
Abstract
Abstract
Orbital reconstruction is very challenging due to complex anatomy of the orbit and desirable functional and aesthetic results. Timing of intervention, indications for open reduction, choice of implant material, and placement play a very crucial role in the treatment protocol. Correction of posttraumatic enophthalmos and residual diplopia remain difficult to achieve and even sometimes need secondary revision. In the present case, we have discussed about the correction of posttraumatic enophthalmos and the challenges faced during and postsurgery and review about the management protocol for orbital reconstruction.
Introduction
Enophthalmos refers to recession of eyeball into the orbit. It occurs in case of isolated orbital blow out fractures or associated zygomatic complex fractures or nasoorbito-ethmoid fractures. The most common etiology is increase in the orbital volume due to displaced zygomatico-maxillary complex (ZMC) fractures or naso-orbito-ethmoid complex fractures. Periorbital fat atrophy, fibrosis of retrobulbar tissues and loss of suspensory ligament can also lead to enophthalmos.1, 2
The main concern in managing such conditions is restoring the facial symmetry along with vision of the involved eye, enophthalmos, restricted ocular motility and esthetics. In this case report we are presenting the results after reconstruction the orbit and difficulties faced during the surgery.
Case Report
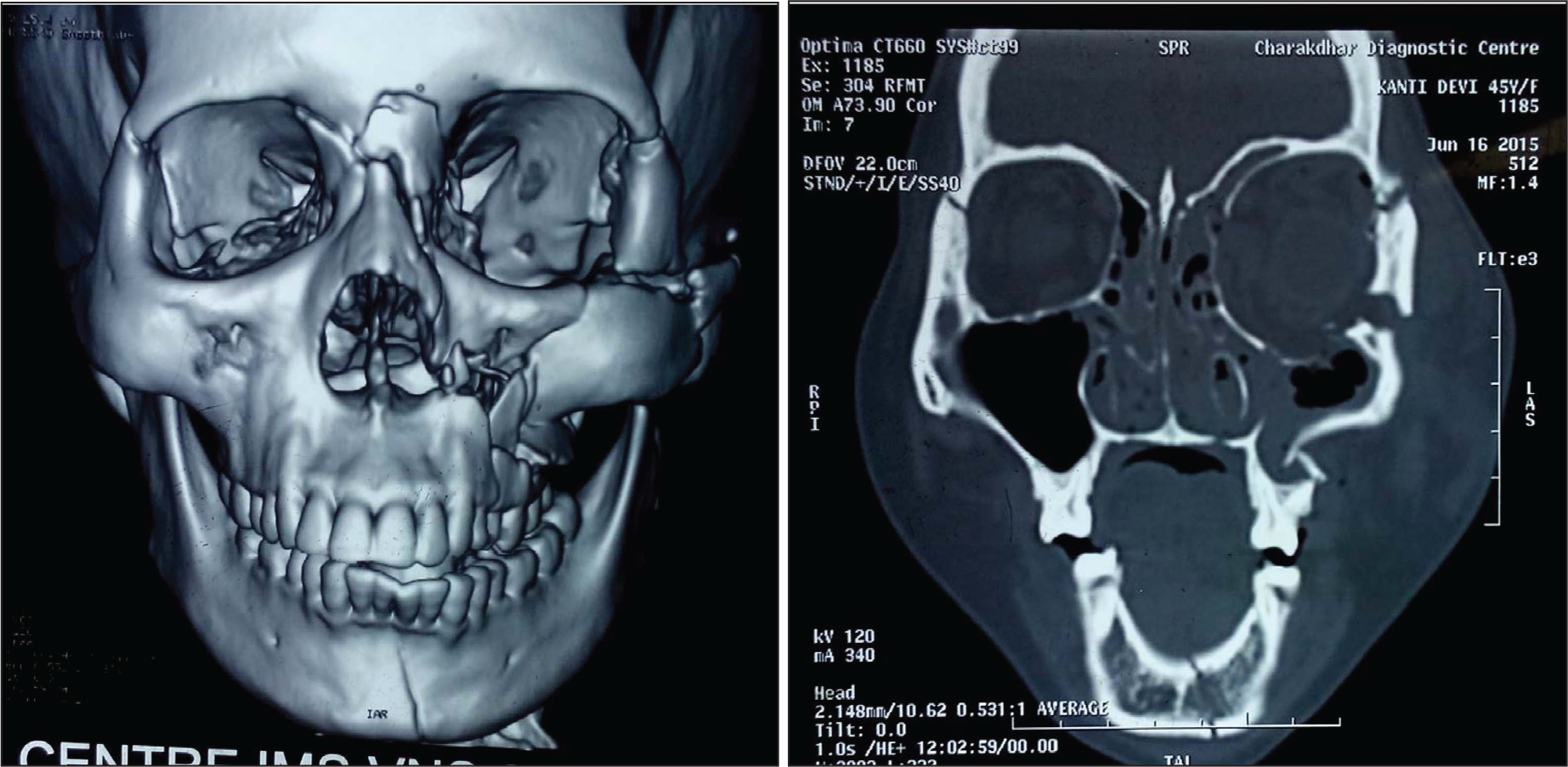
