
Abstract
This paper examines the place of theory in qualitative medical research. While theory’s place in research planning and data analysis has been well-established, the contribution of theory during qualitative data collection tends to be overlooked. Yet, data collection is not an asocial or apolitical process and requires reflection and analysis in and of itself. Therefore, drawing on an exemplar case study research project which focused on patients’ use of medicines, the paper argues that engaging with theory to think reflexively, throughout a project but particularly during the process of data collection can ensure the rigour and trustworthiness of qualitative data. In this case study, we draw on sociologist Erving Goffman’s theoretical framework of the dramaturgical metaphor to address the multiplicity of roles that healthcare practitioners undertaking qualitative research have to occupy and navigate. Rather than painting researchers out of their research through a naïve search for ‘objectivity’, reflexivity that is scaffolded by theory, offers a way through which researchers’ biases and subjectivities can be made explicit and their data analysis transparent. In making this argument, we encourage medical researchers to engage with, and be attuned to, theoretical perspectives outwith their own discipline.
Introduction
Given that many contemporary global health challenges call for diverse and interdisciplinary research approaches, healthcare practitioners and health scientists are increasingly stepping outside of traditional disciplinary boundaries to engage with qualitative methods. This methodological mobility can present philosophical, epistemological and ethical challenges 1 as well more practical considerations centred on the occupation of two roles (healthcare practitioner and qualitative researcher) simultaneously. In some ways, these roles are similar as both involve in-depth and often personal conversations, rely on a degree of trust and rapport and are underpinned by conventions of confidentiality. In other ways, although, these roles come into conflict with each other particularly around the expectation of interventions, whereby healthcare practitioners are expected to offer advice during interactions while qualitative researchers are not. 1 Moreover, while qualitative researchers try to rescind power as much as possible and position participants as the experts during research interactions, 2 shaking off the deeply established power associated with being a medical professional is not straightforward.
Given this complexity, this article explores how theory and processes of reflexivity can support healthcare practitioners to navigate issues of role-swapping during project design, data collection and data analysis, to make sense of their own place within, and effects upon, qualitative research. Such theoretically informed reflexivity ensures the rigour of qualitative data in the medical and health sciences field (where data quality is often linked to high participant numbers, generalisability and objectivity, 3 ) by explicating the theoretical perspectives of the researchers, improving transparency of the research findings.
While theory is always an integral part of qualitative research design and data analysis, 4 its value during data collection and to inform processes of reflexivity can often be overlooked in health and medical research. For example, Meyer and Ward provide useful guidance on integrating theory into qualitative healthcare research but do so by focussing solely on the research design and analysis stages. 5 However, data collection is not a mechanical, apolitical process but, rather, involves researchers actively engaging with and becoming a part of the social world they are researching. 6 This can bring researchers’ characteristics, attitudes and personal beliefs into sharp focus – all of which can ultimately affect the quality of data collected. This can be a particularly acute challenge for healthcare practitioners undertaking qualitative research as they navigate and occupy multiple social roles at the same time. In this article, we build on Meyer and Ward’s perspective to demonstrate that theory is also valuable for qualitative researchers as a lens through which to make sense of challenges during data collection.
To do this we use an illustrative exemplar case study of qualitative research into patients’ experiences of medicines adherence to demonstrate the use of theory ‘in action’ in research. This exemplar research sought to explore patients’ understandings of medicines and the effects of these understandings on medicines use. Existing research on medicines adherence has highlighted that approximately 50% of patients do not take prescribed medication as directed by their practitioners. 7 Poor adherence to medications can result in poorer health outcomes, economic loss, increased health systems costs and increased morbidity and mortality. 8 Current theoretical models of medication adherence disproportionately emphasise the identification of barriers and facilitators to adherence, targeting specific observable factors such as age, 7 sex, 9 ethnicity 10 and cognitive impairment 11 yet fail to address the complex social worlds where decisions about medication use are actually made.
Using smaller sample sizes to obtain rich data, qualitative approaches foreground lived experiences of medicines use.12,13 Within this paradigm, medicine non-adherence is not a simplistic case of variables, barriers and facilitators but is acknowledged as stemming from multiple social, cultural, familial and economic factors. Although these factors may appear irrational to healthcare practitioners, 14 qualitative research has repeatedly demonstrated rational decision-making processes underlying intentional non-adherence. 15
To understand the social dimensions of medicines use decisions, we collected rich qualitative data from chronically ill patients about their experiences of medicines use and their reflections on adherence interventions. To gather this data, APR, a registered UK pharmacist, conducted interviews and focus groups with 57 adults (≥18 years old) who had been prescribed medicines for long-term conditions (diabetes, chronic obstructive pulmonary disorder, cancer, gout and cardiovascular disease) in the last 6 months. These disease groups were chosen to provide a range of experiences of illnesses with different symptomatic profiles.
