
Abstract
Background
Type 2 Diabetes (T2D) is associated with a higher magnitude of static postural sway. This investigation compared three statistical methods to explore the role of sensory modalities contributions to posture in T2D.
Research design and methods
Two groups were evaluated in this study (n = 20); T2D group - 10 participants with T2D (age 54.6 ± 11.09 years), comparison group - 10 age/sex matched healthy participants (age 53.18 ± 9.89 years). Postural sway data was collected using the modified Clinical Test of Sensory Integration in Balance (mCTSIB), consisting of four 20-s trials on a balance plate with manipulations of vision and support surface to target the contributions of proprioceptive, visual, and vestibular senses. Scores were assessed by group wise analysis of path length, group wise analysis of percentile rank, and distribution of percentile rank.
Results
The two-way ANOVA used for the group wise analysis of path length and percentile rank showed significant differences between groups scores (p < .05), but no significant interactions between group and condition. The frequency distribution of percentile rank of the T2D group revealed unimodal distributions for all conditions except for vestibular, which was found to have the highest and lowest percentile ranks of any condition.
Conclusion
The results show that the individualized normative analysis revealed aspects of individual impairments that would have otherwise been missed using a group-wise method. Though limited, our findings also suggest that impairments to the vestibular system may be more pronounced but less frequent compared to proprioceptive and visual impairments.
Introduction
Postural control is a dynamic behavior that involves corrective adjustments of the body in order to maintain upright position. These adjustments are made in response to detecting body sway through inputs from visual, vestibular, and proprioceptive sensory systems.1,2 These movements often occur automatically, although conscious mechanisms have also been identified (e.g. attentional demands or balance confidence). 3 A disturbance in any one of the contributing sensory or cognitive systems can lead to postural instability and reduced mobility. 2
T2D is associated with a higher magnitude of postural sway.4,5 Diabetes is an impairment of control over the body’s blood glucose levels due to either a lack of insulin or reduction in response to insulin . 6 This can result in acute hypo or hyperglycemic states that cause symptoms that may affect a person’s balance such as trembling, weakness, blurry vision, nausea, and confusion. Long term complications of uncontrolled blood sugar include diabetic peripheral neuropathy (DPN), diabetic retinopathy (DR) and diabetic vestibulopathy (DV). All of which have been found to significantly impact balance and falls risk.7–9 Bonnet et al., (2009) 4 suggest that DPN is the primary factor of postural instability in persons with type 2 diabetes (T2D). However, there is little agreement on how the impairment of individual sensory systems contribute to the measured increase in postural sway.4,5
It is well established that in persons with T2D, DV has a high prevalence (50–84%)9–11 while DPN and DR are also quite common (prevalence between (26–34%).12–15 Though there is clearly a discrepancy in the prevalence of these sensory complications, their functional effects on postural sway has yet to be fully understood. It is unclear as to why there is a lack of agreement, but one reason may be due to the multiple forms and complexity of available testing methods . 16 Diagnostic testing for DV and DR are the most cumbersome, due to the additional specialist training, equipment, and cost associated.17,18 Due to the additional barriers associated with screening for these complications, many patients with diabetes do not receive proper screening and treatment. 19 Sensory complications of T2D are prevalent and may be irreversible if not detected and treated early. 20 Utilizing less costly and more accessible forms of screening may enhance early detection and feasibility for researching these complications concurrently. 21
Postural instability is assessed clinically through observation or, through medical devices known as force plates. Force plates are objective systems that can provide higher spatio-temporal resolution and a recording of the sway performance that can be later analyzed.22,23 Lopatin et al. (2022), was able to show that the use of portable force plates is a quick and easy way to assess many of the various sensory aspects of postural sway for patients with T2D during a visit with their primary care physician. Though this work has not been examined for the implications of sensory complications to postural sway, it does show the feasibility of using balance assessments to quantify sensory deficits in a clinical setting.