45-year-old female patient, presented to the trauma center sustaining multiple injuries due to road traffic accident. She was drowsy, irritable with Glasgow Coma Score of E3V4M5 (12/15). History of loss of consciousness for one hour, bleeding per nose and oral cavity was reported. Vitals were recorded as heart rate—110/min, blood pressure—94/46 mm of Hg, respiratory rate—18/min, and afebrile. On clinical examination a lacerated wound over the left side of forehead and malar region of the left side face along with circumorbital ecchymosis, edema and subconjuctival hemorrhage of the left eye was found. On palpation tenderness over left side of mid face and lower face suggestive of bony injury. Tenderness was also reported over the left-side hypochondrium region and left clavicle region. On computed tomographic examination of face, comminuted fracture of left ZMC with inferolateral displacement and orbital blow out along with dropping of periorbital fat into the antrum, naso-orbito-ethmoid complex fracture and left side parasymphysis and ascending ramus of mandible was reported (Figure 3a-3b). Computed tomography (CT) of the abdomen was suggestive of hemoperitoneum due to splenic laceration, which was alarming and also led to anemia (Hb 6.2 g%) and hypotension. PA of chest revealed fracture of left clavicle bone. Initially, the patient was admitted in trauma surgery department for the management of splenic injury. Emergency splenectomy was done and adequate blood transfusion was performed to maintain the hemodynamic stability. After 3 weeks, the patient was referred to our side for further management of the facial injury. She had the chief complaints of sunken