
Abstract
Objectives:
This pilot project aimed to develop, implement and evaluate a model of care delivered by community volunteers, called Compassionate Communities Connectors. The Connectors’ principal task was to support people living with advanced life-limiting illnesses or palliative care needs by enhancing their supportive networks with Caring Helpers enlisted from the local community.
Methods:
The project was undertaken in Western Australia, 2020–2022. A mixed methods research design incorporated a prospective cohort longitudinal design with two cross-sectional measurements, pre- and post-intervention. The primary outcome was the effect of the intervention on social connectedness. Secondary outcomes were the effect of the intervention on unmet practical or social needs and support from social networks, and the self-reported impact of the programme on social wellbeing such as coping with daily activities, access to formal services, community links, social activity and reducing social isolation.
Results:
Twenty Connectors were trained but 13 participated; 43 patients participated but 30 completed the study. Over half of these patients lived alone and 80% of their needs were in the social domain. There were significant improvements in social connectedness, reflected in reduced social isolation, better coping with daily activities and a two-fold increase in supportive networks. The programme was able to address gaps that formal services could not, particularly for people who lived alone, or were socially isolated in more rural communities that are out of the frequent reach of formal services.
Conclusions:
This project led to an ongoing programme that has been incorporated by the health service as ‘business as usual’, demonstrating rapid translation into practice. It has laid solid grounds for community capacity building with successful measurable outcomes in line with reports on similar programmes. Ongoing work is focused on replication in other communities to help them establish a similar model of care that better integrates formal and informal networks.
Keywords
Introduction
Public health palliative care emphasises community capacity building and holds that all community members have a role in contributing to end-of-life care initiatives. One approach for developing these roles is compassionate communities’ programmes that use community development strategies in volunteering and community engagement. A number of public health programmes have developed new models of volunteering and fresh understandings of the roles that volunteers and community members may have in supporting palliative care services.1–7 Community development strategies build upon the current skills of community members and aim to reduce social isolation by enhancing and supplementing people’s existing social networks. Connector is thus a useful description for this volunteer role, as the volunteers’ focus is upon enhancing or re-connecting relationships within the dying persons’ social networks, recruiting further contributors to those networks, and improving communication between all involved in providing care. There is, however, no generally agreed use of this term, as different projects focus on different sorts of connections.
Public health initiatives do not operate in isolation from or in competition with existing end-of-life care services and strategies but seek to supplement and enhance them. In their ‘new essentials’ model for end-of-life care, Abel et al. 8 propose that a comprehensive model of care should involve the collaborative articulation of four caring sub-systems: specialist palliative care, generalist palliative care, civic action and natural networks. In most healthcare systems, mechanisms are already in place to connect the contributions of specialist and generalist palliative care, even if those mechanisms are often only partially utilised. Civic action can include ‘third-sector’ philanthropic or community-based organisations, but the focus, coordination and reach of these is quite variable, as are their relationships with formal healthcare. Some collaborate well with the healthcare sector and provide some community support but – to generalise – this community engagement addresses individuals more than the informal groups or networks that surround them. Public health approaches tend thus to focus on this gap; on the natural networks in which dying people and their informal caregivers participate, exploring how these networks can be supported or enhanced by resources from the wider community in which they are embedded.
Examples of how these public health palliative care concepts can be operationalised, and the effects of doing so are increasingly available.9–16 In the United Kingdom, for example, the ELSA study 17 found that volunteer befriending services may reduce the rate of decline in quality of life and concluded that clinicians can confidently refer to volunteer services at end of life. A recent Australian study provided insights about the development of local place-based programmes. 18 This research highlighted the significance of collaborations between health and community organisations and found evidence for the important contribution volunteering and volunteers bring to compassionate communities’ work. It also highlighted the need to educate health providers about community-led initiatives and compassionate communities volunteer roles. 19
There is positive evidence emerging from public health palliative care initiatives, including reductions in hospital admissions, 20 reduced loneliness, 21 improved death literacy,22,23 improved intergenerational connections 24 and stronger connections between community members and healthcare services.25,26 However, recent systematic reviews and research collaborations have acknowledged the challenges associated with researching and evaluating public health palliative care initiatives.15,16,27–32 As such, evaluations of community-led initiatives of practical and social support, or those focusing on outcomes involving palliative care volunteers and/or volunteer programmes, are scarce. The Compassionate Connector Program recently trialled in the South West of Western Australia sought to map and mobilise people’s personal and community networks of care. Connectors then enlisted Caring Helpers (community volunteers) to deliver practical and social support to address a variety of needs in the domains of personal care, medical, transport, home, food, social, pets, and preparation for end of life. 1 This article reports on the implementation and evaluation of this model of care.
