
Abstract
Background
Very few studies have been done to evaluate bone healing in odontogenic keratocysts (OKCs) after surgical treatment along with 5-fluorouracil (5-FU) application.
Purpose
To evaluate bone healing following treatment of OKC with enucleation, peripheral ostectomy, and 5-FU using cone beam computed tomography (CBCT) at 6 months and 1 year postoperatively. Secondary objectives were to evaluate recurrence after 6 months and 1 year and to evaluate complications.
Study Design, Setting, and Sample
Prospective observational study on 20 patients with biopsy-proven OKCs in a tertiary care government hospital was conducted.
Predictor/Exposure/Independent Variables
Age, gender, number of cysts, side involved, chief complaint, syndromic or not, cystic dimension in cm3, teeth involved, bone density in Hounsfield units (HU), teeth extracted, nerve involvement, and use of prophylactic intermaxillary fixation.
Main Outcome Variables
Primary outcome variables were size of cavity and bone formation in HU. Secondary variables were recurrence and incidence of postoperative complications.
Covariates
Demographic covariates included age, gender, side involved, and chief complaint. Radiographic covariates were the preoperative size of the lesion in cm3 and the cortical breach evident on CBCT. Operative covariate was inferior alveolar nerve involvement.
Analyses
Wilcoxon signed rank test, P value < .001.
Results
In total, 20 patients were included. Four patients were lost to follow-up after 6 months. Mean age of patients was 32.3 ± 10.4 years with a male-to-female ratio of 3:2. Median (interquartile range, IQR) density of lesions on the unoperated side was 374.61(251.69-529.49) HU. Median (IQR) density values of lesions preoperatively, 6 months, and 1 year postoperatively (N = 16) were 1.35(−39.21 to 24.68) HU, 169.31(72.61-290.26) HU, and 378.31(141.33-559.83) HU. Recurrence rate was 0%. Mean (visual analog scale, VAS) values on days 1 and 7 and 1 month postoperatively were 3.9 ± 1.8, 1.75 ± 1.68, and 0.4 ± 0.94. There was a 40% incidence of sensory disturbance at 1 month and 15% at 6 months and 1 year; 70% incidence of dehiscence, 25% infection, and 5% each for osteomyelitis and pathologic fracture.
Conclusions and Relevance
Bone density was comparable to that of unoperated normal bone at 1 year postoperatively. No recurrence was noted. Theoretical concerns for 5-FU, being an antimetabolite with possible negative effects on bone remodeling, make these study results relevant.
Keywords
Introduction
Odontogenic keratocyst (OKC) is a benign uni- or multicystic, intraosseous tumor of odontogenic origin, with a characteristic lining of parakeratinized stratified squamous epithelium and potential aggressive, infiltrative behavior (WHO). 1
In a systematic review and meta-analysis conducted by Al-Moraissi et al. 2 using pooled data of 2,989 patients included in 40 studies, recurrence of OKCs was evaluated. It was shown that 5-fluorouracil (5-FU) directly competes, rather fares better than even the resection modality.
The identification of the role of the Hedgehog (HH) signaling pathway in the tumorigenesis of various cancers, including basal cell carcinomas, led to the hypothesis that HH signaling pathway inhibitors could be a potential therapy for patients with Nevoid Basal Cell Carcinoma Syndrome (NBCCS) who frequently presented with multiple basal cell carcinomas and OKCs. 3
Following the observation that 5-FU results in a downregulation of the HH signaling pathway by acting as a thymidylate synthase inhibitor in hepatocellular carcinoma, the investigators hypothesize that the HH-inhibiting action could also be used to treat syndromic and sporadic OKCs. 4
According to earlier studies, no recurrence of OKC was noted with a mean follow-up time of 3 years when post enucleation, 5% 5-FU was coated in ribbon gauze and placed in the cystic cavity for 24 hours. Only a few patients developed transient nerve paresthesia, which resolved after 42 weeks. 5
The purpose of this study was to evaluate the efficacy of 5-FU as an adjuvant to enucleation and peripheral ostectomy in the treatment of mandibular OKC. The specific aims of the study were to evaluate bone healing following treatment of mandibular OKC with enucleation, peripheral ostectomy, and 5-FU using cone beam computed tomography (CBCT) and orthopantomogram (OPG) at 6 months and 1-year postoperative period. Secondary objectives were to evaluate the recurrence rate after 1 year using panoramic radiographs, CBCT, and clinical evaluation and to compare the incidence of other postoperative complications.
Materials and Methods
A prospective observational study was conducted with the study population including all patients treated for OKCs in our unit using 5-FU from February 2022 to March 2023. The study was initiated after obtaining ethical clearance from the Institute Ethical Committee under the registration number: IECPG-118/24.02.2022 and RT-39/24.03.2022.