left eyeball with double vision in left eye. On detailed examination, we found severe enophthalmos of left eye along with hypoglobus, ptosis and diplopia in the upper gaze (Figure 1). She had dilated pupil of left eye with no light reflex. Forced duction test was suggestive of restriction in inferior rectus and inferior oblique muscle movement. Hess charting revealed diplopia in the upper gaze.
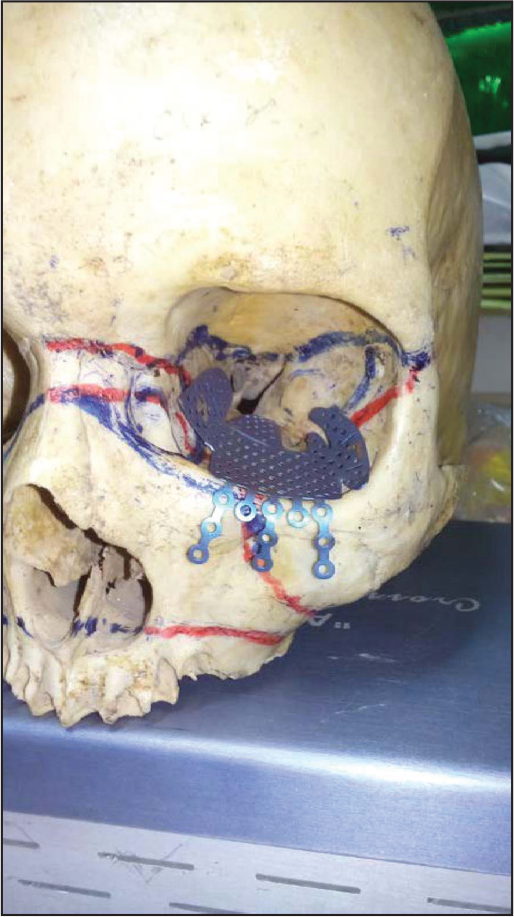
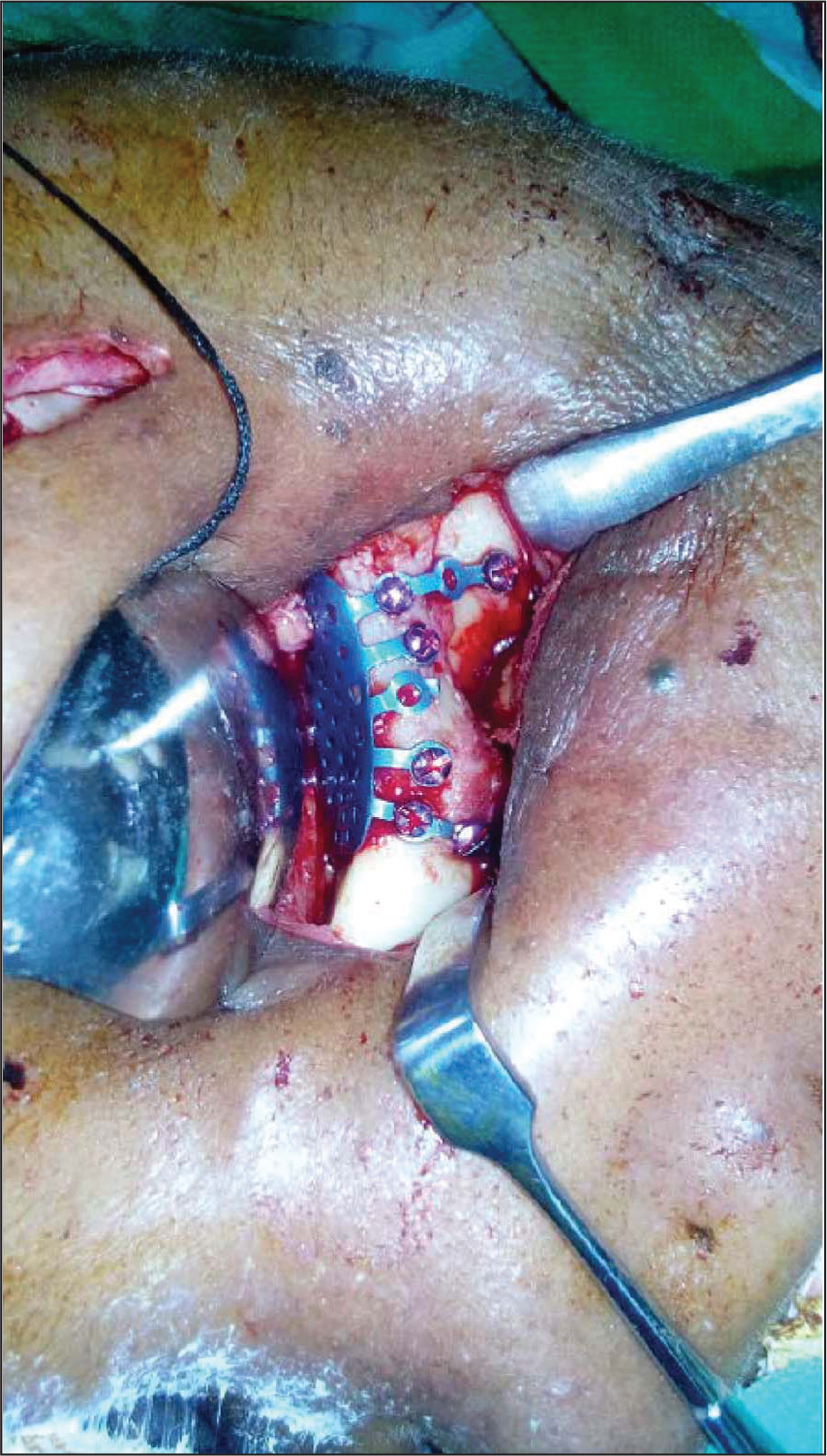
She was planned for the titanium mesh reconstruction of the orbital floor and fixation of zygomatic complex fracture with miniplates. The orbital mesh was precontoured over the dried skull of similar age group (Figure 2). The surgical procedure was carried out under general anesthesia, and the lateral brow approach was used to fix at fronto-zygomatic suture and zygomatic body fractures. The modified subciliary approach was used for the exposure, and titanium mesh was fixed to the inferior orbital rim (Figure 4). Intra-orally vestibular incision was given to fix the zygomatico-maxillary buttress region. After internal fixation, closure was done in layers with 4-0 vicryl suture and 4-0 prolene suture. After 1 week, mild periorbital edema was present. There was slight elevation in supratarsal fold with reduction in ptosis. Improvement in enophthalmos and diplopia was found. The pupil was still dilated as seen in preoperative period. After a month of follow-up, residual enophthalmos and slight hypoglobus were found. Improvement in dilated pupil and diplopia was reported (Figure 5a-5b).