Thus, the current study aimed to provide an initial examination of sensorimotor aspects of postural sway of persons with T2D. Namely, by furthering the work of Lopatin et al. (2022), 24 three different methods for analyzing balance testing results for patients with T2D were examined and compared; (1) groupwise analysis of path length, (2) groupwise analysis of percentile rank, and (3) individual analysis of percentile rank. It is the goal of this work to further define the methods that should be followed to assess the sensory deficits using a portable force plate to provide effective patient-centered care.
Materials and methods
Participants
Patients were recruited from a general physician’s office during one of their appointments, qualifying if they had a T2D diagnosis, were between the ages of 18–64 years, and were able to walk and stand unassisted. Participants were excluded from the study if they could not walk or stand unassisted (used walker, cane, wheelchair), had any neurological disorders that could affect their balance, had a lower limb replacement, or had a lower limb injury in the past 6 months. Participation in this study was also limited to those with fasting blood glucose levels between 80–250 mg/dL, in order to avoid ketone body testing, which is recommended by the American Diabetes Association (ADA) exercise guidelines for when blood glucose is above 250 mg/dL. 25
Characteristics of participants with T2D.
A comparison group was sampled from normative data 26 which is composed of persons who self-identified as healthy with no known balance impairments. Comparison group participants (n = 10) were sampled from corresponding age and sex matched subsets of the normative data. Participants in the T2D group over the age of 59 years were matched with the oldest participants from the normative data set.
Testing procedures
All testing on participants with T2D was conducted at the general physician’s office during the participant’s scheduled appointment. Fasting blood glucose, height and weight were measured by physician’s office staff following standard clinical procedures and recorded. A 10g-monofilament test was conducted on all participants with T2D to screen for DPN. Participants performed the modified Clinical Test of Sensory Integration in Balance (mCTSIB) on a BTrackS Balance Plate (Balance Tracking Systems Inc., CA, USA) connected to a 10” Windows 10 tablet (Fusion5, FWIN232 Plus S1) running BTrackS Assess Balance Advanced Software (v5.5.6).
Modified Clinical Test of Sensory Integration in Balance (mCTSIB) testing evaluates the relative contributions of various sensory modalities on postural sway control. 26 This test has been shown to have high test-retest reliability. 27 Four trials were performed on the BTrackS balance plate, with each lasting 20 s while the participant stood as still as they could for each trial. The first trial (standard condition) had the person stand still with eyes open. In the second trial (proprioception condition), they stood still with eyes closed. For the third trial (vision condition), and fourth trial (vestibular condition) the participant stood on a foam pad on the plate with eyes open and closed, respectively. Scoring for each condition was based on the participants’ center of pressure (COP) during each of the 20 s conditions. Higher scores indicated more movement of the COP (path length) during the conditions, with lower scores indicating less postural sway and better balance. COP path lengths were calculated by the BTrackS Assess software.
From the path length results, percentile rankings were calculated for each condition of the mCTSIB for all participants. Rankings were calculated based on the sex (male or female) and age of the participant (30–60 years, subdivided by decade) using previously published normative data. 26 This normative dataset provides pathlength scores separated by age and sex (ex. 40–49 males, 50–59 males, 50–59 females, etc). Rankings were determined per participant using the percentile rank function in Excel. Participants over 59 years of age (n = 5, ranging from 60–64 years of age) were included in the 50–59 age bracket as norms for this age range were not available in the reference data set.
Statistical analysis
Separate 2-Way, mixed model ANOVAs (2 × 4) were conducted to look for differences between fixed groups (T2D and Comparison) and repeated mCTSIB conditions (Standard, Proprioception, Vision, Vestibular), for path length and percentile ranks. Follow-up, pairwise t-tests were used to evaluate differences between conditions. Alpha 0.05, with Bonferroni correction, was used to determine significance. Frequency plots were generated to display the distribution of occurrence of percentile ranks of the T2D group for the four mCTSIB conditions into four bins (0–25%, 26–50%, 51–75%, 76–100%) representing very poor, poor, good, and very good performance. All analysis were performed in Microsoft Excel (v16.76) using the Analysis ToolPak.