All biopsy-proven cases of OKCs aged 18-65 years treated in the department were included. Recurrent cases of OKCs, patients not giving consent for follow-up, and patients with a systemic disease affecting bone healing were excluded. Pathologies with a span necessitating resection as a treatment plan were also excluded. Pregnant patients and nursing mothers were also excluded from the study.
A detailed case history of the patient was taken. Preoperative nerve status was assessed using subjective evaluation along with cotton wisp tests. Preoperative pain was assessed using the visual analog scale (VAS). All routine preoperative investigations, including complete blood cell count, liver function test, renal function test, coagulation profile, viral markers test, and blood sugar tests, were performed. The lesion was assessed preoperatively using OPG and CBCT scans for its size, extent, borders, and influence on surrounding structures using Materialise Mimics software. After the patient was cleared for surgery, informed written consent was obtained for both the planned surgical procedure and enrollment in the study.
Baseline variables, including age in years and gender, were noted. Preoperative nerve paresthesia was checked and documented as yes/no. Side involved was noted as left, right, or bilateral. The cortical breach, as evident on CBCT, was checked, and Hounsfield units (HU) were calculated on the same.
The surgical procedure was initiated under general anesthesia, after preparation of the surgical site in an aseptic manner. Crevicular incision was given along the teeth on the side of the lesion, along with anterior and posterior releasing incisions. The mental nerve was carefully preserved. A subperiosteal dissection was carried out to expose the lesion. The involved teeth were extracted atraumatically. A bony window was created using a bur and rongeurs to create an opening into the cystic cavity. The cystic lining was enucleated, and peripheral ostectomy was done. The surrounding bony margins were smoothened. Copious irrigation was carried out with saline water. Hemostasis was achieved. The bony cavity was then dried thoroughly. In total, 5% 5-FU cream soaked in roller gauze was applied in the cavity left after enucleation, with a small part of it extruding out of the suture site. Closure was done using 3-0 Vicryl sutures. The 5-FU-coated gauze was kept in place for 24 h after the procedure. After 24 h, it was removed from the cavity. The cavity was irrigated with saline through the opening formed after the removal of the roller gauze. A suture (3-0 Vicryl) was placed under local anesthesia to close the opening. The patient was kept under observation. One representative case is shown in Figures 1-6.
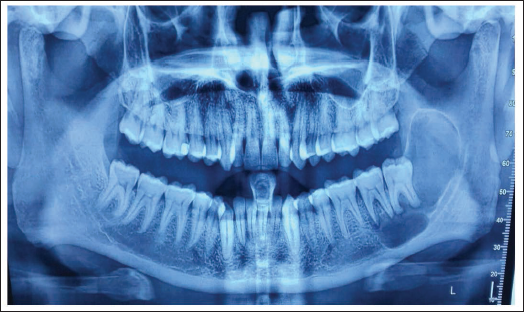
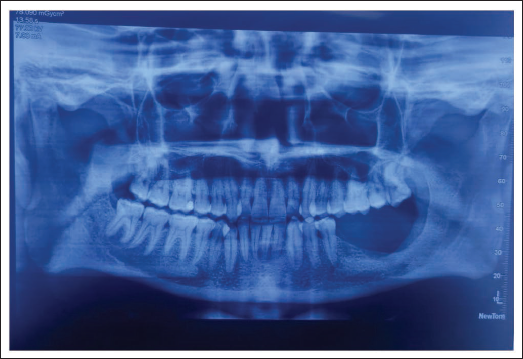
Preoperative Orthopantomogram.
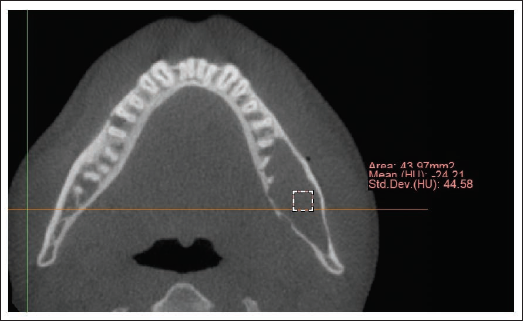
Preoperative Cone Beam Computed Tomography (CBCT) Scan.
Postoperative Orthopantomogram at 6 Months.
Postoperative Cone Beam Computed Tomography (CBCT) Scan at 6 Months.