Discussion
Orbital blow out fracture is one of the most challenging traumas of the maxillofacial region; the orbit being the most prominent and esthetic facial bone, minor asymmetry is also appreciated and needs to be corrected as early as possible. 3
The most common etiology is by assault or road traffic accidents. Orbital fractures constitute less than 20% of all maxillofacial fractures. If other fractures such as nasoethmoid and ZMC are involved, it becomes approximately 50% of all facial fractures. 4 Diplopia and enophthalmos are most commonly associated with orbital trauma and rarely blindness may occur. Diplopia can be monocular or binocular, monocular being more alarming should be attended as soon as possible. Reconstruction needs thorough knowledge of the surgical anatomy, form, and function of orbital and periorbital tissues, and the variable material options. 5
Surgical Anatomy
Orbit is confluence of 7 bones: maxilla, zygomatic, frontal, ethmoid, lacrimal, palatine, and sphenoid. The average volume of an adult orbit is 30 mL, out of which the globe constitutes approximately 7 mL. Orbit growth continues till puberty. The orbital walls thickness varies considerably. The orbital floor and medial wall are most commonly fractured owing to their least thickness. The orbital roof underlies frontal sinus and anterior cranial fossa. In old age, there can be resorption of the orbital roof in few locations, leading to the direct connection of dura with periorbita.
The orbital floor is formed primarily by orbital plate of maxilla, orbital surface of zygomatic bone, and orbital plate of palatine bone. It is bordered laterally by inferior orbital fissure and medially by a maxilloethmoidal suture. Infraorbital foramen lies 4 mm below the inferior orbital margin, which transmits infraorbital nerve and vessels. Orbital blow-out fractures present commonly due to very thin orbital floor (0.5 mm), which is even more weakened by infraorbital groove and canal, and invariably involves infraorbital nerve and vessels leading to diplopia and enophthalmos.
The lateral orbital wall is formed by the greater wing of the sphenoid and the zygomatic bone. It is the thickest orbital wall which separates the orbit from the middle cranial fossa and the temporal fossa. The superior orbital fissure creates demarcation between the roof and the lateral wall.
The medial wall is the thinnest orbital wall formed anteroposteriorly by the frontal process of maxilla, lacrimal bone, orbital plate of ethmoid, and body of the sphenoid, which are almost parallel to each other. The anterior ethmoidal foramen lie 20 to 25 mm posterior from the anterior lacrimal crest, opens in the anterior cranial fossa at side of cribriform plate, and transmits anterior ethmoidal nerve and vessels. Posterior ethmoidal foramen is 32 to 35 mm posterior to the anterior lacrimal crest and 7 mm anterior to the anterior rim of the optic canal and transmits posterior ethmoidal nerve and vessels. The anterior and posterior ethmoidal foramen are present with in the frontoethmoidal suture line.
