
Abstract
Along with functional periodontal health, esthetic demand is increasing among patients. Creating a perfect smile through periodontal plastic procedures or multidisciplinary approaches involving orthodontic, restorative, and prosthetic specialties is a real challenge in esthetic dentistry. “Black triangle” is one of the common causes that can compromise esthetic. Black triangle is open gingival embrasure cervical to interproximal contact. Its presence may also cause problem in phonetic and retention of food debris. This article discusses the definition, causes, classification, prevalence, and various approaches in handling the case of black triangle.
Introduction
In the last few years, people have become very conscious of facial aesthetics. Earlier, restoring functional periodontal health was the prime concern, but the current generation gives too much importance to their esthetics. So along with functionally stable occlusion, patients frequently ask for an esthetically pleasing smile, and the periodontists are trying their best to advance the esthetic dentistry. Esthetically pleasing smile depends on gingival display and color of gingiva, contour of lips, tooth color, size and position, occlusal level, etc. So, the causes of unesthetic appearance may be:
Gummy smile Hyperpigmentation of gingiva Gingival recession Gingival enlargement or abnormal contour of the gingiva Open gingival embrasure Abnormal overjet or overbite
One of the described factors that can compromise a perfect smile is the presence of “black triangle,” an open gingival embrasure formed when the embrasure apical to proximal contact point is not filled by interdental papilla. As its presence in esthetic zone can lead to cosmetic deformities, and there is enhanced awareness of beauty and esthetic, it is important to treat black triangle. Also, its presence may cause a problem in phonetic and retention of food debris. 1 So, it can adversely affect periodontal health. 2
Definition
“Black triangle” is defined as embrasures cervical to the interproximal contact that is not filled by gingival tissues. 3
Out Line on Interdental Papilla
The interdental papilla is composed of overlying oral epithelium and dense connective tissue. The shape of interdental papilla depends on the distance between adjacent teeth, their contact points, surfaces, and cementoenamel junction (CEJ) level. 4 “Cohen” first described the morphology of interdental papilla. 5 The tip of papilla lies just below contact point; it is pyramidal and narrow in anterior whereas flatter (buccolingual) in molar region.
The Common Causes of Open Gingival Embrasure
Loss of attachment because of periodontal disease
Aging
Traumatic oral hygiene
Abnormal tooth shape
Improper contour of restoration
Postorthodontic alignment
Gingival biotype
Root angulation
Factors that Affected Height and Shape of Interdental Papilla
There are various factors responsible for the presence or absence of papilla and their height and shape. They are as follows
Osseous Architecture
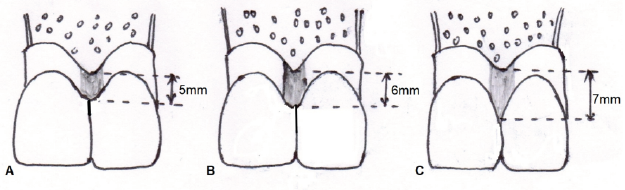
Osseous crest, which follows the shape of cementoenamel junction, impacts the shape and form of interdental papilla. Ochsenbein gave the term “positive architecture,” in which the position of interdental bone is more coronal than radicular bone. 6 According to Tarnow et al, 7 there is a 98% probability of the completely filled papilla type embrasure, when 5 mm or less distance is present between alveolar crest and cervical contact point, while at 6 mm at crest to contact, this probability drops to 56%, and when the distance is 7 mm, only in 27% cases the embrasures were completely filled (Figure 1). 7
When the Distance from Crest of Bone to the Apical Contact Point is 5mm or Less, there is 98% Probability of the Embrasure with Completely Filled by Papilla. While at 6mm at Crest to Contact, this Probability Drops to 56% and when the Distance is 7mm, only in 27% Cases, the Embrasures were Completely Filled.
Distance Between Adjacent Teeth
Tal 8 examined the prevalence of intrabony defects with interproximal distance and concluded that morphology of osseous portion of an intrabony lesion may be determined by interdental distance. It means there may be correlation between health of interdental papilla and interdental distance. Other study 9 also concludes that the presence and the shape of papilla depend on horizontal space dimension between approximating teeth.