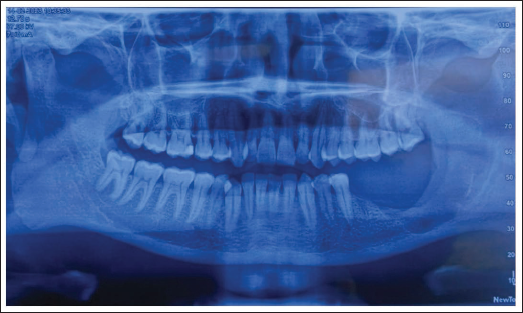
Postoperative Orthopantomogram at 1 Year.
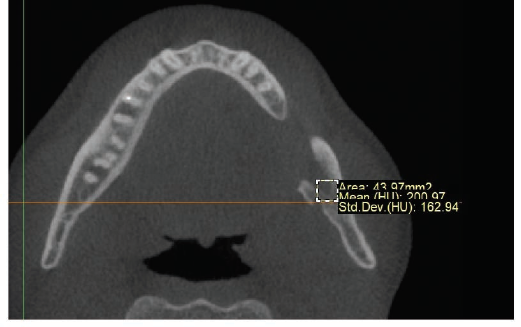
Postoperative Cone Beam Computed Tomography (CBCT) Scan at 1 Year.
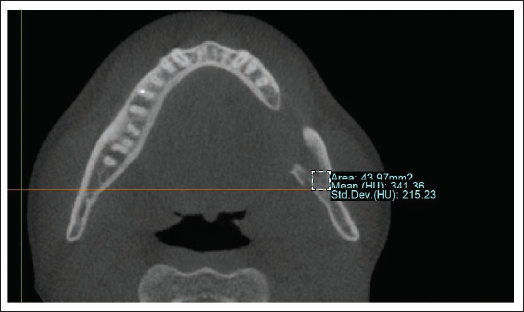
Postoperative care was initiated by a pressure dressing placed for 24 h postoperatively. No drain was placed. Intermaxillary fixation (IMF) was done for 4 weeks if the remaining bone at the lower border of the mandible was less than 1 cm or if there was radiographic evidence of pathologic fracture. Oral hygiene maintenance was reinforced. For all the patients, Tab Amoxicillin + Clavulanate 625 mg BD was prescribed for 5 days, Tab Aceclofenac + Serratiopeptidase + Paracetamol TDS for 5 days, rescue pain medication of Tab Ketorolac SOS, and Tab Pantop 40 mg once a day (OD) × 5 days. Patients were recalled post 7 days, 1 month, 6 months, and 1 year for clinical evaluation. OPG scans were taken at immediate postoperative, 1 month, 6 months, and 1 year postoperative periods. Additionally, at 6 months and 1 year, CBCT scans were taken and assessed. Materialise Mimics software was used, and bone density was measured on the lesion using a rectangle of area 43.97 mm2. It was compared to the opposite side at the same level and same site.
Primary outcome variables assessed were HU as calculated on CBCT scan using Materialise Mimics software. Secondary outcome variables, including pain (VAS), dehiscence (yes/no), infection defined as purulent discharge from suture site with or without systemic signs (yes/no), and nerve paresthesia (yes/no), were assessed using subjective symptoms and cotton wisp test and documented at each visit. Recurrence defined by reappearance of discharge/swelling coupled with radiographic evidence of an increase in size of radiolucency from a similar radiograph taken at a prior follow-up visit was also looked for.
The data were analyzed by STATA software version 16.1 (StataCorp, College Station, Texas, USA). The Wilcoxon signed-rank test was used for statistical analysis. A level of P < .001 was considered statistically significant.
Results
One patient had a bilateral lesion in the mandible and was excluded from the sub-analysis comparison of the parameters of bone densities between operated and unoperated sides after 1 year.
There were a total of 20 patients enrolled in the study who were allocated to the same treatment modality (enucleation of the lesion, peripheral ostectomy, and chemical cauterization using 5-FU) under general anesthesia.
In terms of demographic data, the mean age of the total patients enrolled in the study was 32.3 ± 10.4 years (mean ± SD). There was a slight male predilection among the enrolled patients, with 12 males and 8 females. The ratio of males to females was 3:2. The majority of the patients in the study presented with the chief complaint of pain due to periodontal involvement of the lesion (8 patients, 32% of the cases). Six patients (24%) had pus discharge as the reason for seeking treatment, other 6 patients (24%) had swelling, and for 5 patients (20%), it was an incidental finding on radiographs. Right-sided lesions were encountered most frequently, constituting 11 patients (55% of cases). In total, 8 cases (40%) had involvement of the left side and 1 patient had bilateral involvement. The average preoperative size of the lesion was 32.3 ± 10.4 mm2. The majority of the lesions had no involvement of the inferior alveolar nerve canal, including 16 cases (80%), while 4 patients (20% of cases) had inferior alveolar nerve involvement. A breach in the cortex was noted in 15 cases (75%), and both the cortical plates were intact in the rest 5 patients (25%). The median (interquartile range, IQR) density of the lesions preoperatively for patients included in the study (N = 20) was 15.59 (−35.44 to 27.87). All the preoperative variables are summarized in Table 1. No complications were encountered intraoperatively in any patient.