Objectives
The objectives of this pilot project were to:
Develop, implement and evaluate a model of care delivered by community volunteers, identified as Compassionate Communities Connectors, to support people living with advanced life limiting illnesses or palliative care needs.
Develop and evaluate a training programme for volunteers.
Assess the feasibility, acceptability and potential effectiveness of this compassionate community connector model of care.
This article reports on the quantitative findings of the evaluation of this intervention. Forthcoming articles will report on qualitative findings concerning the experience and satisfaction with the intervention of the three participant groups: patients, Connectors and referring health professionals.
Methods
Ethics
Ethics approval (RGS3419) was obtained from WACHS Human Research Ethics Committee and La Trobe University Ethics Committee. All participants received a participant information sheet and had the opportunity to ask questions about participation before deciding to take part. Participants signed a consent form and received a copy for their own records. If participants decided to withdraw from the study, they were able to do so at any point without providing a reason and without any future care, treatment or employment being affected.
Setting
This project took place in the South West of Western Australia, a region of 24,000 km2 with a population of approximately 170,000. It comprises one regional port town, Bunbury and many smaller rural towns and communities. The project was a partnership between the South West Compassionate Communities Network (SWCCN – www.comcomnetworksw.com), The West Australian Country Health Service (WACHS) (involving the SW Palliative Care Team, The Chronic Disease Team and The Older Persons Initiative), GP Down South Chronic Disease Team and the WA Primary Health Alliance (WAPHA). In terms of the new essentials model outlined above, the partnership involved specialist palliative care, generalist palliative care as provided by chronic disease services, and the civic organisation SWCCN.
Participants
The study involved five groups: patients, their family carers, the Connectors, the Caring Helpers and the referring health professionals.
Patients
Inclusion criteria:
Patients with cancer, chronic obstructive pulmonary disease (COPD), chronic heart failure or renal disease and other chronic conditions such as neurodegenerative conditions.
Patients aware of their advanced illness.
Patients with frequent hospital usage (more than two times in the past 2 months of hospital admissions or emergency department visits) or at risk of hospitalisation for palliative care.
Patients with unmet social, psychological and practical needs.
Patients who are socially isolated and rely on just one other person to meet the majority of their everyday needs.
Patients 18 years and older.
Patients with capacity to provide informed consent.
Connectors
Connectors were community volunteers who provided assistance to the person affected by advanced illness and their family by identifying the additional social and practical support they may require from within their local community and tap into formal and informal sources. Their role was to enhance supportive and sustainable networks around families in need. Names of Connectors who were invited to participate were drawn from the database of attendees of SWCCN educational programmes, anticipating that they would have a moderate level of death literacy because of their prior involvement. Connector selection involved an interview process with members of the project team, which enabled the interviewers to determine the person’s understanding of the role and the project. Connectors underwent reference checks and a National Criminal History Record Check according to the volunteer policies of the health service.
Caring Helpers
Caring Helpers were members of the family, friends, neighbours or other people in the community who were willing and able to assist with specific activities such as walking the dog, doing the shopping, collecting a prescription, transport to appointments, going to the library, mowing the lawn, gardening, making a snack, tidying up or sitting with a person who needs a break. Assistance was provided by Caring Helpers without expectation of payment or other reward or benefit.
Research design
A mixed methods research design incorporated:
A prospective cohort longitudinal design with two cross-sectional measurements, pre- and post-intervention.