Role of Periodontal Tissue Morphology
Periodontal Biotype
Ochsenbein and Ross first introduced the “gingival biotype” to describe the variation of gingival contour. Later Seibert and Lindhe gave the term “periodontal biotype,” which categorized gingival contour into “thick” and “thin.”
10
The thin periodontal biotype is friable, whereas the thick biotype is fibrotic and resilient, so they are more resistant against pocket formation and recession following surgical procedures. The factors that contribute to the thick biotype, a superior characteristic, are as follows:
Thick biotype has high collagen and intracellular matrix volume to prevent collapse and constriction. Keratin stratification prevents bacterial access and physical trauma. Thick biotype has more vascularity that enhances oxygenation, excretion of toxic products, and release of growth factors facilitating good healing.
Periodontal Bioform
Different scalloped morphologies of gingiva are because of periodontal bioforms. Different bioforms are:
Normal: if the distance between interproximal gingival tip (most coronal) and the midfacial free gingival margin (FGM) peak (most apical) is 4 mm.
High scallop: if the distance is >4 mm.
Low or shallow scallop: if the distance is <4 mm.
Hence, scalloped gingiva or periodontal biotype can be categorized as high, normal, and flat/low. 11
Underlying bony architecture determined the scalloped gingival morphology because interproximal gingival contour follows it. In shallow gingival scallop, the interproximal bone is thin, and in flat scallop, there is a congruous relationship between bone and FGM, this type of bioform is less prone to recession following surgery. In high scallop, interproximal bone is wider and incongruity between bone contour and FGM, there are chances of recession creating black triangle and compromised esthetic. For favorable esthetics, a flat scallop is better than a high or pronounced scalloped.
Shape of Crown
There are basic crown forms: circular, square, or triangular crown morphology also affects the shape and form of interdental papilla. Triangular crown yields pronounced scalloped gingival form and predispose to black triangular (as discussed earlier). In square, interdental papilla maintenance is better because of wider contact and smaller interproximal distance from osseous crest to the contact point.
Contact Point
In maxillary anterior teeth, the form and shape of the interdental papilla depend on the contact points and their distance from the bony crest. Tarnow et al 7 described “5 mm rule.” If the distance from interproximal bony crest to contact point is 5 mm less, the gingival embrasure is completely filled with interdental papilla, or if the range is 1 mm to 5 mm, then chance of complete filling is progressively reduced by 50%. But for square-shaped teeth, the possibilities of black triangle are minimal because of narrower and more coronally positioned contact points.
Classification
Nordland and Tarnow classified the loss of interdental papilla into 4 categories (Figure 2). They used 3 reference points: Contact point, facial apical extent of CEJ, and interproximal CEJ (iCEJ) 12 :
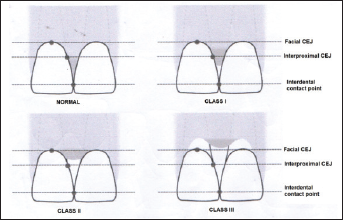
Normal: Interdental papilla fills embrasure completely.
Class I: Tip of papilla lies between the contact point and the most coronal extent of CEJ.
Class II: Tip of the papilla lies at/or the apical to iCEJ but coronal to facial CEJ.
Class III: The tip of the papilla lies at level with or apical to the facial CEJ.
Jemt described a papillary index 13 to clinically degree of regeneration and recession of papilla adjacent to single implant restoration through clinical and photographic examination.
Score 0: No papilla is present
Score 1: Less than half of the height of papilla is present.
Score 2: More than half of the papilla is present, but the entire proximal space is not filled with papilla.
Score 3: The papilla fills up the entire proximal space.
Score 4: Papilla is hyperplastic.