Baseline Parameters for Participants Included in the Final Analysis.
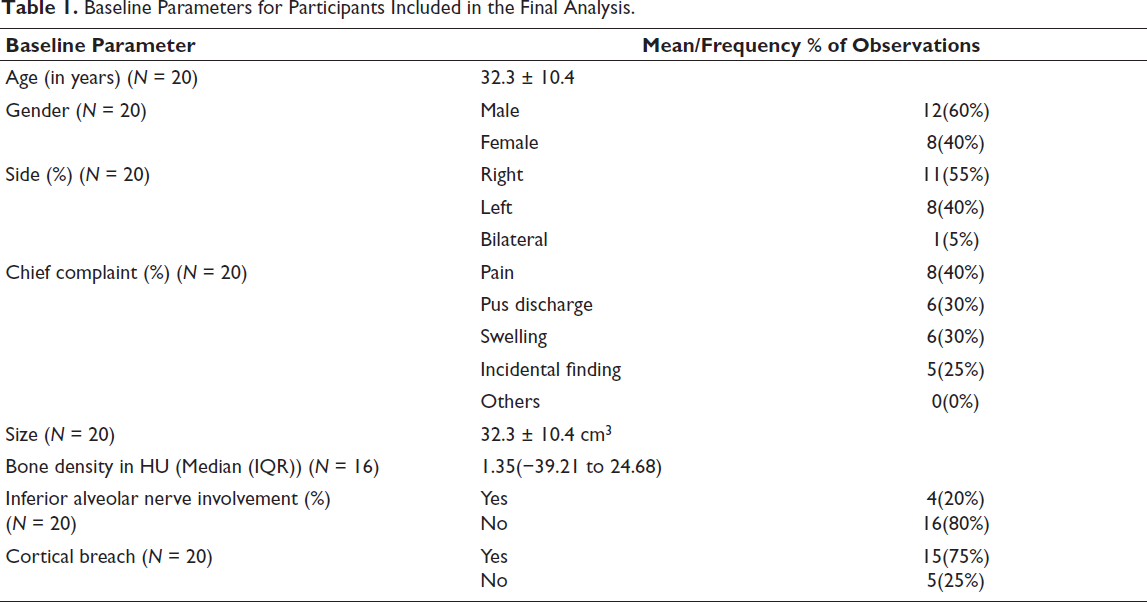
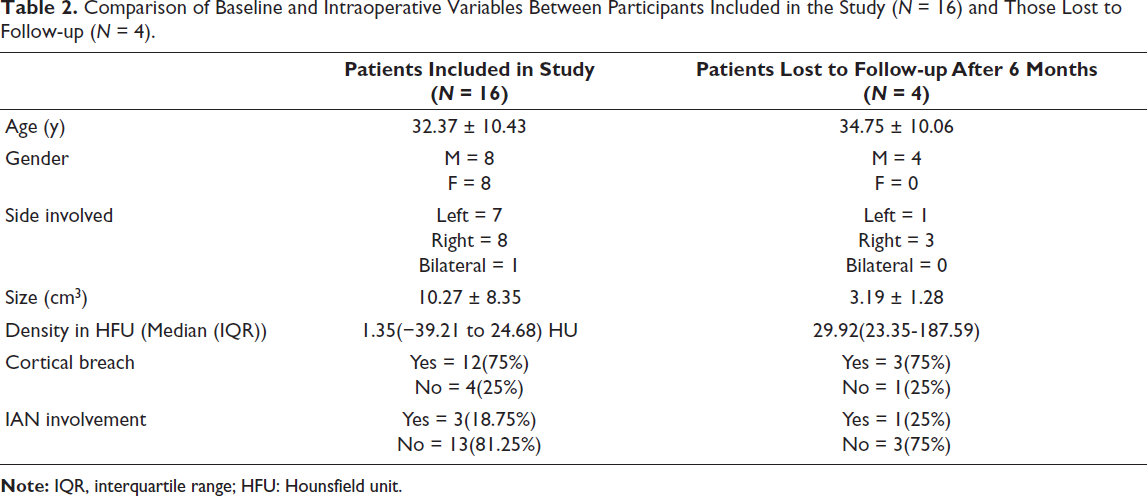
Four patients were lost to follow-up after 6 months due to personal reasons. All baseline parameters for participants included in the final analysis are summarized in Table 1. A comparison of preoperative and intraoperative variables between participants included in the study and those lost to follow-up after 6 months has been summarized in Table 2.