Results
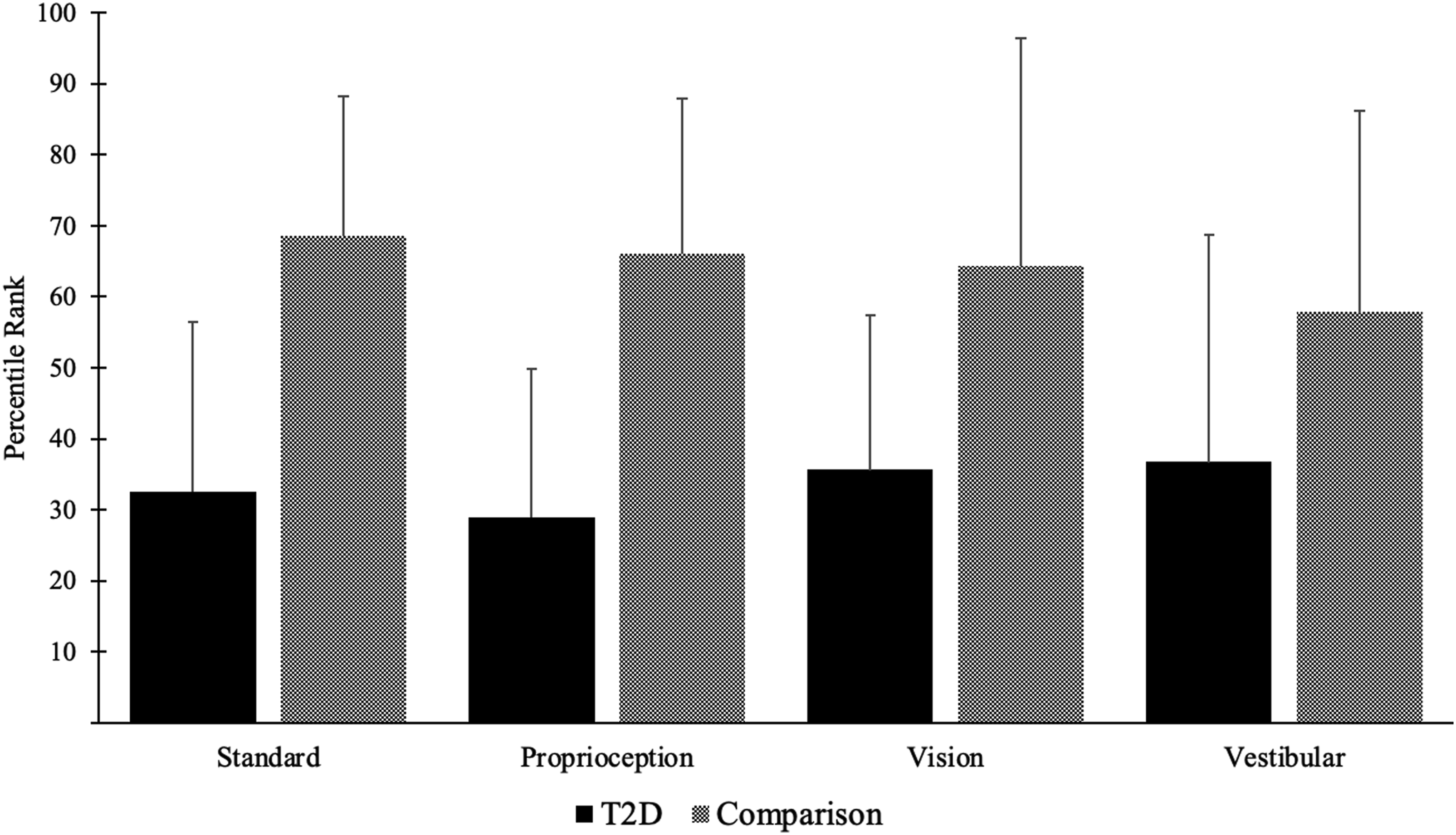
A significant main effect (p < .05) was found between groups for both path length (Figure 1) and percentile rank (Figure 2), with the T2D group having significantly higher path lengths and lower percentile ranks. A significant main effect (p < .001) between conditions was found for path length, but not for percentile ranks. Bonferroni corrected pair wise tests reveal increased path length between standard and proprioception (p < .001), no significant difference between proprioception and vision (p = .037), and a significant increase between vision and vestibular (p < .001). No specific interactions between groups and conditions for either path length or percentile rank was found (p > .05). Mean path lengths (cms) of the T2D and control group for the four mCTSIB conditions. Error bars represent standard deviation. Significant (p < .05) main effects of group and condition were found using 2-Way mixed model ANOVA. * Indicates significance. Mean Percentile ranks for the T2D and comparison group for the four mCTSIB conditions. Error bars represent standard deviation. A significant (p < .05) group main effect was found using a 2-Way mixed model ANOVA.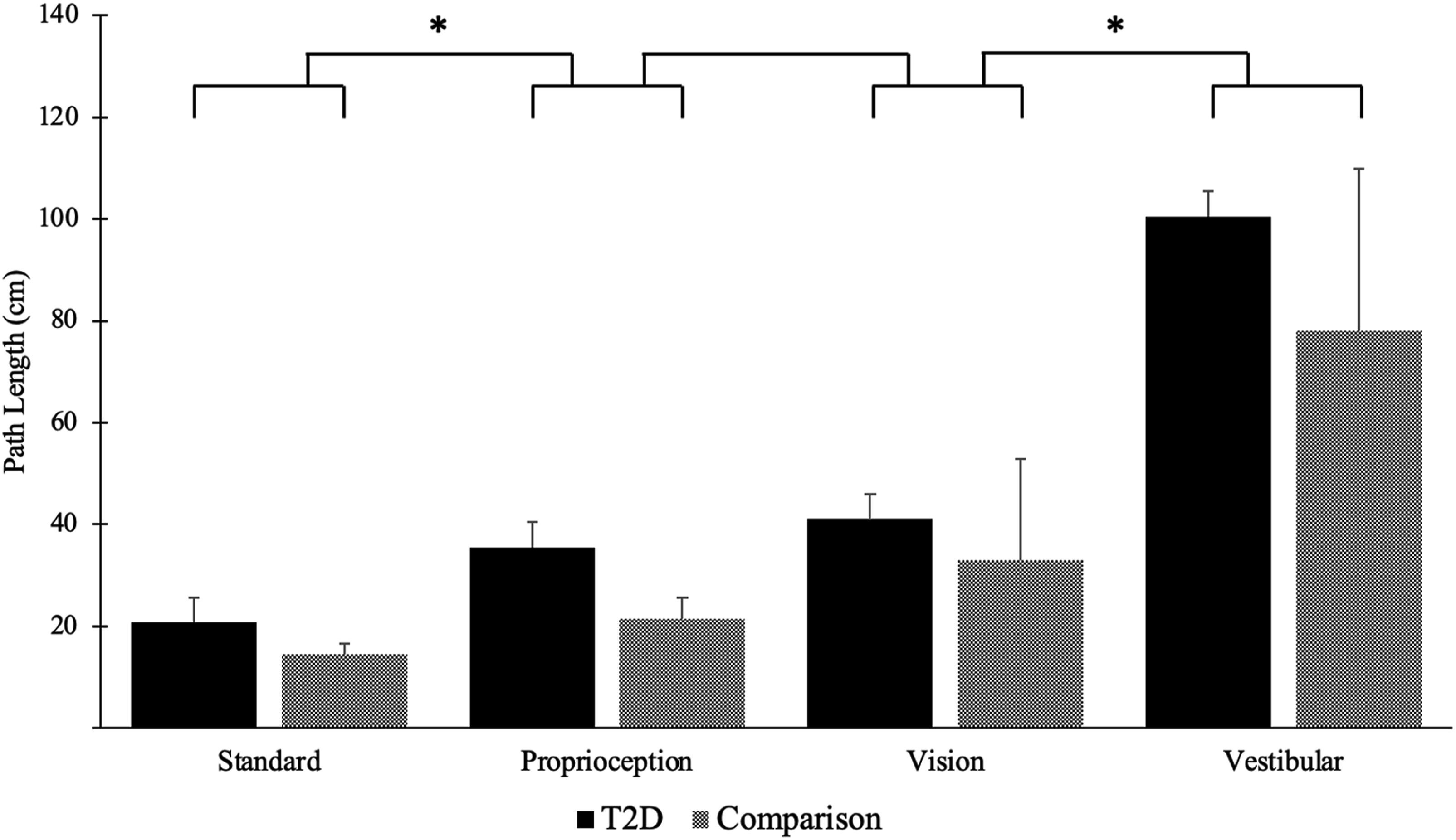
Frequency plot distributions revealed that a majority of the T2D group ranked below the 50th percentile in all conditions. The vestibular condition had the largest number of participants scoring in the 0-25th percentile category (n = 6), with the standard and proprioception having the second most (n = 4). The vestibular condition was the only condition to have no participants score in the 26–50th category and one participant in the 76–100th category.
Discussion
