
Abstract
Background:
Advanced cancer patients need an accurate understanding of their prognoses in order to engage in informed end-of-life care treatment decision-making. Latino cancer patients experience disparities around prognostic understanding, in part due to a lack of culturally competent communication around prognosis and advance care planning (ACP).
Objective:
The objective of the present study of Latino patients with advanced, terminally ill cancer is to examine their understanding of prognosis, and how cultural factors may influence this understanding and engagement in ACP.
Methods:
A mixed methods study was conducted, which consisted of surveys and semi-structured interviews. Descriptive statistics were used for sociodemographic information and self-reported prognostic understanding. Interviews around prognostic understanding and cultural influences on this understanding and engagement in ACP were recorded, transcribed, and then coded and analyzed using thematic content analysis.
Findings:
Latino patients with advanced cancer (n = 20) completed a self-reported survey and participated in a semi-structured interview. Results indicate that among terminally ill patients, 50% of the patients inaccurately believed they had early-stage cancer, 85% did not believe their cancer was terminal, and 70% believed their cancer was curable. Moreover, interviews yielded two main themes: varying levels of awareness of the incurability of their cancer and diverse end-of-life care decision-making and treatment preferences based on prognostic understanding. Within these themes, patients expressed denial or acceptance of their prognosis through communication with the oncologist, the importance of family, and incorporating their pre-existing beliefs.
Conclusion:
Findings indicate the importance of communication, family involvement, and incorporation of beliefs for promoting an accurate prognostic understanding among Latino patients. It is imperative to address disparities in Latino advanced cancer patients’ prognostic understanding so they can engage in informed treatment decision-making around end-of-life care.
Introduction
Understanding prognostic information and engaging in advance care planning (ACP) is essential for informed end-of-life treatment decision-making among patients with advanced cancer. Informing patients about their terminal prognosis is a critical step during the end-of-life process to help patients make informed treatment decisions.1,2 Prognostic understanding is composed of multiple facets and can include terminal illness acknowledgment, recognition of incurable disease status (e.g., not curable), knowledge of the advanced stage of one’s disease, anticipation of a limited life expectancy measured in months rather than years, 3 and life expectancy based on perceived well-being, rather than a medical estimate. 2
Most patients with advanced cancer fail to understand their prognosis accurately, with many patients believing their cancer is curable when it is not.4,5 In a prior study of patients with advanced cancer, between 69% (lung) to 81% (colorectal) of patients inaccurately believed their incurable cancer was curable. 6 This has negative implications for patients’ ability to engage in informed treatment decision-making at the end of life because patients are making treatment decisions based on a likely false hope of cure.
A group highly at risk for not understanding the incurability of their cancer is Latino patients with advanced cancer,1,7 who suffer disparities in prognostic understanding and engagement in ACP. 8 One prior study conducted with Latino patients with advanced cancer shows that 31% were unsure of their incurable cancer, and 40% found it difficult to discuss treatments because they did not understand their available treatment options. 9 Additional research among Latino patients with cancer reveals that Latinos report having lower levels of diagnostic awareness than their non-Latino counterparts. 10 This lack of understanding adversely impacts their treatment decisions and disease management, such as avoiding information and being passive in their decisions. 10 For instance, only 11% of Latino patients with expected prognosis of less than 6 months reported being terminally ill, compared to 39% of White, non-Latino patients. 11 These studies illustrate the importance of ensuring that Latino patients with cancer have an accurate understanding of the incurability of their cancer.
Key cultural differences may be impactful to prognostic awareness and end-of-life decision-making, therefore leading to differences in end-of-life care treatment trajectory for Latino patients. 12 During this trajectory, Latinos tend to lack awareness during a choice of treatment, 10 have higher home death rates and lower hospice care utilization,13–17 and rely on physicians in determining needed treatment. 18 Additionally, Latinos have a preference for a family-centered approach to determining end-of-life goals of care, 19 which can be attributed to the strong familial bonds prevalent in Latino culture, influenced by cultural values such as familismo.16,17,20,21 Familismo, is the loyalty to one’s family and highlights how Latino individuals often prioritize the family over others’ or one’s interests.22,23 This cultural bond influences a patient’s health behavior and aspects of end-of-life care and decision-making, such as lack of medical continuity to keep supporting the family economically or choosing to attend medical visits due to support of the family. 22 Such value underscores how Latino individuals often prioritize cultural values in end-of-life decision-making.22,23 Understanding and integrating key cultural values of Latinos, such as familism and miracles, into end-of-life care planning may help improve awareness and engagement in ACP and, ultimately, promote informed decision-making around end-of-life care.
