
Abstract
This report discusses the case of a failed root canal treatment in the right mandibular first molar, which exhibited a chronic periapical pathology in its distal and mesial roots. The tooth was managed surgically by periapical curettage and apicoectomy. This approach is indicated in teeth having periapical pathosis which does not resolve by routine endodontic treatment. The aim of periapical curettage is to make the apical periodontium and root canals of the treated tooth free of bacteria and their products. With the advancements in magnification, armamentaria, and materials, the ease of operation and success rate of apicoectomy have underwent a significant improvement. The treated case showed a complete resolution of clinical symptoms and the periapical pathology, thus substantiating the effectiveness of this treatment approach.
Introduction
During the late 19th century Black 1 described the root-resection technique or amputation of the root apex, as an alternative to dental extractions, for the management of “pyorrhoea alveolaris” complicated by a dental abscess. The first reported procedure which may be considered a primitive form of periapical surgery was performed in 1846, on a 14-year-old male, when access to the root of one of his teeth was gained by drilling away areas of inflamed/infected tissue with a trephine and a bur mounted on the dental engine. 2 In the subsequent years, pioneers of the apicoectomy technique started using a more radical approach by completely removing the root end. They applied 95% phenol on the gingiva and scraped away the inflamed tissue (dental abscess) until the bony covering of the root apex was exposed to the action of trephine and straight burs.1, 2
Total debridement and appropriate obturation of the root canals form the basis of an efficient Root canal treatment. 2 Incomplete obturation, root perforations, coexistent periodontal/peri-radicular lesions, grossly overfilled or overextended canal fillings, developing apical cysts, inadvertently removed silver points, and broken instruments are some common causes of root canal treatment (RCT) failure. 3 Broken files and root canal filling materials extending to the periapical region elicit a foreign body reaction in the surrounding connective tissue. The resultant immune reaction either tries to absorb the foreign body or to surround it with a fibrous capsule, the latter being a more frequent observation. 4 This response plays a major role in determining the prognosis of the endodontically treated teeth. 5
When such a foreign body or a bacterial colony lies beyond the root apex, it may give rise to a self-sustaining extra-radicular lesion. RCT failure resulting from such lesions is either managed by orthograde root canal retreatment or by apical surgery. 1 Therefore, in the present case a combination of endodontic re-therapy and apical surgical intervention was carried out in order to manage a failed RCT. 6
Case Report
A 37-year-old male patient reported to the Department of Periodontology; Faculty of Dental Sciences King George’s Medical University, Lucknow, with a chief complaint of intermittent, dull, gnawing type of pain in the right lower back region of his jaw. The patient also reported undergoing RCT at a private dental clinic for treating caries in his right mandibular first molar, when he experienced sudden, sharp, throbbing pain in the same tooth, two years back. On examination, no swelling or pus discharge was noted. Also, there was no tenderness on percussion. Periodontal examination revealed no significant findings. A provisional diagnosis of improper root canal treatment was made. Upon radiographic evaluation, periapical radiolucencies were noticed in both the mesial, as well as the distal root. Among the two radiolucencies, the bigger lesion was present in relation to the distal root (Figure 1A). The patient first underwent orthograde retreatment and a possible requirement for surgical intervention, was explained to him, followed by a written consent obtainment. After gutta-percha (GP), removal, thorough cleaning of the root canals was carried out (Figure 1B). The canals were then obturated with mineral trioxide aggregate (MTA), followed by a temporary filling.
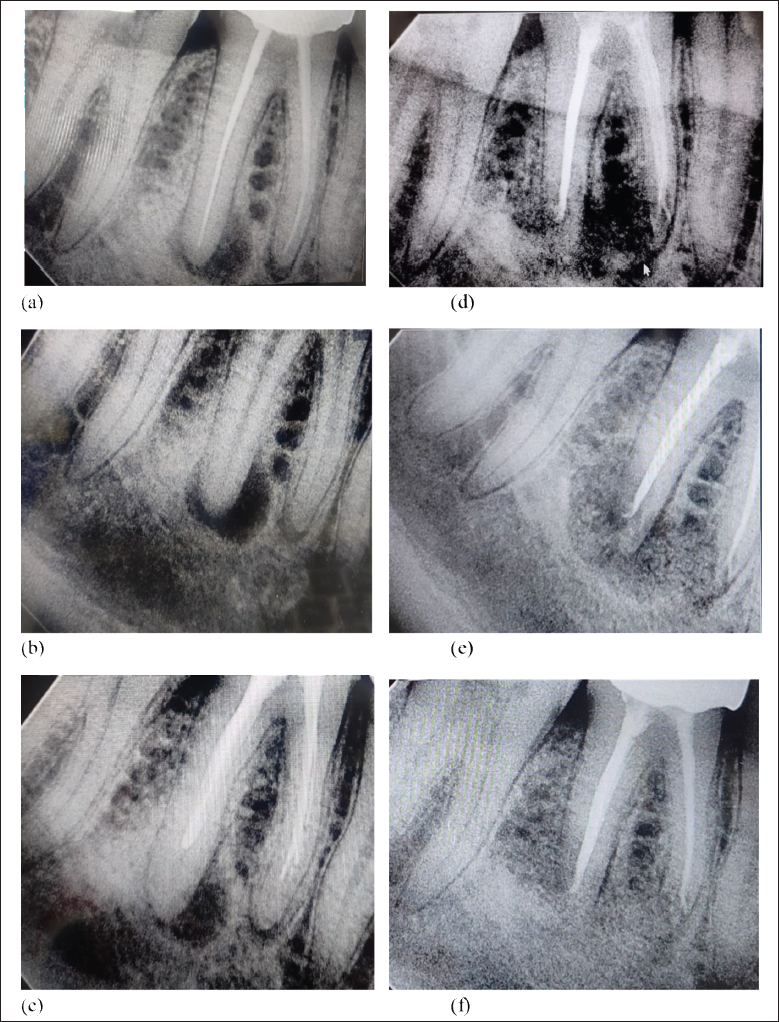
A week later, the patient was recalled and subsequent follow-up was done over a month (Figure 1C). On recall visits, the patient was asymptomatic, but no signs of periapical healing could be noted radiographically.