Comparison of Baseline and Intraoperative Variables Between Participants Included in the Study (N = 16) and Those Lost to Follow-up (N = 4).
The mean pain score on the first day following surgery was 4.06 ± 1.88 (VAS). On postoperative day 7, mean pain scores were 1.87 ± 1.69. One month postoperatively, mean pain scores were 0.25 ± 0.75 (Table 3). Dehiscence was the most frequently noted postoperative complication with 14 cases (70%). Five patients (25%) showed signs of infection postoperatively, nearly 7 days postoperatively, with pus discharge, swelling, and pain. All were managed by betadine irrigation, local dressing, and obturators. One patient developed osteomyelitis post 6 months of treatment and was managed by local curettage and antibiotics. One patient had a pathological fracture of the mandible 2 months postoperatively and was treated by open reduction and internal fixation (ORIF) with reconstruction (2.4 mm Synthes Plate). Eight patients (40%) had inferior alveolar nerve paresthesia at 1 month postoperatively. Three patients (15%) had persistent inferior alveolar nerve paresthesia post 6 months. None of the patients showed any signs of recurrence on OPGs and CBCT scans, both 6 months and 1 year postoperatively (0%).
Postoperative Variables at the Various Follow-up Intervals.
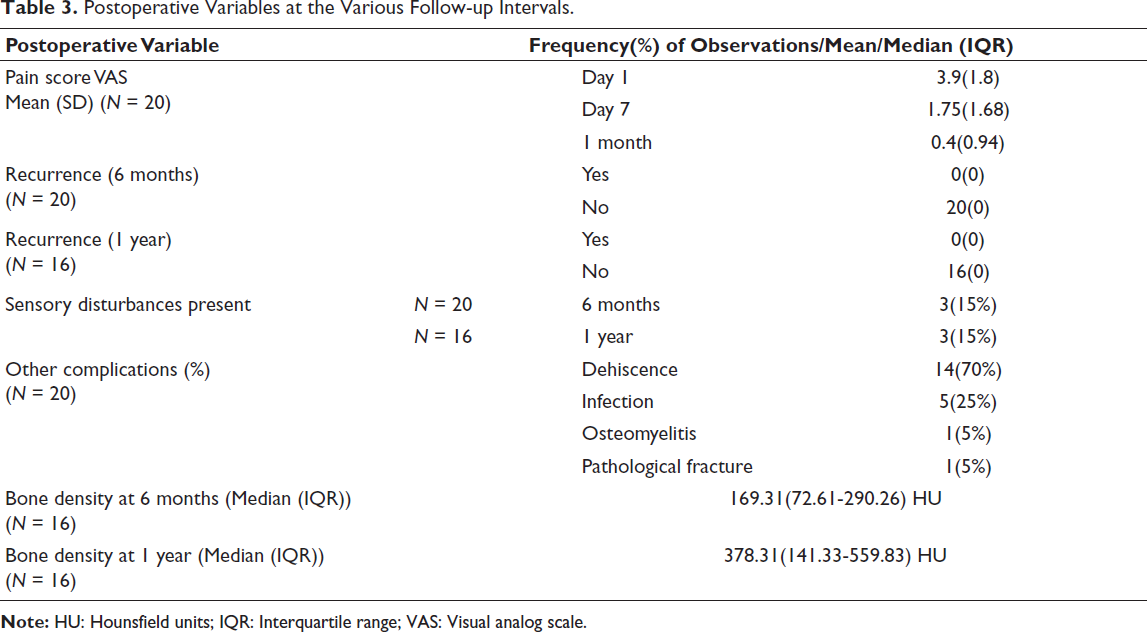
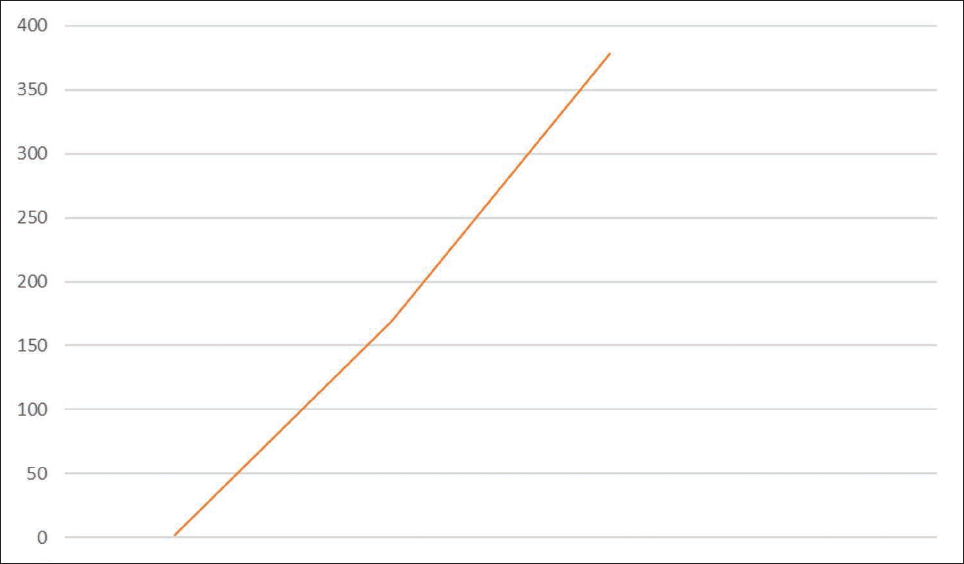
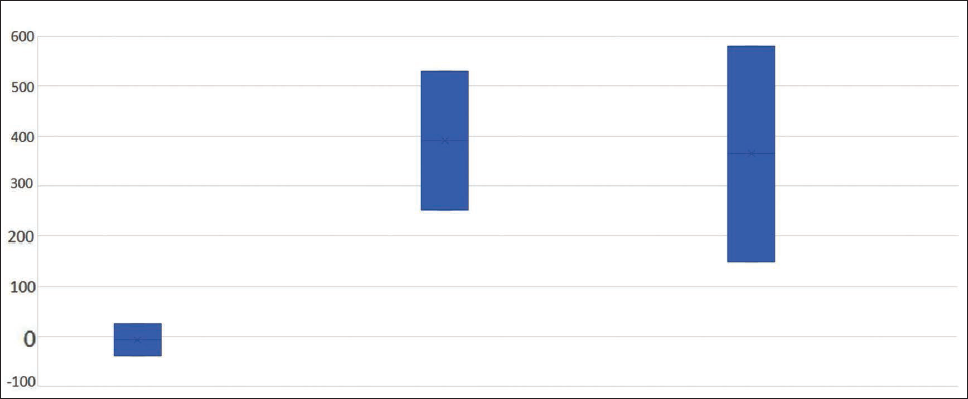
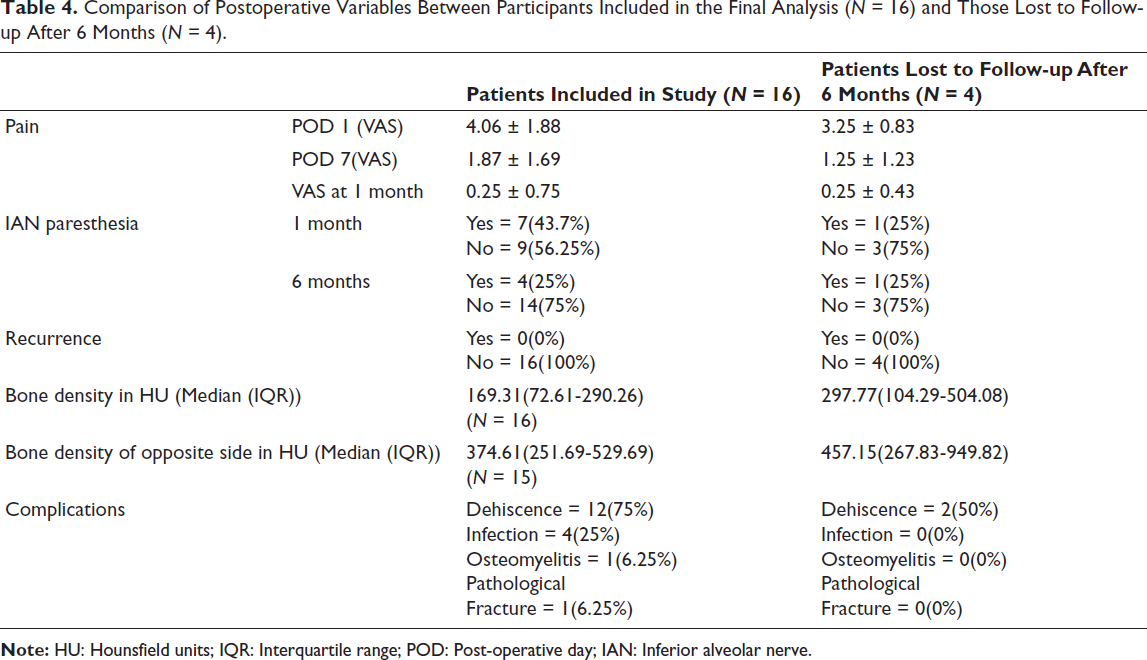
The median (IQR) of density of the lesions after 6 months (N = 16) was 169.31(72.61-290.26) HU. The median (IQR) of density of the lesions after 1 year (N = 16) was 378.31(141.33-559.83) HU (Figure 7). Since one patient had bilateral lesions, patient was excluded from the comparison of bone density on the unoperated side versus the operated side at the 1-year follow-up visit. The median (IQR) of the density of the unoperated sides after 1 year (N = 15) was 374.61(251.69-529.49) HU. Comparison of these 15 unilateral lesions that turned up at 1 year is shown in Figure 8. All the postoperative parameters have been summarized in Table 3. A comparison of postoperative variables between participants included in the final analysis (N = 16) and those lost to follow-up after 6 months (N = 4) is given in Table 4.
