
Abstract
Aim:
The aim of the study is to evaluate the efficacy in treatment outcome while using freshly prepared human amniotic membrane against freeze dried human amniotic membrane in intraoral soft tissue defects.
Method:
This prospective study included 20 patients having postsurgical soft tissue defect requiring primary wound coverage with human amniotic membrane. Patients were divided randomly into 2 groups. In group A, freshly prepared human amniotic membrane was placed, while in group B, freeze-dried human amniotic membrane was placed. Patients were evaluated on the basis of following parameters: postoperative pain, swelling, rate of epithelialization, and interincisal distance over a period of 6 months.
Result:
The results showed no significant difference in the mean of the pain between both the groups except on the first postoperative day. No significant difference in terms of reduction in swelling and increase in interincisal distance postoperatively was found at any point while using either fresh or freeze-dried human amniotic membrane.
Significant difference was found in the mean rate of epithelialization between the groups on the 7th and the 21st postoperative days.
Conclusion:
Thus, we conclude that freshly prepared human amniotic membrane in comparison to the freeze-dried human amniotic membrane accelerates epithelialization and healing when used in the repair of postsurgical oral mucosal defects.
Introduction
Surgical wounds if left uncovered are prone not only to infections but also to contraction by scarring and other clinical complications. 1 Because the lost material must be replaced with its equivalent according to the surgical principles, open wound surfaces often require a proper dressing material to prevent such complications. 2 Over the ages, a variety of dressing materials, from the use of fresh meat, honey, and antibiotic films to the use of lyophilized porcine skin, fibrin and chitin membranes, synthetic plastic, xenografts, and artificial skin have been evaluated and studied in an attempt to develop an ideal wound cover. 3
The human amniotic membrane (HAM) has been used as a biomaterial for surgical reconstruction for nearly 100 years. It is a graft with biological relationship to the wound surface. It is bacteriostatic in nature, inhibits fibrosis, promotes epithelialization, provides pain relief, lacks immunogenicity, has high tensile strength, and is a rich source of stem cells. Its unique properties along with its easy availability and comparatively low costs for preparation, storage, and use makes it an ideal alternative for soft tissue reconstruction in maxillofacial region. 4 The present study aims to compare the clinical outcomes of freshly prepared versus freeze-dried human amniotic membrane when used to reconstruct intraoral soft tissue defects.
Materials and Method
Materials
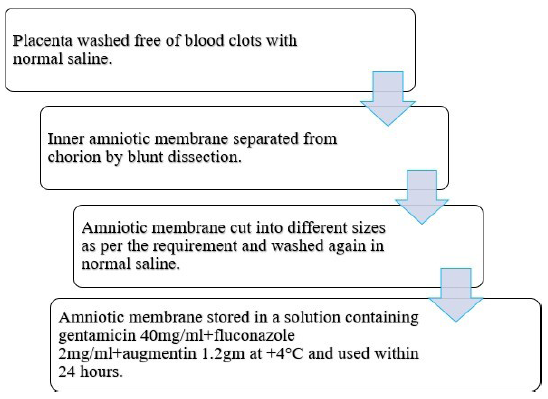
Amniotic membrane was prepared from the placenta of healthy pregnant women undergoing elective caesarean section. Eligible mothers were screened based on medical history, physical examination, and laboratory examination for viral markers and blood-borne infections to decrease the risk of disease transmission.
The placenta for procuring the freshly prepared HAM was obtained from Saraswati Hospital, Ajanta Hospital, Hind Hospital, and Fatima Hospital Lucknow (Figures 1 and 2).

Freeze-dried amnion is prepared by freeze drying the membrane at –60°C under vacuum for 48 h and then irradiating with 25,000 Gray. Thereafter it is stored in sterile sealed packs at room temperature and can be used until 2 years (Figure 3).
For our study, freeze-dried amniotic membrane was obtained from Tissue Bank, Tata Memorial Hospital, Mumbai.

Method
In this study, 20 patients were included of the age group between 20 and 60 years irrespective of their nationality, religion, gender, caste, creed, race, and socioeconomic status having intraoral soft tissue defects.
Patients were randomly divided into 2 groups.
The study was conducted after taking approval from the “Institutional Human Ethical Committee” and the “Institutional Research Development Committee.”
All selected cases were evaluated based on detailed history. Thorough clinical examination, hematological and radiological investigation, and RT-PCR for COVID-19 was done prior to treatment planning.
Surgical planning was done for each patient on an individual basis. The proposed treatment was then conveyed to the patient and an informed, written consent was obtained.
Patients who were immunocompromized, allergic to any drugs involved in the study, pregnant or lactating mothers, or having infection in the area of the graft were excluded from the study.