Prevalence
Black triangle is more frequently seen in adult patients with bone loss (more than one-third of adults). 14 Study found black triangle in 18% of the population below 20 years of age and in 67% of the population above 20 years of age. It has been found that dissatisfaction among patients with black triangle is quite high. Patient’s attitude to black triangle with aesthetic defects ranks third following carious or dark crown margins. 15
Management of Black Triangle
Soft tissue or periodontal morphology depends on the underlying bone architecture. So, management of black triangles emphasizes restoring the lost interproximal soft tissue, but complete restoration is not achieved if the recession of interdental tissue is because of bone loss. If the recession is mainly because of soft tissue lesions, reconstructive techniques may be useful in restoring papilla.
Management of black triangles might be as follows:
Nonsurgical approach Periodontal approach Orthodontic approach Restorative approach Prosthodontic approach Surgical approach Papilla recontouring Papilla preserving Papilla reconstruction
Nonsurgical Approach
Periodontal Approach
Papilla can be restored completely by reepithelialization of traumatic lesions.
If the loss of papilla height is only because of soft tissue damage from oral hygiene devices, then it must be discontinued to allow papilla to regrow, then successively interproximal cleansing means should be modified in order to eliminate/minimize injury to papilla.
16
Curettage is done every 15 days interval for 3 months to recreate papilla that has been destroyed by necrotizing gingivitis.
17
It will induce a proliferative hyperplastic inflammatory reaction. Regeneration of interdental papilla occurs after 9 months of the first curettage. Some papilla shows complete regeneration, but 100% of cases don’t respond to periodic curettage. Injecting hyaluronic acid (HA) gel preparations into interdental papilla reduces the black triangle height. In most studies, authors have proposed approximately 0.2 mL of HA gel injection directly into the middle of papilla (2 mm to 3 mm apical to tip of papilla) following local anesthesia. Then, the gentle message of that area for 1min is recommended. This treatment should be repeated at 21 days and then at 42 days. After each treatment session, postoperative instructions should be given to the patient that includes: Discontinuation of mechanical plaque control in the area for first 24 h. Use of a soft toothbrush after first 24 h. Reconstitution of routine mechanical oral hygiene after 2 weeks.
Restorative/Prosthetic Approach
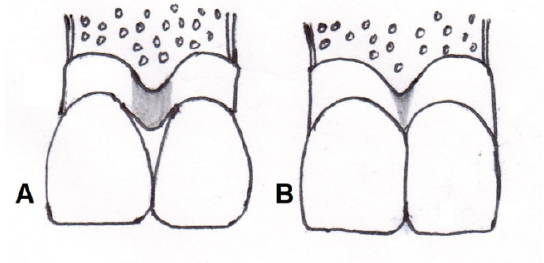
Abnormal tooth shape may cause low level of papilla. The deficient papilla and open gingival embrasures can be corrected by restorative or prosthetic approach. By restorative reshaping or prosthetic approach, contact point may be lengthened apically to the tip of papilla to close the space (Figure 3). These approaches are noninvasive; however, there are some disadvantages, such as food impaction, increased bacterial growth.
(A) Excessive Large Embrasure as the Contact Point is more Coronal; (B) Shape of Crown has been Changed, Contact Point Lengthened to Tip of Papilla.
Orthodontic Approach
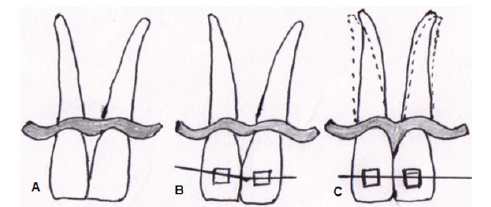
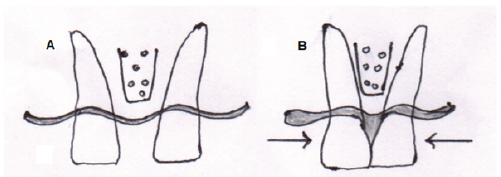
Divergent roots are sometimes associated with abnormal embrasure, creating black triangle. This can be corrected orthodontically by changing root inclination. This approach is to reduce embrasure by placing the contact point more apically (Figure 4). However, bodily tooth movement is needed in case of presence of diastema (Figure 5).