This study sought to evaluate several methods for analyzing the sensory contributions to postural sway control of persons with T2D. Three forms of analysis were carried out: (1) group-wise analysis of path length between the T2D and healthy comparison group, (2) group-wise analysis of percentile ranks between the T2D and healthy comparison group, and (3) individual case analysis of percentile ranks of the T2D group. This work will help establish the groundwork for further investigations into the implications of sensory impairments of T2D on postural sway control.
Group-wise analysis
Group-wise case control testing is commonly used in the field of postural sway,28,29 most often by comparing raw scores such as path length or scores normalized to anthropologic measurements such as leg length or height30,31 between a clinical group and a comparison group. Group-wise analysis of path length and a more novel percentile rank approach to normalization 26 were conducted. Neither fully clarifies the roles each sensory impairment plays in the postural control deficits affecting those with T2D.
Path length
Persons with T2D showed significantly higher amounts of path length than the healthy group (p = .039), which aligns with previous literature.4,5 The path length was progressively greater across the various conditions, which also aligns with previous literature. 26 No significant interaction across mCTSIB conditions were found. This indicates that persons with T2D may not always have a singular predominant sensory impairment which has been previously suggested. 4 An increase in COP path length is associated with greater falls risk,30,32 though it is unclear through this type of analysis which (if any) sensory complications lead to increased falls risk for persons with T2D.
Percentile rank