Deep dissection of the orbit carries high risk because of the presence of the optic nerve and contents of the superior orbital fissure. The infraorbital nerve, the inferior orbital fissure, the greater wing of the sphenoid, and the orbital plate of the palatine bone are the four surgical landmarks of the deep orbit present in almost every case of blunt orbital trauma.4, 6
Diagnosis, Indications and Timing of Surgery
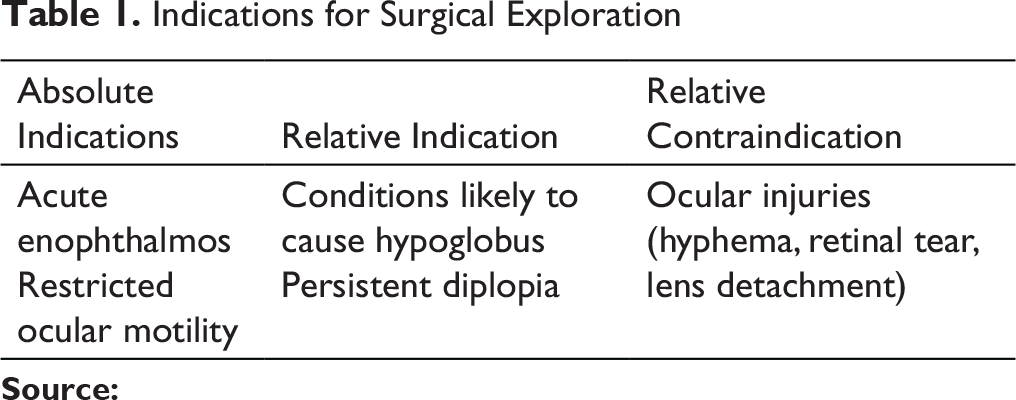
Indications for Surgical Exploration
The gold standard imaging for orbital trauma is to obtain sections in coronal planes without contrast. Magnetic resonance imaging has limited uses and is less sensitive than CT.6, 7
Indications
Lack of ocular motility, enophthalmos, and persistent diplopia require surgical exploration of the orbit. Muscle entrapment into a defect in the orbital floor is the most common etiology for restricted ocular motility. According to de Man and colleagues, severe restricted ocular movement, positive forced duction test, and CT evidence of muscle entrapment are indications for open reduction. For enophthalmos greater than 2.0 to 3.0 mm, surgical correction is required for the orbital floor reconstruction. There is 1 mm increase in enophthalmos for every 1 mL increase in volume. It can be clinically measured using CT scans or Hertel’s exophthalmometer (Table 1).
Persistent diplopia after 7 to 10 days (time required for reduction in muscle edema) postinjury needs surgical correction.5, 8–9
Correct timing of surgery plays a pivotal role in resolving the impairment because of increased fibrosis and adhesions with delayed surgery. It should be based upon clinical findings, age, type of fracture, and radiographs. The goal is to restore the orbital walls, and sometimes delay is beneficial which allows the swelling to resolve helping in making a more accurate diagnosis.
Burnstine (2002) recommended surgery within 2 weeks in cases with diplopia and cases with orbital tissue entrapment.
Study of 108 orbital fractures by Matteini et al suggests early intervention for fractures with diplopia. Functional impairment and muscular entrapment in children need early treatment as compared to adults. 10
Late reconstruction of the orbit is sometimes necessary in cases of residual defects after primary surgery, or for injuries that went undiagnosed, or where no adequate medical evaluation was done. It should be done at least 6 months postsurgery to allow adequate healing. 7
Properties of an ideal material for orbital reconstruction should be strength, cost-effectiveness, easy availability, easy application and fixation with screws, resorbable, low infection rate, less reactivity, and biointegration. Various materials have been described in the literature for the orbital reconstruction like, polydiaxone, nylon, porous polyethylene, titanium mesh, and autogenous bone grafts. The most commonly used grafts are calvarial bone of split thickness and iliac crest. But, in general, titanium mesh is commonly used due to its easy availability, cost-effectiveness, easy adaptability, and fixation and biocompatibility. Precontouring can also be done, which again saves a lot of time intraoperatively. But there are chances of postoperative scarring to the mesh, which can lead to restricted ocular motility so it is recommended to use calvarial graft as an onlay graft over it.11, 12
Preoperative Photograph Showing Enophthalmos

Precontouring of the Titanium Mesh Over a Dried Skull
Coronal and 3D View of CT Scan Showing Orbital Blow Out Fracture
Intraoperative Photographs Showing Adaptation of the Mesh
Postoperative Photograph Showing 1 Month Follow-Up

Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.