
Abstract
Abstract
Presence of head injury in patients with maxillofacial trauma is a potentially life threatening condition. Frontal bone injuries are uncommon but significant and may appear with facial deformation and impaired aesthetics. Bicoronal approach provides excellent surgical access for frontal bone reconstruction with a very low rate of morbidity. This paper present two cases of posttraumatic frontal bone deformity treated with bicoronal approach.
Introduction
The bicoronal approach is regarded as a popular and versatile approach to surgically expose the skull, and the upper and middle third of the face with minimum morbidity. Its popularity is accounted because of the excellent exposure and aesthetic scar provided by this approach.1-3
Hartley and Kenyon first described this approach in 1907, and Sachs advocated bilateral frontal lobe exposure two decades later. In the late 1970s, Tessier and later Henderson and Jackson modified this approach for Le Fort II and III osteotomies, following which it gained widespread acceptance.4, 5
Selection of a surgical approach must be given the utmost importance while deciding a treatment plan for complex craniofacial surgeries. The surgical access to this region depends on various factors, including the extent of exposure to critical facial structures, aesthetics, and potential morbidity. The ideal surgical approach should provide adequate exposure, reduce the risk of injury to important structures, and enable acceptable aesthetic outcomes.
This article presents two cases of frontal bone fracture managed successfully using bicoronal approach with excellent uneventful and aesthetic outcomes.
Case Report
Patient was planned for frontal bone reconstruction via bicoronal incision under general anesthesia. Incision was made involving skin, subcutaneous tissue, and galea aponeurotica extending from one superior temporal line to the other, revealing the subgaleal plane of loose areolar connective tissue. Below the superior temporal line, incision was made to a depth of the glistening