In short, lack of culturally sensitive interventions could lead to poor understanding and inadequate engagement in end-of-life decision-making. 12 For instance, patients with advanced cancer who do not accurately understand their prognoses are more likely to receive aggressive treatments in the last week of life.24–26 This, in turn, may impact their quality of death and unnecessarily increase suffering. The lack of culturally sensitive interventions may contribute to a lack of prognostic awareness among Latino patients with advanced cancer, who engage in ACP at much lower rates than their white counterparts. 10
To develop interventions that can improve prognostic understanding among Latino patients, it is critical to understand how they integrate their own values and beliefs into their prognostic understanding and their ACP process. The goal of the present study was to examine Latino advanced, terminally ill cancer patients’ understanding of their curability and the influence of their cultural and other values on their prognostic understanding and ACP decision-making processes using brief surveys and in-depth semi-structured interviews.
Methods
Recruitment and procedures
Patients were recruited from outpatient oncology clinics at Weill Cornell Medicine (New York, NY, USA) between August 2016 and June 2017. Patient eligibility criteria included: (a) diagnosis of advanced cancer (defined by the presence of distant metastases and treating oncologists’ estimate that the patient would live ⩽12 months), (b) ⩾21 years, (c) fluent in English or Spanish, and (d) adequate physical and psychological well-being to complete study interviews. 12 Patients meeting eligibility criteria were screened through the electronic health record by trained research staff. After the treating oncologist affirmed that the patient was eligible to participate, patients were approached by bilingual and bicultural (identifying as Latino/Latina) research staff in person during a scheduled clinic appointment (e.g., doctor’s visit, chemotherapy infusion appointment). Of 97 screened, 39 were approached to participate in the study, and 20 patients (51%) provided informed consent and completed semi-structured interviews. Reasons for refusal (n = 19) included: failed to pick up the phone/response calls (n = 8), did not wish to participate in a research study (n = 4), were deemed ineligible (n = 3), did not wish to share feelings (n = 2), was too stressed to participate (n = 1), and was uncomfortable being recorded (n = 1).
Measures and semi-structured interview
Sociodemographic characteristics
Patients’ sociodemographic variables assessed included: age, ethnicity, country of origin, race, gender, education, immigration status, employment, marital status, income, insurance, the language of the interview, format of the interview (in person versus telephone), and primary cancer tumor site.
Prognostic understanding
Patients’ prognostic understanding was assessed using three questions. 3 To examine terminal illness awareness, patients were asked ‘How would you describe your current health status?’ Response options were: (1) relatively healthy, (2) relatively healthy and terminally ill, (3) seriously ill but not terminally ill, (4) seriously ill and terminally ill, and (5) don’t know. Response options were coded as ‘terminally ill’ (2 and 4) and ‘not terminally ill’ (1, 3, and 5). To examine awareness of cancer stage, patients were asked ‘What stage is your cancer currently?’ Response options were: (1) early stage of cancer, (2) middle stage of cancer, (3) late stage of cancer, (4) end stage of cancer, and (5) don’t know. Response options were coded as ‘early/middle stage’ (1, 2, and 5) and ‘late/end stage’ (3 and 4). Finally, to examine awareness of the incurability of cancer, patients were asked ‘Which of the following best represents what your oncology providers have told you about a cure for your cancer?’ Response options were: (1) your cancer will be cured; (2) your cancer may be cured if treatments are successful; (3) your cancer cannot be cured but doctors will try to control your cancer with treatment; and (4) your cancer cannot be cured, and you are not able to have any further cancer treatment. Responses options were coded as curable (1 and 2) and incurable (3 and 4).
Interview process
The present study consisted of mixed methods (surveys and semi-structured interviews). First, patients completed a brief survey designed to assess their demographics as well as their self-reported prognostic understanding. Second, patients participated in an in-depth, semi-structured qualitative interview that asked them about their preferences for the communication of ACP if their illness were to become incurable or progress, including probing for cultural, religious, and familial beliefs influencing prognostic understanding. For this brief report, we will focus on the patient’s perspective on curability and end-of-life treatment decision-making. Methodology and additional reports from other data around ACP communication are reported elsewhere. 12 All interviews were conducted in the patients’ preferred language (English or Spanish) by trained bilingual trained qualitative expert. Interviews lasted 30–45 min.
Analytic procedures
Descriptive statistics
Descriptive statistics provided information on patient demographics, patient clinical characteristics, and patients’ self-reported prognostic understanding. All statistics were reported as means and standard deviations for continuous variables and counts and percentages for categorical variables.