(A) Divergent Roots; (B) Orthodontic Treatment; (C) Convergent Roots.
Closure of Diastema and Papilla Regeneration. (A) Prior to Treatment; (B) Closure of Diastema with Formation of an Interdental Papilla Fills an Empty Space.
Surgical Approach
Several surgical techniques have been described to solve black triangle by reconstructing interdental papilla.
Papilla Reconstruction
Specific techniques have been proposed to reconstruct papilla, such as pedicle flap, semilunar coronally repositioned flap, envelop type flap, autogenous osseous, and connective tissue graft.
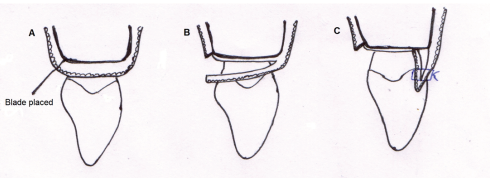
Beagle (1992) 18 described a pedicle graft procedure utilizing the soft tissues palatal to the interdental area. Following split thickness flap on palatal aspect of the interdental area, flap is elevated labially, folded, and sutured to create the new papilla at the facial part of the interdental area. The flap was elevated, folded, and sutured facially to create a new papilla (Figure 6).
(A-C) Papilla Reconstruction: Pedicle Graft Technique.
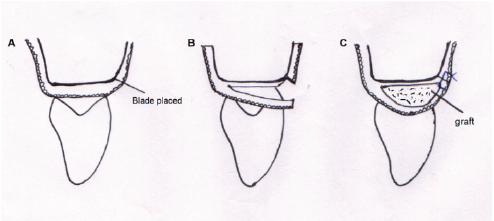
Han and Takei (1996) 19 proposed an approach for papilla reconstruction based on the use of a free connective tissue graft. A semilunar incision was placed on the facial aspect of interdental area, and a pouch was created to receive the graft. Intrasulcular incisions were placed around adjacent teeth to free connective tissue from root surfaces to allow coronal displacement of the interdental soft tissue. Connective tissue graft was taken from palate and placed into the pouch to support coronally positioned papilla (Figure 7).
(A-C) Papilla Reconstruction: Semilunar Coronally Repositioned Papilla Technique.
Papilla Recontouring
To eliminate excess tissue in presence of gingival enlargement, gingivectomy may be performed to reshape papilla. In case of a localized gingival lesions, such as peripheral giant cells granuloma, gingivectomy followed by reconstruction of papilla is indicated.
Papilla Preservation
Surgical approach that splits papilla contributes to shrinkage and decrease in height of interdental papilla, leading to exposure of interproximal embrasure. Specific surgical approaches have been developed to spare the papilla instead of splitting it. Thus, apical displacement of the gingival margin following treatment of periodontal defects can be minimized.
In papilla preservation flap, sulcular incision is placed in facial aspect of each tooth. Interdental papilla is not dissected. Sulcular incision along palatal aspect is then placed. Semilunar incision is made across each papilla; interdental papilla is elevated intact with facial flap.
Modified Papilla Preservation Flap
Cortellini et al 20 described this technique, where papilla is elevated toward palatal aspect, and GTR membrane was used. This technique helps in the primary closure of flap in interdental spaces over the membrane.
Simplified Papilla Preservation Flap 21
Where the interdental space is narrow (<2 mm), an oblique incision is made across the associated papilla starting from buccal line angle of involved tooth to reach the mid interproximal position of papilla under the contact point of adjacent tooth. Then intrasulcular incisions are given along the defect and tiny buccal and lingual flaps are reflected allowing the buccal flap elevation with 2mm to 3mm of exposure of alveolar bone.
Microsurgical Approach
Cortellini et al further improved the result by using microsurgical instruments with microscopic magnification up to 4 to 16 times that improved illumination, access, and magnification of surgical field.
Conclusion
Rebuilding the pink esthetic is important. Management of interdental papilla is one of the most important factors that a clinician should pay attention to. Periodontal plastic procedures, a multidisciplinary approach involving orthodontic, restorative, prosthetic specialties, must be considered for a successful outcome.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.