superficial layer of temporalis fascia. Following this, preauricular extension of the incision was made up to the level of the ear lobule. Dissection was continued anteriorly in the subgaleal plane to a point 3 to 4 cm superior to the supraorbital rims. Superior temporal lines were palpated and incision was made through the pericranium. A subperiosteal dissection was then done to expose the supraorbital rims. Once the lateral portion of the flap was elevated to within 3 to 4 cm of the body of the zygoma and zygomatic arch, the superficial layer of temporalis fascia was incised at the root of zygomatic arch, and continued anteriorly and superiorly at a 45° angle joining the cross-forehead incision made previously. Blunt dissection was done in this plane, preserving the temporal branch of facial nerve, to reach the superior surface of body of zygoma and zygomatic arch. An incision was made through the periosteum over the upper border of zygomatic arch and body of zygoma extending over the posterior surface of body of zygoma to the lateral orbital rim. Subperiosteal flap was then raised which allowed the flap to fold anteriorly, thus exposing the deformity entirely.
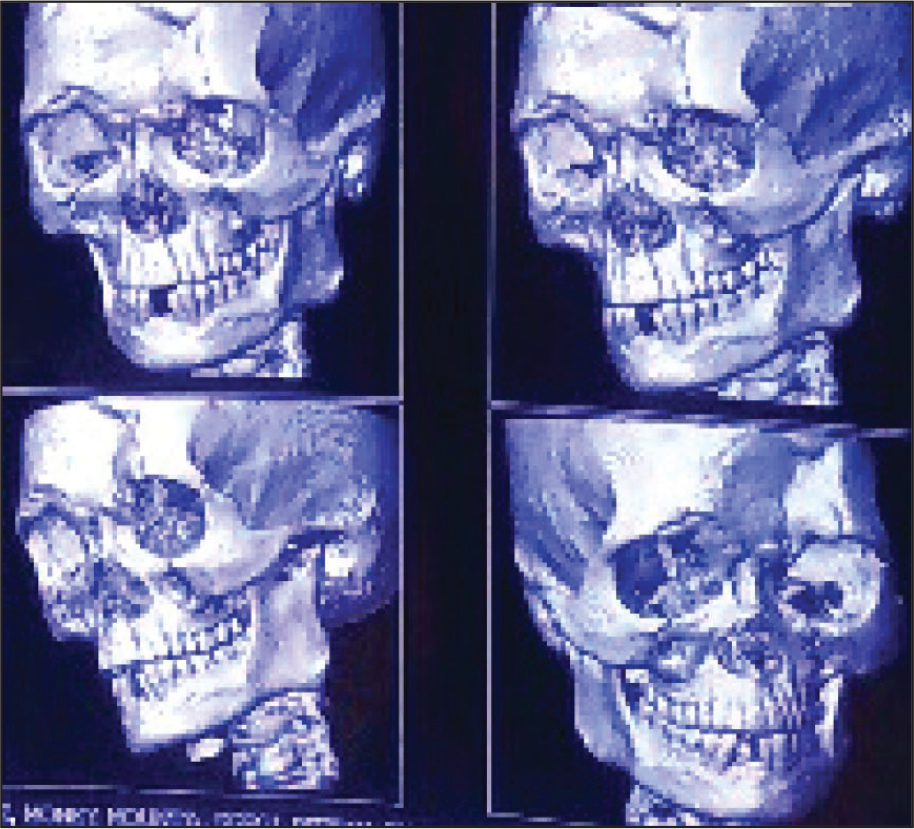
Deformity of the Frontal Bone

Deformity of the Frontal Bone: 3D CT Scan
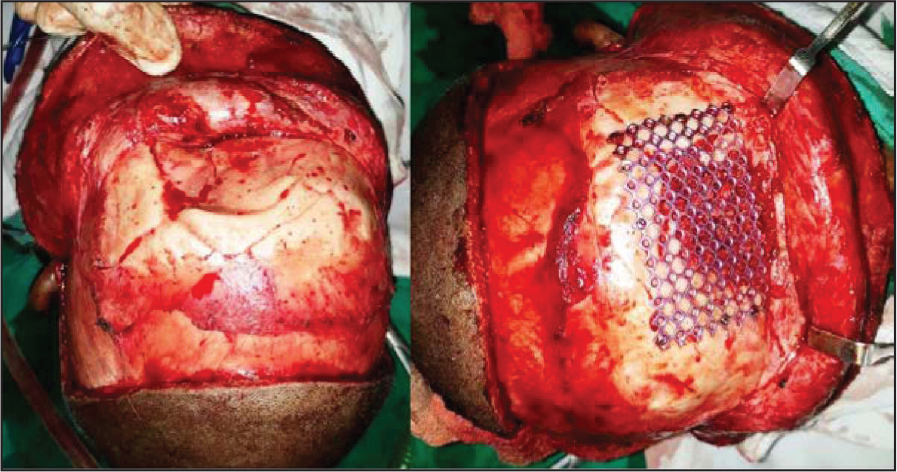
Once the defect was exposed, a 1.5 mm Ti mesh was properly contoured to cover the defect and was secured with 4 mm screws. The gap between the defect and Ti mesh was reconstructed with corticocancellous graft harvested from the ipsilateral iliac crest (Figure 3). Layerwise closure was done with 4 to 0 vicryl and 3 to 0 mer silk for deep and superficial layers, respectively, and a compressive dressing was given (Figure 4).
Bicoronal Approach to the Deformity. Also Visible Are A Titanium Mesh and Ileac Crest Graft.
Bicoronal Flap Sutured in Place

Fourth Year Follow-Up

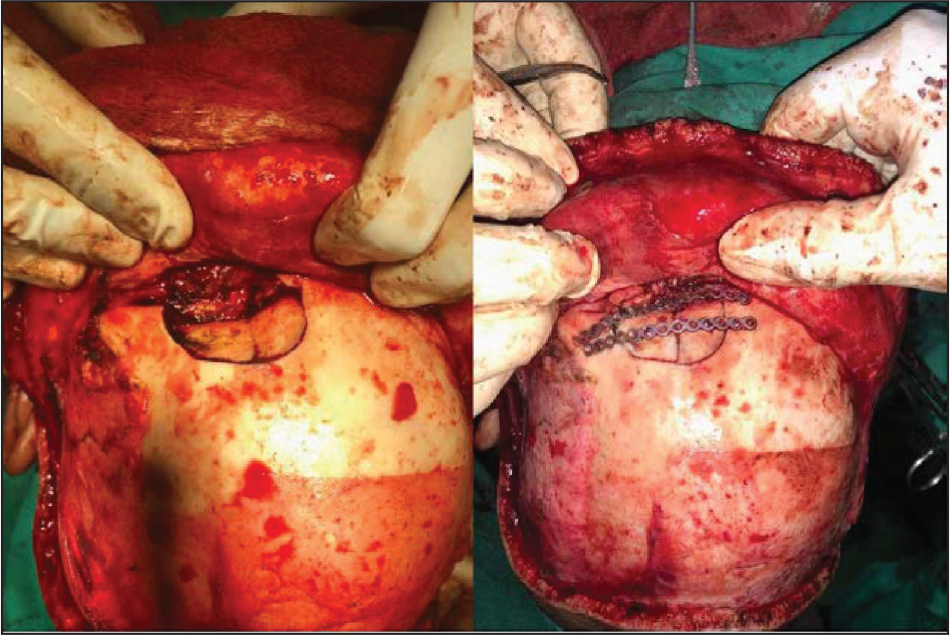
Frontal Bone Defect (Case 2) Visible Through Bicoronal Approach. Also Visible Are the Miniplates.
