present in the US-based course were removed from the Chilean diploma. This included a session on best practices for pain management within the context of an opioid epidemic. In Chile, like most of Latin America, the core challenge with respect to opioids is actually a lack of access for seriously ill PC patients that need them most. Several other more theoretical sessions, such as teaching pedagogy, bereavement best practices, and death and dying literature, were also removed based on feedback to make the diploma as practical and applicable as possible.
The need for increased formal education pathways was one of the most common and heavily emphasized points made within the KIIs. Despite this unanimous support for enhanced educational opportunities, there were some variations in their perspectives on the most important domains to include. For example, though most interviewees highlighted enhanced communication skills as an essential domain, one interviewee questioned whether communication skills were a part of PC practice. Such heterogeneous responses are likely a reflection of the diversity in prior training of these leaders, as many have studied in different countries outside of Chile, and each identified using varying resources for self-learning over their many years in practice. This diversity is not surprising, given PC services strive to be designed and adapted to the unique cultural context of the local population. However, it does highlight the importance of building more robust education pathways inside of Chile so that home-grown future leaders of PC feel empowered and equipped to collectively determine the model of PC that best meets the needs of the Chilean people.
Just as the key informants noted the immense need for enhanced education pathways, the target audience surveys also revealed a strong desire for further formal training. Interestingly, despite having a high degree of confidence in their ability to execute on the five core domains of PC practice, respondents still communicated a desire for further training in each of the 17 sub-topics within these domains. This may be evidence of the Dunning-Kruger effect, in which people overestimate their abilities within a context where they have not yet engaged with the full complexity of a multifaceted task, such as communication skills or psychosocial suffering.16–19 Lastly, the target audience respondents also noted the need for non-traditional teaching methods such as asynchronous virtual learning, as well as virtual case review and discussion sessions. This highlights the importance of designing educational programs that are as accessible as possible to reach the largest potential audience.
Limitations
This study had several limitations. First, the sample size of the initial KIIs was very small. Because PC is a new specialty and in an early stage of development in Chile, there are only a small number of nationally recognized leaders. Though snowball sampling was utilized to maximize the sample size, only eight potential key informants were identified. Second, the data from the KIIs was not audio recorded, but shared with the working group via structured notes and analyzed using a rapid qualitative inquiry. These methods were selected to help seed discussion between the course directors as they collaboratively reviewed the notes. However, this method could have also been a source of bias, leading to findings more aligned with the individual perspectives of the interviewers. Lastly, the target audience surveys were limited by the fact that nearly half of the respondents had minimal prior formal training in PC, making it difficult for them to accurately reflect on their personal learning needs.
Conclusion
There remains an immense need for the expansion of comprehensive, culturally adapted PC services around the world – especially within the low and middle-income countries where the burden of serious-illness-related suffering is the greatest. This study resulted in substantial changes made to a potential curriculum to provide formal PC training to clinicians across Chile. However, for those seeking to expand palliative education globally, the key lessons from this study are not these specific curricular changes, but rather the details of the adaptation process that was utilized. Additionally, adaptation based on feedback from local learners and course participants should be continuously repeated even after a course has been designed and implemented. Though the first version of this course was delivered in 2019/2020, a continuous quality improvement process has been used to continue to evolve the course to better meet the learning needs of the participants.
The adaptation steps of this PC education program confirm a core global health principle that education programs cannot simply be lifted from a US context and dropped into a new environment. The creation of sustainable and culturally adapted programs requires a comprehensive and intentional adaptation process that this paper describes. Though such a process could ideally be replicated in other parts of the world where the need for PC remains extremely high, it should be expected that such replication will produce a different result – similarly matching the context and needs of the local patients and clinicians it aims to serve.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524231209057 – Supplemental material for The development of an advanced diploma program for palliative care leaders in Chile
Supplemental material, sj-docx-1-pcr-10.1177_26323524231209057 for The development of an advanced diploma program for palliative care leaders in Chile by Mark Stoltenberg, Ofelia Leiva-Vásquez, Pedro E. Pérez-Cruz and Bethany-Rose Daubman in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524231209057 – Supplemental material for The development of an advanced diploma program for palliative care leaders in Chile
Supplemental material, sj-docx-2-pcr-10.1177_26323524231209057 for The development of an advanced diploma program for palliative care leaders in Chile by Mark Stoltenberg, Ofelia Leiva-Vásquez, Pedro E. Pérez-Cruz and Bethany-Rose Daubman in Palliative Care and Social Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.