The findings of the study were twofold. Firstly, insights into patients’ lived experiences of medicines adherence identified that the experience of adherence was shared across disease groups. Participants’ decisions about medicines use were informed by the triangulation of diverse information from both formal and informal sources including doctors, pharmacists, nurses, friends and family and the internet. Moreover, use behaviours were linked to existing beliefs about, or inclinations towards, medicines use in general; participants who were suspicious of medicines or concerned about their ubiquity avoided medicines use.
The second key finding which is most pertinent to this article was methodological and relates to the transformational process required for healthcare professionals, trained within the natural sciences, to engage in, understand and apply interpretivist theories and approaches which centralise individual experiences and do not seek to produce generalizable findings to research. 1 While we anticipated some negotiation of these competing approaches, this proved to be far more extensive than we initially imagined and permeated each stage of the research project.
Occupying the (often competing) positions of qualitative researcher and pharmacist during this research presented multiple challenges and dilemmas which were navigated using theoretically informed reflexivity. To make sense of this role ambiguity we drew on theory, specifically Goffman’s Dramaturgy, to help us plan and carry out the research. Throughout this article, we continually refer to this case study project as a way to exemplify the central role of theory in qualitative health research. In particular, we elucidate the challenges and dilemmas of occupying multiple roles during data collection and explain how using theory helped us to address these challenges. First, we define what we mean by ‘theory’ and outline the ways that theory is most prominently entangled in qualitative medical and health sciences research – namely, through design, data collection and data analysis. In this, we argue that theory’s contribution to the data collection phase of research is substantial and should not be overlooked by qualitative medical researchers as it provides an invaluable way to address the identity of the researcher and complexities when occupying multiple roles.
Theory in qualitative research
Although ‘theory’ is seemingly ubiquitous across qualitative research, Morrison and van der Werf argue that it ‘defies simple definition’. 16 More alarmingly, Hervé Corvellec suggests that attempting to definitively answer the question what is theory? is ‘simply dangerous’ because it risks engendering dogmatic academic control and legitimising only one way of engaging with theory. 17 Instead, he argues that theory is understood and used differently across academic disciplines and encourages researchers to celebrate this diversity and eclecticism. Joas and Knöbl go a step further and highlight that even within disciplines, particularly the social sciences, the nature of theory, its objectives, mission and core concepts have not been determined. 18
Notwithstanding such ambiguities, Corvellec suggests that using and generating good theory which helps to understand and explain the world is a ‘collective quest’ in academic research. 17 Indeed, classical thinkers Immanuel Kant and Karl Marx commented similarly that ‘practice without theory is blind’. More recently, social psychologist Kurt Lewin commented ‘there’s nothing so practical as good theory’ 19 while educational theorist Martinus Jan Langeveld suggested ‘practice without theory is for fools and rogues’. 16
Despite these challenges in pinning down an exact definition, theory is accepted as a way to help shape research and make sense of its findings. For Meyer and Ward, theory is ‘concerned with the ‘how’ and ‘why’ of empirical phenomena’.5(526) They go on to suggest that theory is ‘a logical-deductive system consisting of a set of interrelated concepts from which testable propositions can be derived deductively’.5(226) We echo this understanding of theory in this article, positioning it as shorthand for a set of ideas and principles that explain and make sense of an observed phenomenon and are, to varying extents, applicable across space and time. In our case study project of medicines adherence, existing theory has sought to explain why large numbers of patients do not take medicines as directed by practitioners. Theories of non-adherence have made sense of this phenomenon through, for example, understanding patients’ balancing of the perceived necessity of using a medicine with concerns about adverse effects (The Necessity-Concern Framework); 20 through understanding patients’ lay constructions of risk and efficacy (Lay Pharmacology) 12 and through the patients’ physical and cognitive abilities and beliefs (Capability, Opportunity, Motivation, Beliefs (COM-B) model). 21
Although an important element through any research project, theory predominantly enters qualitative medical and health sciences research at two crucial points – planning and analysis. During planning, many researchers identify important theories through critical readings of existing literature to understand how others have explained a particular phenomenon previously and locate the research within a broader conceptual landscape. It should be noted that not all qualitative researchers engage with literature at this planning stage of research. Grounded theorists who seek to generate findings and insights entirely from data would actively avoid reading pre-existing theory at this stage of research and similarly, phenomenological researchers who wish to ‘bracket off’ previous experiences and knowledge may not see theory engagement during planning as a particular priority. For others, this critical reading allows qualitative researchers to arrive at their specific research question and identify what their research will add to existing theory. This might not only encompass asking novel research questions but also answering research questions in novel ways by, for example, conducting research in an under-studied population or using novel methods to generate new forms of data. In other words, through this critical reading, abstract concepts and theories become ‘researchable’ through the application of specific methods. 5 In our case study project, critically examining existing theories at the planning stage supported the development of our core research question and methodological approach. A deep analysis of extant literature highlighted to us an absence of qualitative research focused on medicines as ‘social objects’ 13 where decisions about medication use are made within everyday spaces, relationships and interactions.