Qualitative interviews
Recorded interviews were professionally transcribed verbatim. English interviews were transcribed and then coded and analyzed. Spanish interviews were transcribed into Spanish, translated into English through a certified forward–backward translation, and then coded and analyzed in English. Transcriptions were uploaded to NVivo 11 software (Lumivero, Dever, Colorado, USA) for analysis. Interview data were analyzed using the six-step protocol for thematic analysis proposed by Braun et al. 27 The first step of thematic analysis consisted of two independent coders reading and rereading the interview transcriptions separately to determine points of potential analytical interest (MS and RP). The second step used key descriptive phrases to code the data individually. The third step involved combining similar codes into themes. When the themes had emerged through the process of grouping similar codes, the fourth step consisted of reviewing and revising the themes to develop a thematic map. This thematic map was co-created by the two independent coders meeting to reach consensus on their individually coded transcripts. In the fifth step, the researchers refined and organized the data in each theme. The sixth and final step involved a final refinement to contextualize the findings in relation to existing theories and studies of ACP and end-of-life care. This final step was done by the lead researcher and trained qualitative coding expert. 12
Results
Patients’ (n = 20) mean age was 56 years (SD = 14.45), 55% were female, and 45% reported being Puerto Rican. Patients’ cancer types included colorectal cancer (n = 10), followed by lung cancer (n = 3), and esophagogastric cancer (n = 3). The language of the interviews were English (n = 10) and Spanish (n = 10) (see Table 1).
Patients’ sociodemographic and clinical characteristics (n = 20).

Prognostic understanding
The majority of patients had inaccurate prognostic understanding. Half of patients (n = 10) inaccurately believed they had an early stage of cancer, 85.0% (n = 17) did not believe their illness was terminal, and 70.0% (n = 14) believed their illness was curable (see Figure 1).
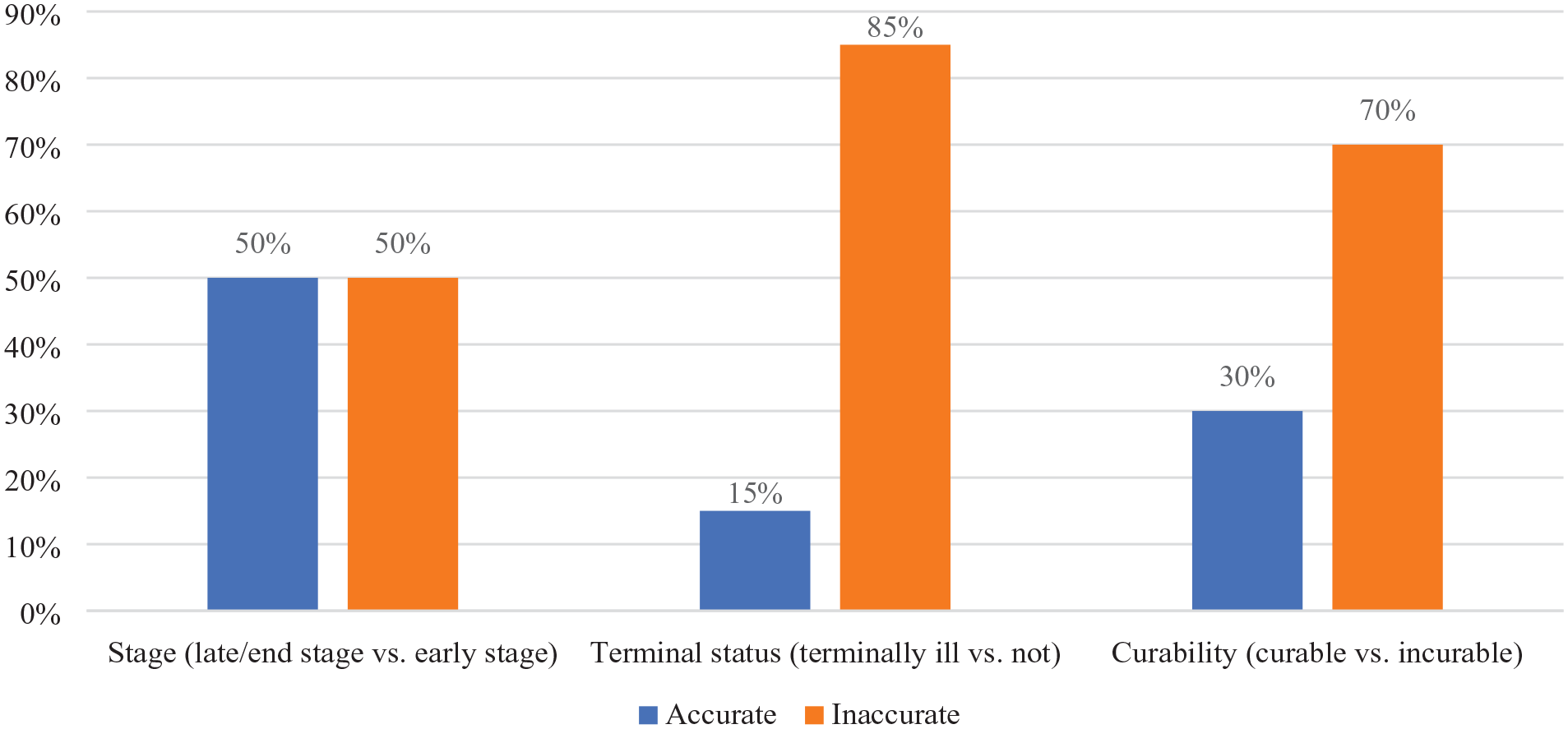
Patients’ self-reported prognostic understanding.