The dressing was removed on the third postoperative day and skin sutures were removed on the 10th postoperative day. The operated site healed uneventfully and results obtained were aesthetically acceptable and stable after a follow-up period of 4 years (Figure 5).
Discussion
Selection of an appropriate surgical approach is one of the most important determinants as it can potentially influence the anatomic reduction and fixation of the fractured maxillofacial skeleton, the duration of surgery, and patient’s overall hospital stay. Direct exposure of all the fractured sites appears to be prudent as this allows for direct access to the fracture site without much dissection, good assessment of the type of fractures, and the degree of displacement that helps to accomplish acceptable anatomic reduction and fixation of the fractures. However, despite having aforementioned advantages, direct exposure by multiple incisions for complex craniofacial reconstruction is avoided as it may leave unacceptable scars on face and many times it fails to provide wide exposure to the region that is probably the first and foremost requisites when selecting an appropriate approach for such complex reconstructions. On the other hand, the hemicoronal/bicoronal approach provides maximum exposure of the operated site, allows for calvarial bone graft harvest through the same approach when immediate bony augmentation is required, and allows for the scar to be hidden in the hairline. Whether single or multiple incisions are used to expose the fractured segments, these incisions should provide adequate exposure with aesthetically acceptable minimal scar, and should reduce the risk of damage to the regional vital structures and facial nerve branches as well.
Indications for the hemicoronal/bicoronal approach in craniomaxillofacial surgery include: (a) severe craniofacial dysjunction, including Le Fort type III, frontal sinus, and nasoethmoidal fractures, (b) severe comminuted zygomatic arch and zygomaticomaxillary complex fractures, (c) simultaneous craniotomy procedure for treatment of intracranial injury and maxillofacial fractures, and (d) osteotomy for reduction of old malunited fractures.5-8
Complications of the bicoronal approach include supraorbital and preauricular sensory disturbances resulting in forehead and temporal paresthesia/anesthesia, motor weakness of zygomatic and temporal branches of facial nerve, and seroma or hematoma beneath the flap. Trismus, ptosis, and epiphora are most likely to be related to the area of impact of the initial injury rather than the approach itself. 9
The conventional coronal incision begins at the base of helix and is transported superiorly across the scalp over skull and then to the helical root of the other side. The incision may be extended to the point of the tragus or beyond for further exposure inferiorly as a preauricular extension. Depending on the exposure required, the incision can be curved anteriorly since this maneuver adequately relaxes the tense flap that helps in convenient retraction of the flap.
The straight line incision scar becomes more apparent with wet hair as a consequence of this approach, especially when the hair is parted sideways. As a result of this unaesthetic scar, Munro and Fearon modified the existing conventional bicoronal incision that is known as stealth incision. The stealth incision is a zigzag incision line that camouflages the coronal scar. A disadvantage associated with this modification is that it is more time consuming as compared to a linear incision to both produce and close. The longer incision may result in more blood loss as well (that may not be significant as it heavily depends on the expertise of surgeon). In addition, the design of the incision is more technically sensitive, requires more expertise, and is not readily and symmetrically reproducible.10, 11
The exposure obtained in both of our cases was excellent and this approach met the aesthetic expectations of patient and surgeon in terms of the postoperative results. The postoperative period in both the patients was uneventful and results have been stable after a follow-up of more than four years. The bicoronal approach provides wide surgical exposure to the upper and upper middle third of the face with reduced incidence of significant and long-term complications, with good aesthetic results.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.