A qualitative design using semi-structured interviews with the following groups: The families, the Connectors and the referring health professionals. Findings from interviews will be reported in future articles.
Training of Connectors
Connectors attended a training course of 2 days duration delivered by content experts. As part of the training, Connectors were provided with a training resource that was developed specifically to assist them in understanding their role and what is expected of them. Sessions included information on public health palliative care, the importance of compassionate communities and how this project fits in, death literacy and advance care planning, grief literacy, communication skills, self-care, understanding advanced illness and the role of the palliative care and the chronic disease teams, and the volunteer processes and procedures within the health service. This resource will be made available after further development. A community directory was developed to assist Connectors in pointing participants to community resources. Pre- and post-training evaluation questionnaires were administered to assess changes in Connectors’ knowledge and confidence.
Procedures and data collection
The health service screened and referred interested families and those suitable for the intervention according to the inclusion criteria. The project coordinator visited the referred families to provide an explanation of the project, seek written consent, and collect baseline information on the demographic and clinical profile of the family, their social and practical needs, the availability of supportive networks, and the extent of their social connectedness. The project coordinator then assigned a connector to each referred family, taking into account the profile of the person requiring support, their age and gender, geographical location, personality and the connector’s availability and experience. Outcome measures were collected also post-intervention.
For the purpose of this time-limited research project, Connectors were guided to visit their assigned families or made contact over the phone (text messaging or video calls) a minimum of six times over a 12-week period per family. Some families required more while others required less contact, and this contact continued between most Connectors and families beyond the 12-week data collection period. The Connectors were encouraged to document their contacts using a Network Enhancement Tool (NET), specifically designed for the project, which specified the domains of needs required by their families and the supports they sought to address the needs. There were eight domains: personal care, home, medical, transport, social, food, pets and preparation for end of life. Where some of the Connectors were not comfortable with paperwork, they could phone or email the project coordinator to provide this information following their visit.
The project team facilitated fortnightly 1 h meetings by Zoom with all Connectors, for the duration of the data collection period. Successes and challenges with families were discussed and advice was provided to one another where required. Connectors were also able to access the support of the project coordinator daily as matters arose.
Outcomes and measures
Primary outcome
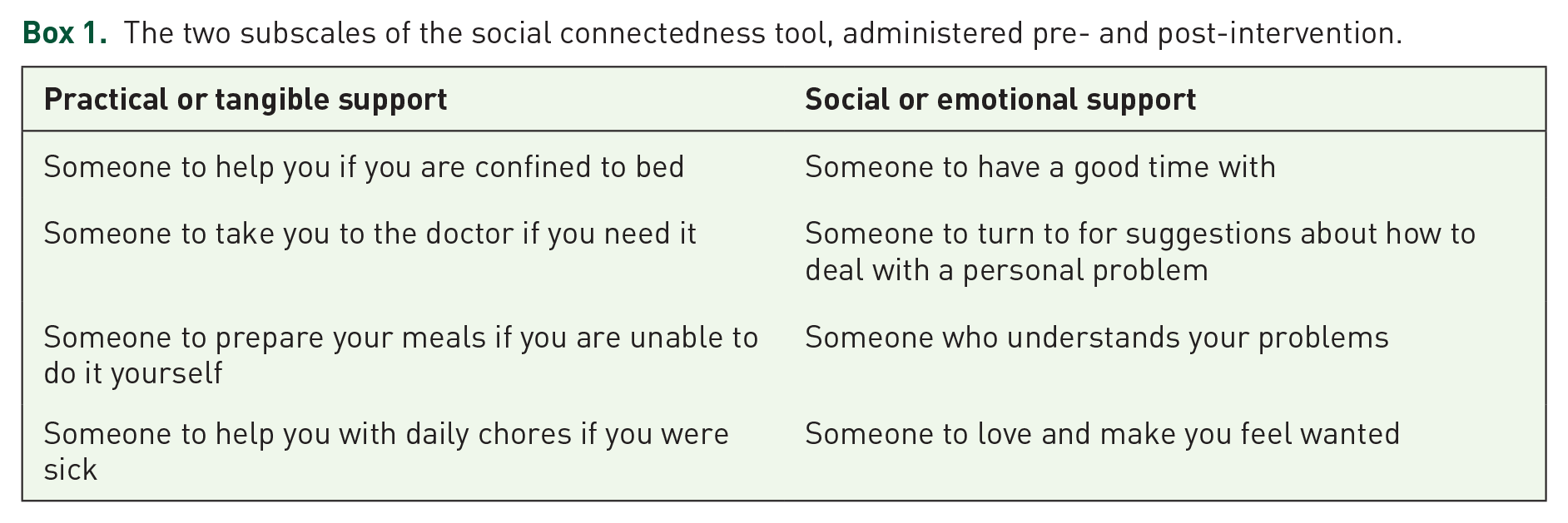