Theory also takes centre stage during qualitative data analysis. For medical practitioners traditionally taught through quantitative approaches, qualitative data analysis is often considered ‘complex and mysterious’ and receives relatively limited attention in the literature. 22 Generally, qualitative research does not seek to quantify data and so analysis is not driven by identifying numerical patterns such as how many times a particular word is mentioned in an interview. 23 Instead, the majority of qualitative analysis is driven by the identification of salient analytical categories through the process of ‘coding’ which Charmaz describes as the ‘critical link’ between data and the eventual theorizing to emerge from it. 23
Although some qualitative methods such as discursive analysis or descriptive phenomenological approaches do not involve coding, our focus here is on those which do, namely, thematic analysis which we used in our case study project. Simply put, codes are shorthand devices to label and describe qualitative data which are then used to identify patterns and categories.
24
Codes, at this point, are purely descriptive interpretations of what is going on in the data. Figure 1 gives an example of this kind of descriptive coding using an extract from an interview with a diabetic patient from our case study project. Example of coded text. Coded text is shown in bold/black and descriptive code is shown above.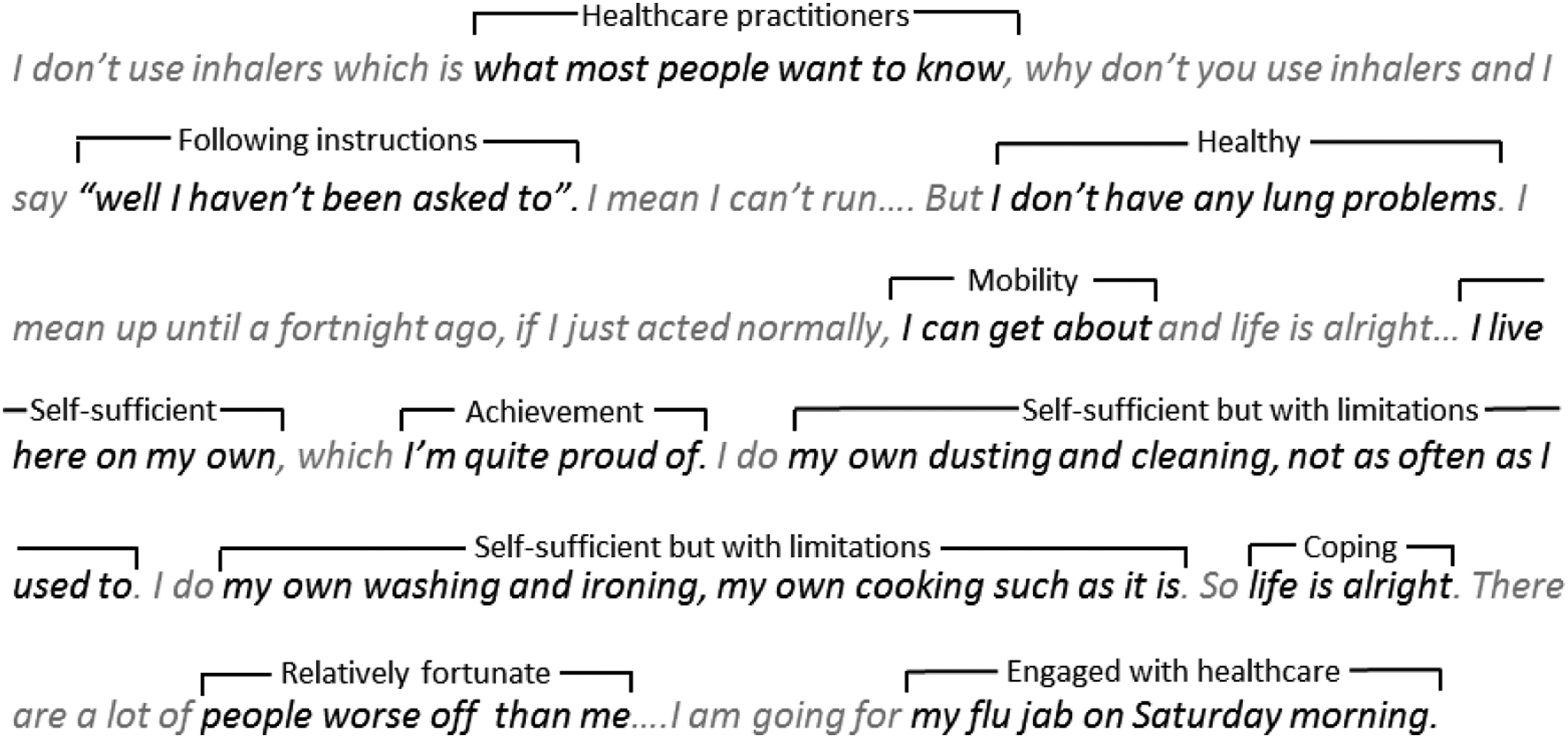