Comparison of Median Bone Density in Hounsfield Units (HU) at Preop, 6 Months, and 1 Year in Patients with Complete Follow-up (N = 16).
Comparison of Median Hounsfield Units (HU) Preoperatively, 1 Year Postoperatively on Unoperated, and Operated Sides (N = 15).
Comparison of Postoperative Variables Between Participants Included in the Final Analysis (N = 16) and Those Lost to Follow-up After 6 Months (N = 4).
Comparison of preoperative, postoperative 6 months, and 1 year CBCT bone density in HU of study subjects with complete follow-up (N = 16) is given in Table 5.
There was a statistically significant difference (P value < .001) between radiographic density preoperatively, after 6 months, and 1 year postoperatively. There was no statistically significant difference (P value = .7615) between radiographic density of the operated and unoperated sides after 1 year.
Comparison of Preop and Postop 6 Months and 1 Year Cone Beam Computed Tomography (CBCT) Bone Density in Hounsfield Units (HU) of Study Subjects with Complete Follow-up (N = 16).

IQR: Interquartile range.
Discussion
There are various treatment options for OKC, which historically have included marsupialization, 6 enucleation followed by peripheral ostectomy (usually with a rotary handpiece and bur), marsupialization followed by enucleation, marsupialization followed by excision of overlying mucosa, and curettage. 7 They are associated with recurrence rates of 25%, 36.7%, 48.1%, 6%, and 36.7%, respectively. 8 Other treatment modalities are resection and the use of cryotherapy and chemical adjuvants like 5-FU. Resection includes two types: segmental resection and marginal resection. 9 Cauterization can be of two types as electrical and chemical. Chemical cauterization is done by the use of a chemical agent (Carnoy’s solution/MCS). 10 In enucleation with cryotherapy, a gel is placed into the bony cavity and frozen with a cryoprobe crystallizing water in the cells of the bony cavity wall, thereby disrupting and lysing them after enucleation of the entire lesion. 11 It is associated with a recurrence rate of 53.9%. 8 5-FU is the newest adjuvant, which is being tested in the present study to assess radiographic bone healing and for recurrence rate.
All patients in the present study were comparable in terms of demographic data, presenting complaints, and the absence of any comorbidities affecting healing. Confounders, such as smoking, bone healing ailments, and recurrent lesions, were excluded so that postoperative outcomes could be better related to the treatment in question. Similarly, all patients were followed up on day 1, post 7 days, 1 month, 6 months, and 1 year to evaluate trends in bone healing, recurrence rate, postoperative pain, nerve paresthesia, and any adverse events.
The mean age of patients included in our study was 32.3 ± 10.4 years with 60% males and 40% females, which is comparable to the study by de Castro et al. 6 The mean preoperative size of the lesions was 32.3 ± 10.4 cm3, which was slightly smaller albeit comparable to those in the study by Zhao et al. 12 Bone density according to a study by Zhao et al. was 1.35(−39.21 to 24.68) HU, which was smaller compared to the study by Zhao et al. 12 ; however, their study result was falling within IQR of the present study. The involvement of the inferior alveolar nerve canal was seen in 20% cases, which was slightly larger, and cortical involvement in 25% cases, which was smaller compared to the findings of Ac et al. 13
In postoperative outcomes of our patient population, dehiscence was the most common complication (N = 14; 70%). Dehiscence may be caused by the cavity postenucleation being packed with roller gauze coated with 5-FU placed with a 1-inch gauze extending out of the cavity, leading to a portal of entry for microbes and subsequent infection and dissolution of sutures. Post pack removal, the bone cavity acts as a closed space, which may lead to blood and fluid serving as a medium for microbial growth leading to dehiscence. 14
Pain scores were low postoperatively (mean VAS on day 1 being 3.9). It may be due to the 1-inch gauze left out of the cavity acting as a drain for the exit of blood and fluid, thereby reducing pain. 15
In our study, immediate postoperative nerve disturbances were noted in eight cases, which may be due to the cellular-damaging effects of 5-FU leading to neural cytotoxicity; however, there can be other factors like retraction and mechanical trauma, which may be responsible. In a study done by Jo et al., 16 the invasion size of the cyst was significantly associated with sensory dysfunction. In a prospective cohort study done by Akhter et al., 17 no permanent nerve paresthesia was observed in lesions treated by enucleation and treatment by 5-FU. In a prospective study done by Ribeiro et al., 18 neuropathy postenucleation in OKCs was related to direct contact between the solution used and epineurium. However, at the last follow-up, only 3 out of 16 patients were having paresthesia. The rest all had regained sensations.