The primary outcome was the effect of the intervention on social connectedness measured by the Modified Medical Outcomes Study of Social Support Survey (mMOS-SS). The mMOS-SS has two subscales covering two domains in social support (practical or tangible and social or emotional) composed of four items, each designed to maintain the theoretical structure of the original 19-item MOS-SS and identify potentially modifiable social support deficits (Box 1). The psychometric properties of the eight-item mMOS-SS were reported to be excellent by Moser et al. 33 Response categories regarding the availability of support for families were: none of the time =1, a little of the time = 2, some of the time = 3, most of the time = 4 or all of the time = 5. The higher the score, the more socially connected are the families.
The two subscales of the social connectedness tool, administered pre- and post-intervention.
Secondary outcomes
The effect of the intervention on unmet practical or social needs and support from social networks was measured by a tool modified from that developed by McLoughlin et al. 34 This tool lists needs in several domains such as personal care, home, medical, transport, social, food and pets. A scale of 0–2 was used to ascertain the extent of unmet needs and networks of support (Box 2). The lower the score, the more dependent on help the person is or the less functional their networks are.
Description of tool on assessment of unmet needs and supportive networks, administered pre- and post-intervention.

The matrix in Figure 1 guided referrals that were high priority to refer to the Compassionate Connectors Program, the medium priority for those who needed to be monitored by the health service and low priority whose suitability needed to be reviewed.

Priority for referrals according to dependency for unmet needs and network of support.
The self-reported impact of the intervention on social wellbeing (coping with daily activities, improved formal access, increased community links, increased social activity and reduced social isolation) was measured by a tool developed for this project. Response categories regarding the impact were: not at all = 1, a little = 2, quite a bit = 3, a lot = 4. Both families and Connectors completed this measure post-intervention. The higher the score, the higher the impact.
Evaluation of the training programme
Nineteen questions tested the Connectors’ confidence in tackling matters of caregiving, dying and grieving that were covered in the training programme, such as ‘please rate how confident you are with the following situations’, using a 5-point Likert-type scale, with the following response categories: 1 = not at all confident, 2 = slightly, 3 = moderately, 4 = fairly, 5 = very confident.
Data analysis
Data were collected and managed by REDCap electronic data capture tools hosted by La Trobe University. 35 Descriptive statistics summarised the quantitative data such as frequencies and percentages, means, standard deviations, medians and ranges. Medians and interquartile ranges were used due to skewed distributions. Changes from pre to post were calculated (post minus pre), with the median difference and their corresponding 95% confidence intervals presented. The p-values were calculated using the non-parametric Wilcoxon signed rank test.
Results
Feedback on training programme and Connector participation
Twenty Connectors undertook a training programme developed for this study and their feedback was positive in terms of the perceived improvement in their confidence to take on such a role. Figure 2 presents the most significant differences in confidence before and after training.

Percentage of Connectors who were very confident pre and post the training programme (p < 0.05–p < 0.001).