It is through theory during data analysis that researchers are able to move from this purely descriptive coding to understand what is going on here? Broadly speaking, qualitative researchers use theory in one of three ways during data analysis – to conduct a deductive, inductive or abductive analysis of their data. These approaches to data analysis differ in the relationship between theory and data, as demonstrated in Figure 2 where the use of these different approaches in our case study research is highlighted in the dashed boxes. Relationship between theory and data in deductive, inductive and abductive analysis.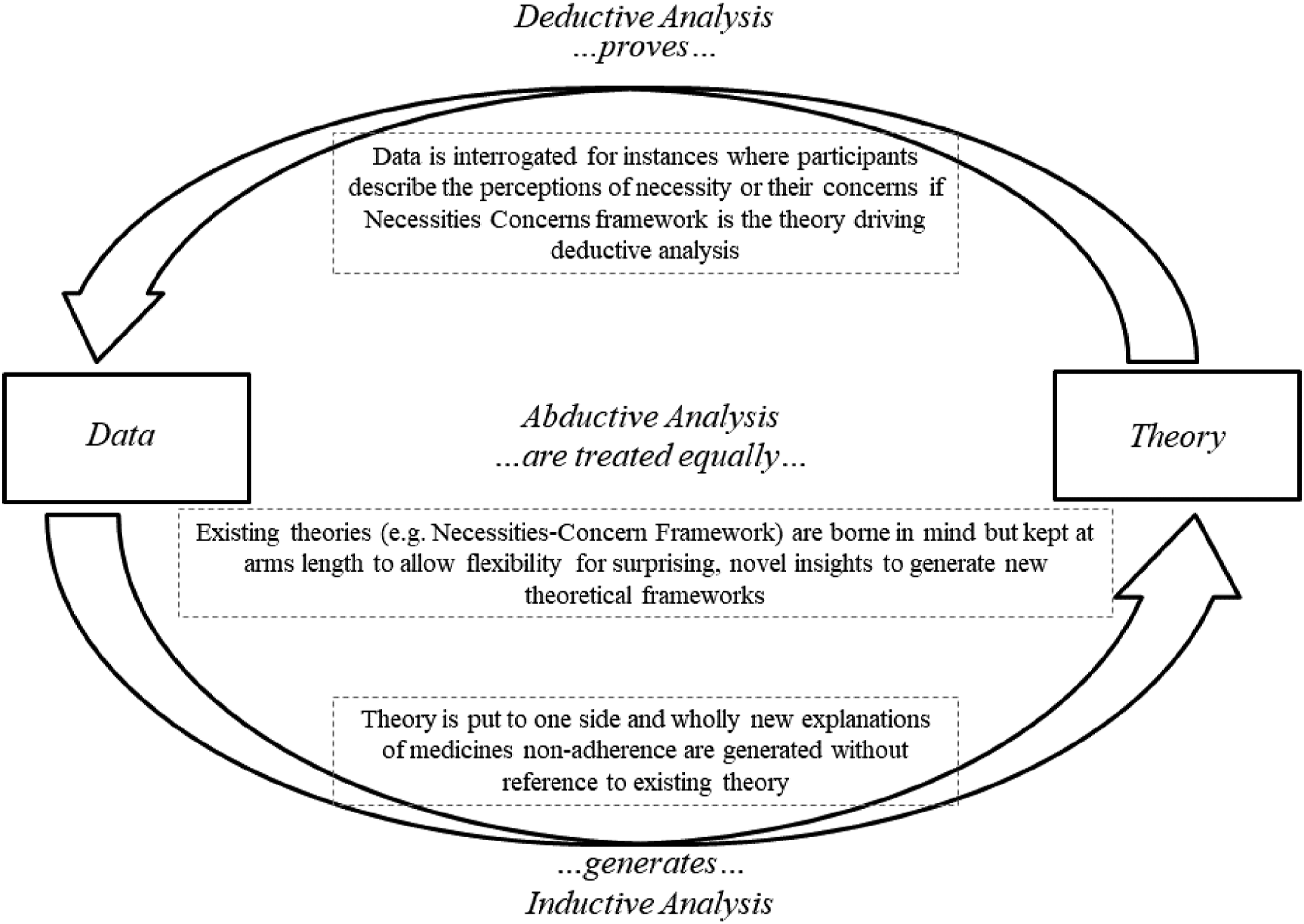
A deductive analytical approach takes existing theory as its starting point and interrogates data for areas where it confirms or contrasts with existing theoretical ideas. In this approach, coding is undertaken in line with the constructs of the particular theory which is driving data analysis. In the case of medicines adherence, the Necessity-Concerns Framework 20 might provide a lens through which the data is deductively organised and explored. In such an approach, data would be explored for mentions of the central tenets of this framework – the perceived necessity of using a medicine and patients’ concerns about adverse effects. To aid this deductive analysis, a particular theory may have also been used in research design where interview questions are specifically constructed around the key features of a theoretical framework (for example, participants might be specifically asked about their perception of a medicine’s necessity and their concerns where research is driven by the Necessity-Concerns Framework as a deductive lens). In this case, theoretical constructs are readily apparent in the data. In this sense, researchers already know some of what they are looking for when they begin to interact with data. 24 Such an approach can use multiple theories to drive data analysis where, for instance, the Necessities-Concerns Framework might be combined with another theoretical approach to non-adherence. Moreover, a deductive analytical approach might identify a theory’s shortcomings, nuances and areas for expansion or ‘prove’ its value.
In contrast to this, an inductive analytical approach seeks to generate new theoretical insights from the data alone. Here, theory might inform the project planning and data collection, however, should be ‘put to one side’ during the analysis. Or in the case of a ‘grounded theory’ 25 approach, researchers will have deliberately avoided any engagement with theory during project planning to prevent tainting findings with pre-existing conceptions. In taking these approaches of avoiding theory during planning or putting to theory to one side at the analysis stage, analysis is grounded in data from which findings ‘emerge’ 26 rather than being driven a priori by existing theory about a particular phenomenon. During inductive analysis when using a thematic approach or another coding-based method, researchers gain deep familiarity with data by reading and re-reading, before moving on to assign codes to the data. Through a process of constant case comparison, in which each code is compared with the rest of the data (rather than compared to pre-existing theoretical constructs), analytical categories or groupings, called ‘themes’ are generated. Once the most pertinent or salient themes have been identified, these are then used to form the basis of a new theoretical idea.