All patients underwent soft tissue reconstruction at various maxillofacial sites using either the freshly prepared or the freeze-dried HAM.
Evaluation of Clinical Parameters
The clinical parameters evaluated were divided into 2 groups: subjective (pain) and objective (swelling, epithelialization, and interincisal distance).
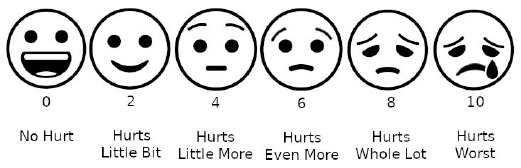
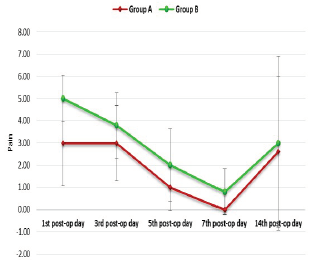
Pain was evaluated using the “Wong Baker Faces Pain Rating Scale” on the 1st, 3rd, 5th, 7th, and 14th postoperative days (Figure 4).
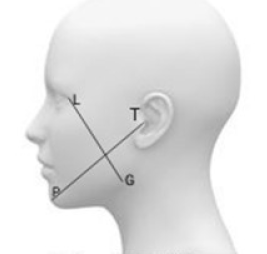
Swelling in oral submucous fibrosis (OSMF) cases was recorded as devised by Souza and Consone 5 using the craniometrical points in soft tissues pre-operatively and on the 1st, 3rd, and 5th postoperative days (Figure 5).
The landmarks taken were as follows:
Lateral canthus of the eye to the soft tissue gonion Tragus to the soft tissue pogonion.
Facial swelling recorded is equal to the sum of the two measurements divided by 2.
In cases of “premalignant lesions,” swelling was recorded on the 1st, 3rd and 5th postoperative days using the following scoring criteria of Siddique et al. 6
None- 0
Mild (just visible and palpable)-1
Moderate (obvious)-2
Severe-3
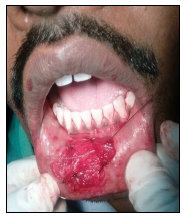
Epithelialization was assessed on 7th, 14th, and 21st postoperative day using the Grid System and scored according to the following criteria of Nouri et al. 7 (Figure 6).
Poor (inadequate<30%)-1
Fair(nearly the entire wound 30-70%)-2
Good(70-90%)-3
Excellent(entire wound >90%)-4
Epithelialization was observed from periphery to center.
According to the “grid system” the operated site was divided into multiple grids of 2 × 2 mm and the epithelialization was assessed by counting the number of grids.
The color of each grid is judged by comparing it to the normal adjacent mucosa. It signifies epithelialization at different stages.
Red = Complete epithelialization
White = No epithelialization
Mixed = Incomplete epithelialization
In case of boxes having mixed color, only those boxes were counted to be epithelized in which the red color was present in more than 50% of the total area of the box.
The rate of epithelialization = area of the epithelialized tissues/total area of the defect × 100
The assessment of interincisal distance in oral submucous fibrosis cases was done preoperatively, intraoperatively, and at the 1st week, 1st month, 3rd month, and 6th month postoperatively using the following scoring criteria by Kar et al. 8
Poor (decreased)-1
Fair (same or slightly increased <5 mm)-2
Good (increased >5mm)-3
Maximum mouth opening (unassisted) was measured using automatic vernier caliper or metallic scale with the patient’s head placed in upright position.
Patients were asked to open their mouth as wide as possible, and the maximum distance from the incisal edge of the maxillary central incisor to incisal edge of mandibular central incisor at the midline was measured.
In cases where central incisors were missing, lateral incisors were used for recording the maximum mouth opening.
Cases Operated
Case 1
Fair (same or slightly increased <5 mm), 2; Good (increased >5 mm), 3. Maximum mouth opening (unassisted) was measured using automatic vernier caliper or metallic scale with the patient’s head placed in upright position. Patients were asked to open their mouth as wide as possible, and the maximum distance from the incisal edge of the maxillary central incisor to incisal edge of mandibular central incisor at the midline was measured.
In cases where central incisors were missing, lateral incisors were used for recording the maximum mouth opening.
Case 2













Statistical Analysis
The results were analyzed using descriptive statistics and comparisons were made among various groups. Categorical data were summarized in proportions and percentages (%) and quantitative (discrete) data were summarized as mean ± SD. The following statistics were calculated in the present analysis: the arithmetic mean, the standard deviation, unpaired t-test, and repeated measures analysis of variance test.
Results
20 patients were included in this study: 16 were males and 4 were females. Their mean age was found to be 34.50 ± 10.30 years. Patients having oral submucous fibrosis, precancerous lesions, or other soft tissue lesions requiring reconstruction after excision were included.