Normalization of COP scores to anthropologic measures is common in the field of postural sway. The use of percentile ranking is a more recent approach to standardization26,33 that has yet to be utilized to describe sensory impairments in T2D.
Group-wise analysis of percentile ranks reiterated a main effect of group, indicating that persons with T2D ranked consistently lower than the control group. Though, the main effect between conditions became non-significant (p = .938). Seen in Figure 2, the average percentile ranks are almost identical across all conditions for each respective group, with the T2D group scoring significantly lower on all conditions. Considering the group-wise analysis of path length it was unclear if the T2D group had greater impairments in one condition over the other, but by using percentile rank it was determined that each condition had similar deficits in the T2D group. While it is unknown if any of the T2D participants had retinopathy or vestibular dysfunction, it was confirmed that they did not have DPN. Though they still had deficits in the proprioceptive condition equal to the other conditions. This finding shows that DPN may not be the primary cause of balance impairments in our T2D group, which does not support the findings of Bonnet et al. (2009).
With the group-wise approach, the meaningfulness of these percentile ranks is still limited since the distribution of individual sensory impairments is hidden. If impairment of one sensory system was highly prevalent, but only had a mild functional effect, it would be seen as the same as an impairment that is less prevalent but more functionally detrimental. Group-wise analysis of percentile ranks provides a deeper level of understanding through the standardization of path length to sex and age, but still limits the clarity of the sensory system impairments of the individual.