Qualitative themes
Results from these interviews indicated two broad themes: varying levels of awareness of the incurability of their cancer and varying end-of-life care decision-making and treatment preferences based on prognostic understanding. Below are results that emerged from each theme.
Varying levels of awareness of curability
Patients’ awareness of the incurability of their cancer varied and were grouped into two major subthemes: (a) denied (n = 4) or avoided (n = 6) incurability and (b) accepted incurability through integration of beliefs (n = 10). More specifically, patients fell into the following categories: n = 4 of the patients denied that they were incurable (denied); n = 6 patients reported they had not considered the possibility that they might be incurable (avoided), n = 6 patients admitted the possibility that they might be incurable (partial acceptance), and four patients acknowledged and accepted their incurable status (full acceptance). This indicates that patients fell on a continuum from denial to full acceptance of the incurability of their illness (please see Table 2 for more details).
Patients’ attitudes toward their incurable status.

Denial of the incurability of one’s illness was often linked to having faith they would be healed: ‘I have faith I’m going to be healed’ (P11). In other instances, it was linked to an avoidance of thinking about it: ‘My care is still at a curable stage . . . So, we don’t think about it or talk about it’ (P09).
For patients who accepted the incurability of their cancer, this acceptance was linked to clear and direct communication from their oncologist as well as integration of their faith into this understanding.
I accept [that the disease is incurable], because when [doctors] told me about this disease that . . . there would be no cure, I started to become aware and I said, no, I have to accept it and I have to accept it and I have to accept it because God told me that this is it, then this is it. (P05)
Varying end-of-life decision-making and treatment preferences by prognostic understanding
The second theme was broken into two major subthemes: (a) end-of-life decision-making and treatment preferences if patients believed their cancer was curable and (b) end-of-life decision-making and treatment preferences if patients believed their cancer was incurable. Among patients who believed their cancer was curable, they highlighted wanting to prolong their life to spend more time with family (n = 3): ‘I just want to live longer and enjoy my grandchildren’ (P04). Patients also highlighted wanting open and candid communication from their medical providers (n = 7): ‘The important thing is the communication that I have with the doctor . . . Because the doctor has to inform me about how my process is going’ (P05).
This indicates both the motivation to spend more time with loved ones as well as an expressed desire for clear communication about their illness and prognosis (please see Table 3 for more details).
Patients’ most frequently reported current care preferences.

Among patients who believed their cancer was incurable, many focused on the desire for comfort care (n = 9). Specifically, patients often noted a preference for home hospice (n = 4), being as pain free as possible (n = 9), and preference for comfort over life-extending care (n = 9). There was also a focus on wanting to spend final moments with family: ‘I wouldn’t want to die in the hospital. My last days is to be with family, that’s where I would want to be’ (P07). Even when patients mentioned being pain free, there was a central focus on the family: ‘I’d also like, even though life lasts less, but to have no pain. Because that’s the most horrible thing for you, because I felt those pains and they’re horrible. Because you suffer, and your family suffers’ (P10) (please see Table 4 for more details).
Family context.

Connected to this theme was a clear expression of a desire to involve family members in treatment decisions (n = 10): ‘I’d like family to participate. And well, they could give me their opinion, even though the decision would be mine, because I’m the one who would decide what I want’ (P05). Even among those who opted to prolong their life as long as possible (n = 3), they still expressed a clear desire to have their pain managed and controlled: ‘I want to live as long as I can and there is medication to control the pain’ (P07). In some instances, however, the hope to live remained central to patients’ decision-making: ‘If there’s life, there Is hope, there’s a desire to live. There is permanent pain, but I think all pain can be bearable if there is hope for life’ (P17) (please see Table 4 for more details).