However, only 13 Connectors were able to participate (12 females and 1 male) for various reasons related to changes in their personal circumstances, and of these, 9 stayed for the whole duration of data collection period (15 months). Families were followed up by Connectors for a median of 18 weeks, ranging from 3 to 52 weeks. The number of families seen by each connector over the study period ranged from one to nine families, with the average as three. There were 1055 encounters with families and with Caring Helpers that were undertaken by the Connectors during the data collection period, leading to 402 h being spent on the various network-enhancement activities. However, these numbers are an underestimate as not all Connectors have reported this information comprehensively.
Recruitment, attrition and profile of patients
Recruitment of families and data collection took place from July 2020 to April 2022, with a 6-month interruption because of COVID-19, resulting in 15 months of active data collection and access of Connectors to families. Eighty-five families were referred by the collaborating health services, the majority being from the palliative care service, and 43 patients agreed to participate in the study (50% participation rate; Table 1). Reasons provided for declining participation are varied and reported in Box 3, although it should be noted that those who declined were not pressed to explain their decision. However, 30 patients finished the study in terms of completing pre- and post-intervention outcome measurements and undertaking an interview to share their experiences. The 13 participants who could not complete the follow-up either died or were too unwell to do so (30% attrition rate).
Number of patients referred and participated by referral source.

GP, general practitioner; WACHS-SW, West Australian Country Health Service–South West.
Patients who self-referred found out about the programme from a variety of sources, including brochures from (unidentified) service providers, Connectors, family and friends.
Reasons for declining to participate.

Of the 43 patients participating at baseline, 56% were female, average age was 73 years, 47% lived alone, 47% had cancer and 33% had cardiac/respiratory disease. For those who completed the study (n = 30), more of those living alone (57%) and more females (63%) were in the sample (Table 2).
Demographics of patient participants at baseline (n = 43) and at follow-up (n = 30).

SD, standard deviation.
Type and extent of supports needed and type of Caring Helpers providing support
This information was obtained from the NET, which Connectors completed fortnightly or reported to the project coordinator to document on their behalf. Just under 80% of unmet needs were in the social domain followed by home and transport (17–16%), medical (12%), food and preparation for end of life (11%; Table 3 and Figure 3).
Type, frequency and examples of support (n = 238 for multiple responses from 43 patients).

ACROD, Australian Council for Rehabilitation of Disabled; IT, information technology.
This extended to a few families where Connectors wished to continue the relationship during the bereavement phase, although it was not part of the initial brief of the project.

Types of support provided by Caring Helpers and Connectors.
A quarter of Caring Helpers were individual members in the community followed by people from community service groups (18%) that Connectors sourced for tasks like gardening, transport and the various social activities. Sourcing Caring Helpers from the inner circles of these families was less frequent with family (8%), neighbour (6%) and friend (12%; Table 4).
Type of Caring Helpers who supported the patients.

About 26% of Caring Helpers came from naturally occurring networks of the patients (family and friends) and 59% from external networks facilitated by the Connectors (community individuals or groups; Figure 4).

Circles of support facilitated by Connectors (based on Abel et al. 36 ).