The maximum mean of pain in group A was found to be 3.00 ± 1.94 on the first postoperative day which after fluctuations reached a minimum value of 0.00 ± 0.00 on the seventh postoperative day. In group B the maximum mean of pain was found to be 5.00 ± 1.05 on the first postoperative day which reached to a minimum mean value of 0.80 ± 1.03 on the seventh postoperative day. In both the groups, pain was found to be increased after the seventh postoperative day in OSMF cases because the patients were started on the mouth opening exercises. No significant difference was found in the mean of the pain between both the groups except on the first postoperative day (P > .05) (Graph 1).
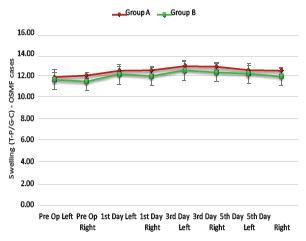
The maximum mean value of “swelling in OSMF patients” of group A was found to be 12.84 ± 0.46 cm on the third day postoperatively, while in group B the maximum mean value of swelling was found to be 12.45 ± 0.94 cm on the third postoperative day. No significant difference was found at any point (P > .05) (Graph 2).
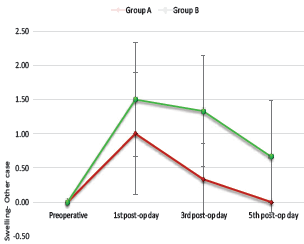
The maximum mean of “swelling in non-OSMF patients” of group A was found to be 1.00 ± 0.89 cm on the first postoperative day, which further reached to a minimum mean value of 0.00 ± 0.00 cm on the fifth postoperative day. In group B the maximum mean of swelling was found to be 1.50 ± 0.84 cm on the first postoperative day which reached to a minimum mean of 0.67 ± 0.82 cm on the fifth postoperative day. No significant difference was found at any point (P > 0) (Graph 3).
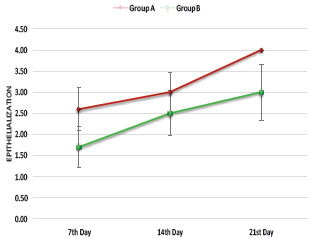
The study revealed that the mean value of the “rate of epithelialization” of group A on the seventh postoperative day was found to be 2.60 ± 0.52 which increased and reached a maximum mean value of 4.00 ± 0.00 on the 21st postoperative day. In group B, the mean value of the rate of epithelization was found to be 1.70 ± 0.48 on the seventh day postoperative day, which was comparatively less than group A, and it reached to a maximum mean value of 3.00 ± 0.67 on the 21st postoperative day. Significant difference was found in the mean rate of epithelialization between the groups on the seventh and the 21st postoperative day (P > .05) (Graph 4).
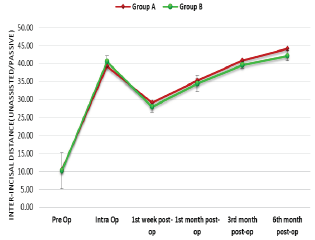
The mean “interincisal distance in the OSMF cases” of group A was found to be 10.40 ± 3.93 mm preoperatively which increased to 39.25 ± 2.50 mm intraoperatively and reached to a maximum mean value of 44.15 ± 1.31 mm by the sixth postoperative month. In group B, the mean value of interincisal distance was found to be 10.13 ± 5.02 mm preoperatively which increased to 40.55 ± 1.72 mm intraoperatively and reached to a maximum mean value of 42.18 ± 1.42 mm by the sixth postoperative month. No significant difference was found at any point (P > .05) (Graph 5) between the 2 groups.
Conclusion
HAM is a potential grafting material for oral cavity reconstruction with useful inherent properties and promising results in the repair of postsurgical oral mucosal defects. In 1999, the first attempt to heal nonhealing ulcers, wounds, and osteoarthritis by freshly collected amniotic membrane and amniotic fluid was started successfully. 9 The whole idea behind the application of freshly collected and fully screened amniotic membrane and fluid was that because of the presence of potent progenitor cells, stem cells combined with growth factors and cytokines unlike other methods for application of amniotic membrane. These factors help regeneration, repair, and healing to occur effectively.
At the end of our study, we conclude that there exists no statistical difference in terms of clinical outcome while comparing freshly prepared HAM with the freeze-dried HAM except in terms of rate of epithelialization which is seen to be increased in the case of freshly prepared HAM. Also, freshly prepared HAM ensures adequate coverage of the defect and early return to function postoperatively. Clinical acceptability, applicability, availability, and affordability of freshly prepared HAM makes it a reliable option for surgeons as well as patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.