In practice, few qualitative researchers, including in our case study project, actually undertake a wholly deductive or wholly inductive analysis of their data. The problem with deductive analysis is that focussing solely on the tenets of existing theory leaves little room for nuance. Indeed, frustration with deductive analysis’ constant reproduction of existing theories underpinned the development of inductive approaches in the 1960s as researchers grew weary of data being ‘forced into the straight-jacket of pre-existing concepts’. 27 The problem with inductive analysis, though, is that it is extremely challenging to ‘bracket off’ previous theory, from both reading and general experiences in order to be entirely data-driven. Timmermans and Tavory point to an inherent contradiction in the key tenets of pure induction – while researchers should generate new theory without being beholden to pre-existing work, they still require some broad knowledge of existing theory in order to design studies and collect data to generate new theory. 27 Moreover, others have highlighted the practical challenges of wholly inductive analysis for novice researchers 28 and those bound by standardization required by ethics committees and Institution Review Boards. 29
Most qualitative researchers, then, undertake abductive analysis, which is both informed by researchers’ existing theoretical positions but also allows space for new theoretical reasoning. 30 In undertaking abductive analysis, researchers must be ‘neither theoretical atheists [as in inductive analysis] nor avowed monotheists [as in deductive analysis], but informed agnostics’. 27 The tenets of abductive analysis are drawn from philosopher Charles S. Peirce’s works on the logic and practice of natural sciences in which he argues that ‘discovery’ (through induction) and ‘justification’ (through deduction) are inseparable. 31 This inseparability became evident during our case study research project where our deep knowledge of the theoretical landscape gleaned through research design and planning necessarily informed our reflections on the meanings of our data. For example, participants talking about ‘needing’ to take medicines put us in mind of the Necessity-Concerns Framework yet we were not driven by ‘proving’ or ‘testing’ this framework.
Abduction, then, particularly centralises surprising research findings which call for new explanations. In our case study research, our participants extensively described devices to support medication compliance (known as multi-compartment compliance aids or dosette boxes) as symbolic of cognitive decline, old age and ill-health which was a finding we had not anticipated and which was not well-reflected in the extant theoretical literature on medicines adherence. Such findings can be alarming and there is undoubtedly a temptation to treat such data as an anomaly or indicative of a methodological issue. 5 However, these kinds of unexpected and non-conformist data can be the most interesting and theoretically insightful. Our unexpected finding that compliance aids are symbolic of ill-health required an openness to participants’ perspectives that allowed participant narratives to ‘give life and meaning’ to these inanimate devices. However, these findings also required familiarity with literature and practice that (i) understood social symbolism and symbolic interaction as forms of reality and (ii) was cognisant of professional practices and evidence that linked compliance devices with health deterioration and cognitive decline.
Abductive analysis, then, treats existing theoretical ideas as ‘sensitizing’ notions 32 which inform research design, planning and analysis but do not predetermine the frameworks within which data should be analysed. As such, researchers are encouraged to enter analysis having a broad knowledge of existing theory but keep this knowledge somewhat at arms-length. Timmermans and Tavory emphasised the recursive nature of abductive analysis and suggested that collaboration and sharing research ideas is crucial for the production and testing of new theory. 27 While there is temptation to form collaborations with and present work to like-minded researchers from our own fields, stepping out of disciplinary silos can introduce researchers to new theoretical landscapes. Interdisciplinarity can enhance the quality and breadth of abductive analysis as well as introduce different theory that challenges well-engrained disciplinary practices. Indeed, Stark reminds us that innovation emerges most readily when multiple, sometimes competing, perspectives, values and theoretical ideas are brought to the table. 33 In this vein, our research brought together theoretical frameworks from APR’s background of pharmacy and KJ’s discipline of sociology to produce a melting pot of diverse theoretical perspectives which we were able to deconstruct, adapt and adopt in innovative ways to analyse our data.
Theory’s absence from qualitative research: Data collection
Although theoretical perspectives are often well described within qualitative health and medical research design and data analysis to rationalise inductive, deductive and abductive approaches, there is limited work describing theory in data collection in this field of research. In their detailed step-by-step guide to qualitative healthcare research, Meyer and Ward mention theory’s relevance to data collection only in its informing ‘saturation point’ (where no new data is emerging) and to recommend analysis occurs alongside data collection. 5 That is not to say, however, that the role of theory or the complexities of research identity in data collection have not been considered. In social sciences, scholars have devoted, and continue to devote, considerable attention to debating these issues. Traditional grounded theory approaches are highly focused on ‘pure induction’ where new theoretical insights ‘emerge’ from data alone and the role of the researcher is downplayed. 34 In this approach, the reality of a particular research field is understood as a single objective truth independent of the researcher which can be ‘discovered’ if the researcher sets aside their personal biases to centralise the data alone. This traditional approach has been critiqued as naïve and Charmaz’s more recent developments in grounded theory approaches acknowledge that pure induction is near impossible as researchers ‘are part of the world we study, the data we collect and the analyses we produce’.35(17) As such, her constructivist grounded theory approach views research as a collective exercise involving researchers and participants and their respective interpretations of the world, and where the collectivity of the research process means researchers should explore multiple understandings of, and positions in, the social world including the researchers’ own. Despite these lengthy and extensive theoretically driven debates within social sciences, health qualitative research does not routinely engage with these discussions when it comes to the data collection process. Hence, data collection can often be presented as an objective, mechanical process of, for example, conducting interviews or undertaking observations. In this sense, researchers can fall into the trap of describing very well what they actually did during data collection but not reflecting on the impacts and implications of this from a theoretical perspective. This limits the transparency of the data collection and obscures the theoretical perspective through which data collection took place.