Individualized normative analysis
An alternative to group-wise analysis would be individualized case inspection against normative values. Frequency distributions are a common tool used to assess prevalence
34
and are often sorted by anthropometric measurements or age.
35
Distribution of percentile rankings (Figure 3) separates the percentile ranks of the T2D group into 4 categories: very poor, poor, good, and very good. Others have utilized this method with balance testing, such as the timed up and go,
36
but not as a percentile rank. This form of grouping allows for a better understanding of where the individual participants’ impairments lie instead of only presenting them as group averages. Frequency of participant with T2D percentile rankings during the four mCTSIB conditions; (a) Standard - eyes open on solid surface, (b) Proprioception - eyes closed on solid surface, (c) Vision - eyes open on foam surface, and (d) Vestibular – eyes closed on foam surface.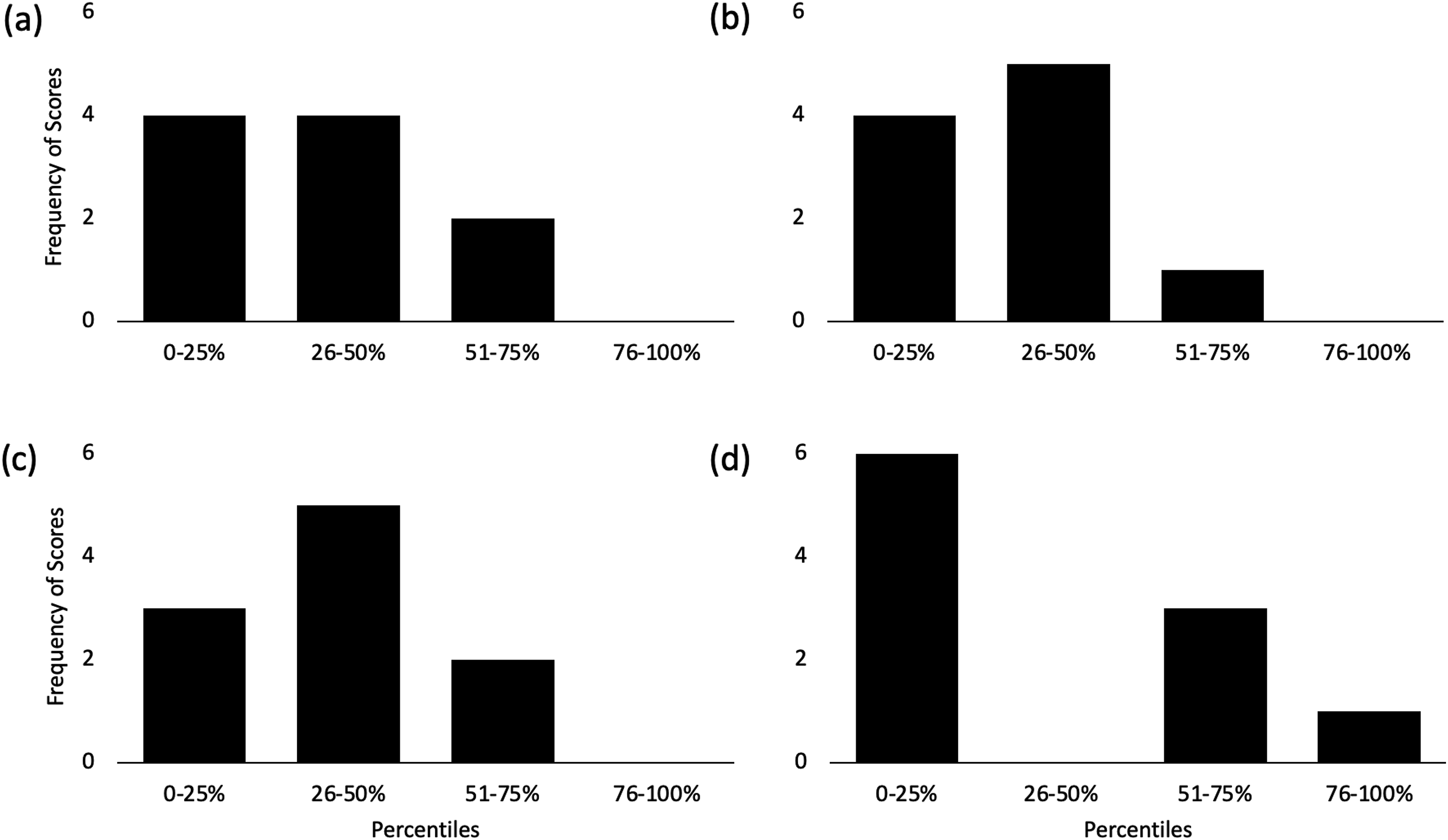
Group-wise analysis of both path length and percentile ranks showed that the T2D group had similar significant sensory deficits, which implies similar impairments for each participant. However, individual rank analysis (Figure 3) revealed variations in individual impairments. Three of the four conditions had a majority of participants scoring between very poor and poor. While the vestibular condition had 60% of participants scoring very poorly, none scoring in the poor category, and one in the very good category. This distribution shows that participants’ vestibular sense was either very impaired or not impaired at all, which is very different from what was seen through group-wise analysis.
The vestibular condition simultaneously had the highest and lowest scores of any condition and may reveal the level of effect that impairments to the vestibular system have on postural sway in T2D. These results suggest a possible “all or nothing” nature to the vestibular system, where those that have a vestibular impairment may only experience a severe functional effect, which align with other studies on vestibular vertigo. 37 The distribution of the proprioceptive and visual condition showed a possible progressive nature to the impairments of these systems, where a majority of participants showed a mild-moderate functional effect to their postural sway.