Outcomes
Social connectedness
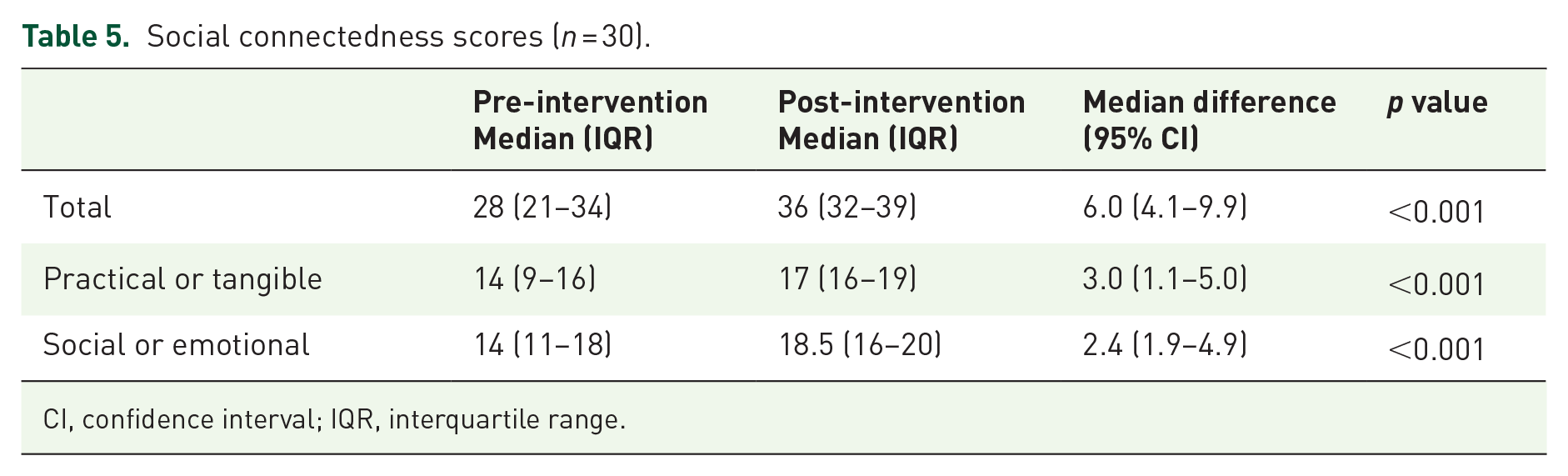
On a total score from a minimum of 8 to a maximum of 40, there was a significant improvement in the primary outcome of social connectedness (p < 0.01) as measured by the validated tool the Modified Medical Outcomes Study of Social Support (mMOS-SS), with a median of 28 at pre-intervention increasing to 36 at post-intervention. The two subscales of practical or tangible and social or emotional support also showed a significant improvement between the two time periods (Table 5).
Social connectedness scores (n = 30).
CI, confidence interval; IQR, interquartile range.
Dependency to meet practical or social needs and availability of supportive networks
On a total score from a minimum of 0 to a maximum of 12, participants had the same moderate to high dependency pre- and post-intervention score (5); however, their supportive networks had improved twofold between the two time periods from low to high functionality to meet their needs (from 5 to 10; Table 6 and Figure 5).
Dependency for unmet needs versus availability of supportive networks (n = 30).


Changes in level of dependency for unmet needs versus availability of supportive networks, before and after the intervention.
Self-reported impact of programme on social wellbeing
On a scale of 1 lowest to 4 highest, the self-reported highest impact of programme on families was in reduced social isolation (3.4), followed by coping with daily activities (3), and increase in community links (2.7). Connectors perceived that the impact of their work on families was also highest for reduced social isolation, although lower than rankings provided by patients for each domain (Figure 6).

Scores of self-reported impact of intervention (n = 30).
Discussion
The programme has been effective in improving social connectedness (primary outcome), reducing social isolation and increasing supportive networks (secondary outcomes). This is echoed by the social unmet needs being the most prevalent for this study group (nearly 80% of total needs). These outcomes should not be underestimated in their importance. Social relationships are a primary determinant of health. 37 The biological mechanism for this, and the evolutionary imperative of social connectedness, are well described, at molecular and immunological levels.38,39 Public health emphasises the importance of social relationships as a positive aspect of people’s lives complementing medical models, which emphasise the treatment of disease and management of symptoms. 40 At end of life, Public Health Palliative Care continues to emphasise the importance of social relationships in supporting quality of life and supporting healthy dying. Horsfall et al. 19 emphasised the central role of community alleviating social isolation, an impact found in our study, and Leonard et al. 41 looked at the impact of engaging communities and found that the size of networks increased during the caring experience, also a finding in our study. Thus, engaging communities in health matters leads to improvements in health and wellbeing, capacity and longer-term community change.
In our study, the majority of support was sourced from the outer informal networks or the community at large (or called externally facilitated networks) rather than from within the inner informal networks of participating families, as depicted in Figure 4 of circles of care. 36 This reflects the fact that over half of the families participating in this study lived alone and hence did not have their own inner informal networks to support them. The programme seems to have filled the gaps that formal services could not, particularly for people who live alone, and those who are socially isolated in more rural communities that are out of the frequent reach of formal services. The activity of network building, using both personal and community resources, works at a practical level to increase participants’ sense of social connectedness.