Discussion
The objective of this mixed methods study was to explore Latino patients’ perceptions of curability and end-of-life treatment decision-making. Findings indicating that patients had inaccurate prognostic understanding as it relates to the stage of their illness, terminal status, and curability. Two themes emerged from the qualitative interviews: (a) Variability in patients’ level of awareness of the incurable status and (b) variability in end-of-life treatment decision-making and care preferences based on differing levels of prognostic understanding. Findings from the semi-structured interviews highlight that there are two major subthemes of awareness about the curability of one’s cancer: denying or avoiding incurability or accepting (partially or fully) the incurability of one’s disease through direct communication and integration of beliefs. Furthermore, findings highlighted the key roles of direct communication from the oncologist and integrating the family into decision-making each play in the end-of-life care treatment decision-making process. These themes remained central whether patients viewed their illness as curable or incurable.
These findings demonstrate the importance of accurate prognostic understanding and its implication for improving Latino patients’ engagement in end-of-life care planning. Specifically, results from the present study highlight key themes to be integrated into interventions designed to improve prognostic understanding and ACP among Latino patients. Culturally tailored interventions aimed at Latino patients may improve end-of-life care planning, as they show lower rates of engagement in ACP when compared to non-Latino White. 28 First, providers must be aware of patients’ cultural, religious, and other beliefs as they influence patients’ prognostic understanding. 7 Second, oncologists need to engage in clear and open communication about the incurable and terminal nature of patients’ illness, as Latinos are welcoming of providers in their end-of-life discussions and respect their professional opinion.12,29 Third, many Latino patients expressed a clear preference for direct integration of family into their end-of-life treatment decision-making. Expressed preference for family integration is congruent with Latino studies underscoring the familial system and influence in end-of-life care.30–32 Finally, patients’ treatment preferences varied based on their understanding of their prognosis. Studies have shown that when patients misunderstand their prognosis, they also misunderstand their treatment options, leading to an overestimation of life expectancy. 33 As such, it is critical to ensure patients accurately understand their prognosis and that their treatment preferences are assessed.
These findings described the importance of prognostic understanding and are similar to those presented in Costas-Muñiz et al., 10 which suggests that low levels of prognostic awareness may impact Latino patients’ treatment decisions. Some patients who reported denial or avoiding thinking about curability also reported that they do not want to talk about prognosis or ACP, which may lead to failing to plan for end-of-life care. 10 This unplanned end-of-life care highlights several keys to the provision of end-of-life care and the importance of addressing patients’ prognostic understanding, from the diagnostic discussion to the ongoing changes during patient treatment.
Limitations
Despite the many strengths of this study, there are limitations that should be considered when interpreting results. First, the present sample (n = 20) was quite small and consisted of Latinos from multiple backgrounds (e.g., Puerto Rican, Dominican, Mexican), and thus sub-group differences among Latinos could not be examined. It is possible that different sub-groups may prefer and benefit from understanding of prognosis and ACP. Second, the present study was a secondary data, thus no causal inferences can be made. Building off the present study results, however, research should examine how these cultural factors influence various sub-groups within the Latino/Hispanic community around diagnosis understanding and ACP.
Conclusion
These findings suggest that culturally sensitive intervention, which involve patients’ beliefs and their families in decision-making processes, should be designed to improve patients’ understanding and engagement in ACP. Family-centered interventions are important because they recognize the critical role that families play in patients’ care and decision-making processes. 13 By involving families in ACP discussions, healthcare providers can ensure that patients’ goals, beliefs and preferences are aligned with their family’s expectations and values, which can ultimately improve patient outcomes and satisfaction with care. 19
Future research should explore the feasibility and implementation of training programs for healthcare providers to promote diagnosis understanding and communication, as well as training for patients and their caregivers to better understand and discuss their expectations related to diagnosis and care. Such training programs are necessary because they can help healthcare providers and patients/caregivers develop the knowledge and skills needed to effectively communicate about ACP and end-of-life care. By improving communication, patients and their families can make more informed decisions about their care and ensure that their values and preferences are reflected in their care plans.
Supplemental Material
sj-pdf-1-pcr-10.1177_26323524231193038 – Supplemental material for Latino advanced cancer patients’ prognostic awareness and familial cultural influences on advance care planning engagement: a qualitative study
Supplemental material, sj-pdf-1-pcr-10.1177_26323524231193038 for Latino advanced cancer patients’ prognostic awareness and familial cultural influences on advance care planning engagement: a qualitative study by Normarie Torres Blasco, Lianel Rosario and Megan J. Shen in Palliative Care and Social Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.