Argawal et al. (2010) is one of few to argue that vestibular dysfunction is the most common and primary sensory balance deficit seen in T2D. Individualized normative analysis of our data revealed the vestibular sense to be the most frequently severely impaired, which is more in line with the prevalence of sensory complications of T2D.9–15 Data in the present study indicated that the statistical design is important to reveal individualized sensory impairments of postural sway in T2D that would have otherwise been missed using group-wise statistics.
Impact & Limitations
This study highlights the importance of individualized normative ranking of balance performance to best reflect the prevalence of sensory complications in T2D. Though limited by the sample size of this study, the distribution of participants matches previously reported prevalence data of T2D sensory complications.9–15 This study is also limited in its ability to attribute sensory impairments to specific sensory complications of diabetes due to the mCTSIB protocol only recently being utilized for this population and purpose. Further research is needed to assess the validity and possible benchmarks related to diabetic complications when using the mCTSIB protocol. Further research examining vestibular dysfunction as a primary cause of instability in diabetes is warranted.
Conclusion
These findings show that examining the postural sensory impairments in T2D with an individualized normative approach should be used to provide effective patient-centered care. Though limited, the findings also suggest that impairments to the vestibular system may have a more drastic effect on postural stability than the proprioceptive or visual system. Further research is needed to assess the validity of using postural sway testing to assess sensory complications of T2D and the impact each complication has in this population.
Footnotes
Declaration of conflicting interests
The Author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Daniel Goble receives royalties paid to San Diego State University from a patent (US Patent 10660558) related to the balance technology in this study. In addition, he has an equity stake (i.e., stock options) and performs contract work for Balance Tracking Systems Inc., the parent company of the BTrackS Balance Plate and BTrackS Assess Balance Advance software. This conflict is mitigated by a management plan put in place by his academic institution (Oakland University) to ensure the integrity of his research. Mr. Lopatin, Mr. Ko, Dr. Brown, and Dr. Haworth has nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
Daniel Goble is a cofounder of BTrackS