Social connectedness is also important in mitigating long-term negative consequences that may arise from bereavement. Relationships established during the period of caring for someone who is dying last in the long term.19,42 The evidence provided by Aoun et al. 43 in their population-based survey showed that the most valued aspects of received bereavement support related first to attachment (emotional support), followed by reliable alliance (practical support) and social integration (sense of belonging or connectedness). This support was provided during the bereavement phase by family and friends (90%) who were already involved in the everyday lives of those recently bereaved. 43 The social and physical morbidities of bereavement may be severe, along with increased mortality in the bereaved, particularly those who are socially isolated. 44
A vital component of a public health approach, captured by the new essentials model, is developing a way of connecting and enhancing the informal care networks already present in community life. 8 In the study reported here, links between specialist and generalist primary care services were established through the foundational partnerships of the project. Links between these services and community resources were to be facilitated by the other major partner, SWCCN, which supplied and supported the Connectors. The role of Connectors in this study turned out to be primarily to mobilise support available through civic groups to supplement the reduced resources of many patients’ natural networks. In other circumstances, and for other client groups, Connectors might have found their role focusing on supporting and enhancing existing natural networks, or advocating for civic organisations to pay attention to end-of-life concerns, or representing unmet patient and family end-of-life need to services with the capacity to meet those needs; for example, encouraging chronic disease services to realise their potential as providers of generalist palliative care. This research builds upon the research describing the links between informal and formal care36,42 by examining the impact of this relationship from multiple perspectives and supports the growing body of international research and evaluation reporting the outcomes of compassionate communities.6,7
When estimating the intervention impact on the social wellbeing of families (Figure 6), it is interesting to highlight that the Connectors seemed to have underestimated the impact of their work in all five domains, while the families have perceived benefits that were greater than the Connectors’ ratings. This finding is consistent with previous research that found that informal care networks tend to underestimate the impact of their support to carers. 19 Palliative care volunteers have been identified as the ‘lynchpin’ between formal and informal care 2 and are considered an essential part of hospice and palliative care workforce. 45 It is interesting that even in the community connector model, volunteers do not fully appreciate the positive impact that informal support has for people who are dying and their family carers. This intangible care provided through the actions of ‘being there’ and the ‘linking’ needs continual highlighting from policy makers and volunteer managers. 46
The training programme seemed to have prepared the Connectors well for their role. As the programme progressed and we acquired more learnings, the training programme became even more tailored to Connectors’ needs using real experiences or scenarios to discuss with a new group of Connectors. The training programme was just the foundation as the learning continued through the fortnightly Zoom meetings. As there was an interest from Connectors to keep following families into bereavement, a more expanded grief literacy training will be incorporated in future training sessions.
Recognition for this relatively short-term initiative was manifested by the connector programme being a finalist in the Palliative Care Awards 2021 competing with well-established hospices in the category of ‘outstanding regional/rural team delivering holistic palliative care and/or a compassionate community approach in any setting’. As a consequence of the success of the programme, the Compassionate Connectors Model of Care has been adopted by the health service (WACHS) as ‘business as usual’ (BAU). This meant that the Connector initiative has moved from being a time-limited project to being absorbed into BAU functions of WACHS with the potential to be scaled up by both SWCCN and WACHS. This is a clear example of a rapid translation into practice. While the workforce compliance components required by WACHS are absorbed into the existing hospital volunteer programme, the Connectors also fall under the SWCCN governance and risk management, models discussed in our previous publication. 4
Strengths and limitations
Public health palliative care interventions, such as this community-based intervention, are implemented in real-world settings, which are complex systems in which to undertake research, and so present a challenge to traditional research methodologies. 47 However, with the mixed methods approach we have employed, and the balance between using a validated tool for the primary outcome and other pragmatic tools to measure the perception of participants of the impact of the programme, the reported quantitative findings in this article point to the success, feasibility and viability of this model of care. The interviews undertaken with the participant groups reinforced these quantitative findings and will be reported in a forthcoming article.