However, data collection (much like other aspects of qualitative research) is never an objective, apolitical process. Instead, it brings researchers’ characteristics, attitudes, biases and beliefs into sharp focus. As Malterud comments ‘a researcher’s background and position will affect what they choose to investigate, the angle of investigation, the methods judged most adequate for this purpose, the findings considered most appropriate, and the framing and communication of conclusions’. 36 In other words, researchers always occupy particular positions in society (as women, as middle-class, as people of colour etc.) and these positions taint our approaches to research, bringing the theoretical ‘baggage’ of our position to our research. Research is, then, influenced in often invisible ways by researchers at every stage, and should never claim to be objective. Chasing objectivity in qualitative medical and health sciences research (indeed any research) is naïve and, instead, researchers should strive to be as reflective as possible, being constantly mindful of implicit subjectivities engendered through social positions.
Data collection is no exception to subjectivity. While qualitative researchers seek to minimise their influence on research encounters, participants and their responses when collecting data (through, for example, not asking leading questions in interviews and asking standardized questions using topic guides), researchers’ characteristics and positions can themselves be influential and affect the quality of data collected. For example, feminist scholars argue that shared gender encourages women to speak freely with female researchers 37 while others note the importance of shared racial experiences in research encounters. 38 In other words, physical characteristics of researchers can have significant impacts on what research participants are willing to share. This creates an insider/outsider phenomenon where ‘insider’ researchers are often the best placed to collect data from participants with whom they share some kind of connection. Contextualising data collection using theory as a lens, such as unpacking insider/outsider relationships can improve the transparency of this process and understanding for other researchers.
Issues with the quality of data collection can arise when researchers undertake work with participants to whom they are ‘outsiders’ without considering the impact of this on the data collected or research outcomes. Researchers cannot, of course, alter their characteristics or social position. In some cases, problems presented by undertaking research as an ‘outsider’ can be predicted. For example, Sollis and Moser note that in highly gender-segregated societies, male researchers are unable to collect the same quality data as women. 39
In other research, issues arising from a researcher’s position may not be as obvious where, for example, the research is not on a particularly sensitive subject and does not have obvious political implications. However, researcher positionality is still a crucial factor in data collection and requires theoretically driven exploration in the presentation of research. In the next section, we highlight an example of ambiguous researcher positionality in our case study project, where a pharmacist explored patients’ lived experiences of using medication. We highlight the insider/outsider dilemma that arose during the project and the ways we used social theory and the practice of reflexivity to navigate this.
Reflecting on and presenting the self: Reflexivity in medical qualitative research
The Dilemma
Data collection in the case study project was undertaken by APR, a UK registered pharmacist. Since the research was focused on medicines use in everyday life, we sought to collect honest data about participants’ adherent and non-adherent behaviours. Given the research focus on the dynamism and complexity of everyday life and medicines’ place within it, data pertaining to non-adherence was actually the most interesting and relevant. However, obtaining this data about non-adherence presented something of a dilemma in terms of APR’s position as a pharmacist, specifically how he should represent himself to participants during data collection and if he should disclose his position as a pharmacist or not?
From one theoretical position (or on the one hand), disclosing his pharmacist status would have located him as part of the medical establishment, potentially reframing the interview encounter as something akin to a paternalistic clinical consultation; after all, a qualitative interview about medicines use is not wholly dissimilar to a medicines review with a general practitioner, physician or community pharmacist. In such an interaction, there is a risk that participants will modify their behaviour or stories to appear as ‘good’ patients. As Palmeieri and Stern point out, patients regularly tell ‘untruths’ in clinical settings in order to tell practitioners what they want to hear and to access services. 40 Given that a research interview with a pharmacist bears striking resemblance to a medicines review consultation, such untruths might be expected during data collection for this project.