Osteomyelitis was observed in one case postoperatively. The patient was a known case of Gorlin-Goltz syndrome and hypothyroidism, which are documented to influence healing rate.19, 20
A pathologic fracture was observed in one patient. The bone remaining at the inferior border for the patient postenucleation was very less, leading to increased susceptibility to fracture. The patient was also partially edentulous, hence, postoperative IMF could not be used effectively to decrease fracture incidence. 21 The same was treated with a 2.4 mm reconstruction plate, and at 2 years, the patient is being planned for dental rehabilitation after bony healing.
Till the time of publication of these results, nearly 2 years postoperatively, no recurrence has been reported, and patients are under follow-up as per usual protocol for odontogenic lesions, which extends up to 20 years postoperative. These favorable results with relation to recurrence are in accordance with a study by Caminiti et al. 22 Low recurrence rates may be due to the exposure time to 5-FU of 24 h, leading to a sustained and prolonged effect. 5-FU is also a very effective antimetabolite, leading to cellular DNA damage, followed by cell damage and interfering with cell division. 5
The median (IQR) of density of lesions preoperatively for patients included in the study (N = 16) was 1.35(−39.21 to 24.68) HU, at 6 months 169.31(72.61-290.26) HU, and 378.31(141.33-559.83) HU at 1 year postoperatively. A prospective study was conducted by Akhtar et al. 17 to assess bone healing of cystic cavities postenucleation and treatment with 5-FU. The bone healing was better, and the recurrence rate was nil compared to patients treated with modified Carnoy’s solution and those treated by segmental resection. Considering the need for postoperative rehabilitation of patients after surgery using fixed/removable prosthesis, the significant bone healing seen after topical application of 5-FU for treatment of OKCs becomes relevant. It may be due to the cytotoxic effect of 5% fluorouracil sparing the tissue fixative effects of solutions like Carnoy’s solution, which may lead to less damage to the vascular supply of the area leading to better nutrition for the osteoblastic and fibroblastic cell lineages. 23 This in turn leads to better and faster bone and tissue healing. 24
Another finding came into our observation that the median (IQR) of density of bone at the operated sites post 1 year (N = 15) was 412.65(150.07-579.72) HU, which was higher than at the opposite unoperated side (N = 15), 374.61(251.69-529.49) HU. According to a study by Ma et al., 25 the bone remodeling process is influenced by osteoclast-derived apoptotic bodies. Mature osteoclast-derived apoptotic bodies (mOC-ABs) induced osteogenic differentiation of mesenchymal stem cells and facilitated osteogenesis via RANKL reverse signaling. 5-FU, by inhibiting thymidylate synthase enzyme and damaging cellular DNA, induces cell apoptosis. 5 This may also affect the osteoclasts, which will lead to increased formation of mOC-Abs, leading to more osteogenic differentiation of mesenchymal stem cells and thus improved osteogenesis. Solutions, such as Carnoy’s solution, on the other hand, cause tissue fixation, leading to cross-linking and coagulation between proteins. 26 This leads to defective formation of mOC-Abs. Hence, the use of 5-FU in addition to preventing the recurrence of OKCs may also lead to accelerated bone formation, leading to better rehabilitation of these patients. However, the confounder of the inference that 5-FU is causing increased bone density in the postoperative period is that the majority of our cases had wound dehiscence, and they required iodoform dressings extending for 3-4 weeks. The effect of iodoform on bone healing, as suggested by the literature, was significant since it acted as an antiseptic, which promotes healing by asepsis. 27
Conclusion
Barring the small sample size and short follow-up period, enucleation, peripheral ostectomy along with chemical cauterization using 5-FU was found to be a very effective treatment modality for the treatment of OKCs and at 1 year postoperative period showed excellent bone healing on CBCT scans. The treatment definitely merits future large-scale studies and incorporation into routine practice.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Necessary ethical clearances and informed consent were received and obtained, respectively, before initiating the study from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.