What we have realistically aimed for, as outlined in the published protocol article, 1 was achieved in terms of at least 10 Connectors and 30 families participating and completing the study. Given the exploratory nature of this study, our conservative estimates were based on the relatively small size of the initial study population (about 100 palliative care patients), on what was feasible within the initial data collection timeframe of 10 months (stretched to 15 months because of the pandemic), and on the need to find enough families willing to participate (50% participation in this study) and then be able to complete the study (30% attrition in this study). Half-way through the data collection period, it became apparent that recruitment needed to be supplemented from other patient groups who have a chronic or life-limiting illness but are not too close to end of life (four additional services as per Table 1). As palliative care patients may have been referred quite late to the palliative care team, their subsequent referral to the Connector programme was often too late to pursue network enhancement, and many were lost to follow-up through death or feeling too unwell, challenges that are well reported in the literature. 48 An added challenge of the pandemic was that the enforcement of vaccination status by the health service led some Connectors, who did not at that stage wish to be vaccinated, to exit the programme. It should also be noted that there are challenges to generalisability due to the small number of participants in this study.
Only 15 family carers agreed to participate out of a possible 23 for those patients not living alone – 14 carers were spouses and one a daughter. In general, family carers participated with patients in completing the pre- and post-outcome measures and interviews as a family unit. However, future research may need to focus solely on the needs of family carers and promote it as such so carers do not feel they are competing with the needs of patients, a challenge encountered in previous research. 49
The research-related paperwork was always not welcomed by consumers and service providers 49 and may have discouraged some families and Connectors from signing up at the start or continuing with the programme. Families needed to sign consent forms, and respond to questionnaires, albeit brief ones, at the start and end of the intervention. The majority of Connectors did not like completing the one brief tool (NET) on needs of families and Caring Helpers they sourced for these needs. One workable solution was for the project coordinator to reach out to the Connectors after their visits and collect the necessary information from them by phone or by e-mail. We anticipate as the programme moves forward, without the research component, these administrative challenges will greatly diminish.
Conclusion
This project has provided the evidence that such Compassionate Communities Connector models of care are effective in improving social connectedness. Moreover, it demonstrated the viability of a working relationship between informal community networks and formal health networks, mediated by the Connectors. The COVID-19 pandemic has demonstrated the importance of local networks of care and the understanding of the Compassionate Communities Connectors approach to care thus gained is relevant and timely, given the need for community capacity building in the wake of the pandemic.
This trial has tested procedures for applicability and feasibility and appraised the likely rates of recruitment and retention of participants that need to be considered in future studies or larger trials. If more or larger communities participate in a research study that could achieve a larger sample size, then other outcomes would be possible to measure such as the impact on health service utilisation using a control group and economic effectiveness.
This pilot project has laid solid grounds for building community capacity, enhancing health services capacity and potential replication into other communities, with successful and realistic measurable outcomes, which are in line with what is reported in the international literature for similar programmes. Ongoing work is focused on rolling out the Connector training to a number of interested communities in other geographical regions to help them establish a similar model of care, meaning further programme applications and better integration of formal and informal services.
Footnotes
Acknowledgements
This project was supported by the Western Australian Health Translation Network and the Australian Government’s Medical Research Future Fund (MRFF) as part of the Rapid Applied Research Translation, and also by Perron Institute and La Trobe University.
Special acknowledgement to the staff who engaged in this initiative from the following partner organisations: The WA Country Health Service (WACHS) (involving the SW Palliative Care Team, The Chronic Disease Team and The Older Persons Initiative), GP Down South Chronic Disease Team and the WA Primary Health Alliance (WAPHA)
Special thanks to the Connectors whose passion, altruism and dedication were key to the success of this initiative. The authors are grateful to the families who agreed to give it a go despite their difficult circumstances and to their Caring Helpers