These observations warranted the need of surgical intervention, in order to remove the peri-apical lesion. A full-thickness, triangular mucoperiosteal flap was raised, with the incision extending from the distal aspect of the second premolar to the mesial aspect of the mandibular second molar. Flap reflection revealed a bone loss in the apical area, corresponding to root apices of 46 (Figure 2A).
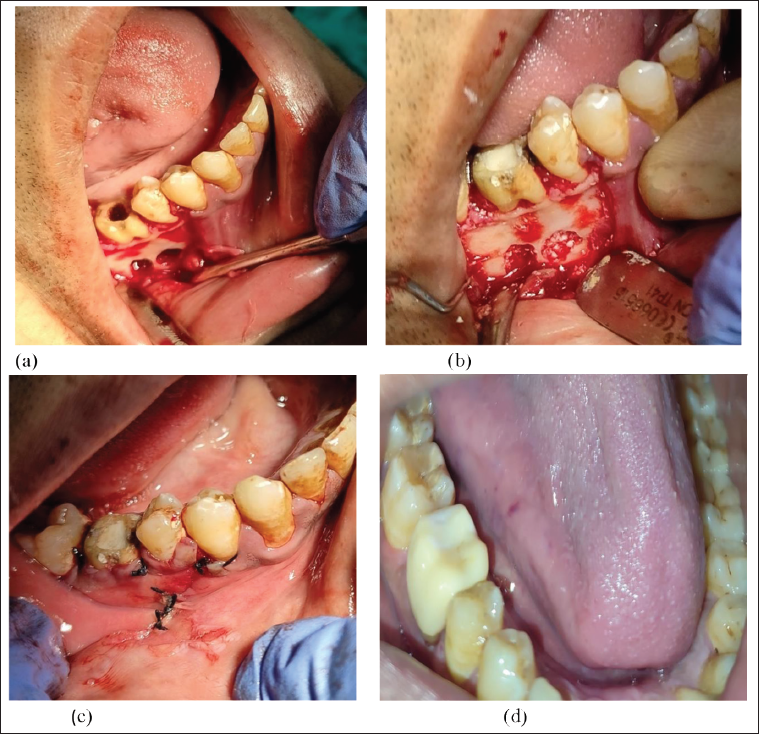
Needful enlargement of the defect access was done to reach the apices and 3 mm of both the root ends were resected. The defect was then curetted to get rid of the granulation tissue and any possible foreign body residues, after which the root canals were retro-sealed. A radiographic evaluation was also carried out (Figure 1D). Then a Xenograft was placed inside the bony cavities around mesial and distal root apices (Figures 1E & 2B). Finally, interrupted sutures were given after flap re-approximation (Figure 2C). Suture removal was done after a week, and the patient was recalled on follow-ups. The follow-ups demonstrated complete clinical and radiographic healing. A post-endodontic restoration was then done with a full coverage crown after three months (Figures 1F & 2D).
Discussion
The removal of diseased granulation tissue, along with root end-resection and retrograde sealing of the root end constitute the essential components of peri-apical surgery. Additionally, a bone graft material may be placed at the site of the defect, to enhance new bone formation. Some examples of root end-filling materials are GP, glass ionomer cement, amalgam, and composite resins. Overfilling of the root canal, a common iatrogenic complication of RCT, deteriorates the prognosis of endodontic therapy. 5
MTA is a remarkable root end-filling material. 7 It was introduced to dentistry in 1993 by Torabinejad et al. It shows commendable sealing ability and promotes osteoblastic activity. While being less cytotoxic than other root-end filling materials, it displays reliable antimicrobial properties. Also, bridges of cementum tend to form over MTA-filled root ends, confirming the cementogenic properties of this material.8–10
A root-end filling material is placed to prevent any communication between the peri-radicular area and the root canal. 11
On the other hand, the most used material for obturating root canal spaces is GP. Biocompatibility of pure GP has been confirmed in in vitro studies.
Commercially available GP points contain 20% of GP, and 60%–70% zinc oxide (ZnO) . They can be cytotoxic, particularly due to zinc, as it may affect the neighboring soft tissues. 12 Cytotoxicity was confirmed in scanning electron microscopic analysis. It can induce peri-radicular inflammation and/or necrosis of the periodontal ligament, and for this reason, overfilling should be avoided as much as possible because it can lead to failure of root canal therapy in the long run. 5
Endodontic surgery has recently improved, with the rates of success crossing 90%. Apparently, the patient’s sex, age, and tooth type, tend to carry no effect on the treatment success.13, 14 The positional relationship of the mandibular canal and molar apices was studied by Littner et al., and they concluded that the mandibular canal usually lies 3.5–5.4 mm below the first and second mandibular molar root apices. 15 In our case, the inferior alveolar canal was about 8 mm away, providing a safe area for periapical curettage and apicoectomy.
Conclusion
Prevention is undeniably the most ideal cure of an iatrogenic error, but once occurred, it must be managed with utmost robustness. Mandibular molars often pose a challenge for periapical periodontal surgery because of their closeness to the inferior alveolar branch of the mandibular nerve. Also, accessibility poses a challenge to the operator, when working in this region. However, if one goes with a systematic approach, periapical lesions in this region can be managed efficiently, eventually yielding excellent results in terms of pathosis healing and symptom resolution.
Author Contributions
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.