The solution, then, seemed simple – APR should not disclose his position as a pharmacist in the interests of building rapport with participants and gathering the most relevant data. However, not disclosing this presented other issues from a theoretical perspective. Firstly, medical practitioners carry a high status which can be beneficial for recruiting participants for research. Not disclosing his pharmacist identity would have removed this expert position, reducing his status and potentially reducing the success of participant recruitment. Secondly, not disclosing APR’s pharmacist status would have removed his right to counsel patients if a safety issue, such as risky non-adherent behaviours, became apparent during a research interview. As such, the dilemma around whether to disclose is not just a methodological question but also an ethical quagmire given that non-disclosure effectively removes the ability to reduce harm to participants if necessary. 1 Finally, suppressing APR’s role as a pharmacist would have been something of a deception. While there is no obligation on qualitative researchers to disclose personal details, there is an expectation that participants will be informed of relevant information. There is, of course, a debate to be had around whether being a pharmacist is relevant to a project on medicines use being undertaken entirely separately from pharmacy service delivery. However, such a debate is moot given that professional ethical frameworks (based on bioethical theory of benevolence and non-maleficence) compel UK pharmacists to always intervene if the inappropriate use of medication is disclosed.
The dilemma in the case study research, then, was not about whether to disclose APR’s role as a pharmacist but rather how to manage the theoretical juxtaposition of his simultaneous roles as healthcare practitioner and researcher to ensure the collection of good quality, relevant data. The actions and impressions of each character, a pharmacist and a researcher, would need to be played simultaneously, but carefully. To do this, we engaged with the process of reflexivity.
Reflexivity
Simply put, reflexivity involves researchers considering themselves and their practice to make implicit biases and effects explicit. 41 As such, qualitative researchers do not seek to paint themselves out of research but to be open, honest and explicit about the ways the research may be influenced by any given researcher. It is a means of holding both subjective and objective roles in relation to the participant and the data produced, acknowledging that researchers are both close to, and distant from, participants and data which themselves exist within particularly interpersonal networks. 42 This is different to reflexivity in education and professional development which is more closely aligned with reflection, and personal and professional development. Reflexivity is not simply reflection. 43 It is not a case of asking what went well in that interview? and how might I do better next time? Granted, reflection of this nature is important in qualitative research but reflexivity goes beyond that to locate the researcher as a dynamic, active participant in the inherently social interactional space of research and the knowledge produced from it. 42 Woolgar’s notion of a continuum of reflexivity is useful to further explain this. 44 At the one end of the continuum is ‘benign introspection’ (or reflection), which is concerned with the process of research and the verification of results where researchers ask themselves, for example, how well their research captured the perspectives of research participants and how accurately methods were reproduced across participants. This positions the topic of research as separate to, and removed from, researchers, their lives and experiences where the truth about a particular phenomenon is best captured through the use of standardized methods.
Reflexivity sits at the other end of the continuum and turns the evaluative gaze away from the deployment of research methods and on to the researcher themselves. This approach does not privilege one theoretical position about a particular phenomenon but, rather, understands social life as constituted by multiple actors, experiences, structures, perspectives and knowledges. 45 As such, the research encounter and the researcher themselves are implicated in this dynamic landscape and the process of reflexivity is focused on untangling just how that is. Below we suggest that drawing on theoretical frameworks can be a useful lens through which to do this untangling work.
While the necessity of reflexivity is clear, the question of how, practically, to be reflexive is more opaque. We suggest that keeping a reflexive journal and using the content of this journal as an entry point into theory, which in turn enhances the rigour of reflexivity, is a useful approach for engaging with a systematic process of reflexivity. Reflexive journals are not intended to record the process of research (e.g. methods and findings) but, rather, to archive researchers’ subjectivities, beliefs, attitudes and thoughts throughout the lifetime of research, including planning and writing-up phases. Ortlipp provides an excellent account of her reflexive journal-keeping during her qualitative doctorate, noting in particular the circular effects of reflexivity as her research design continually evolved in light of her reflection.
46
Moreover, she gives good examples of the sort of things researchers might focus on in reflexive journals. She writes, for example: “I felt strange acting in the role of interviewer … Because of my relationship with three of the participants…I knew that they knew my perspective on assessment to some degree. I didn’t put this out in the open, and wonder if I should have? I felt as though it was a bit fake and not like the equal conversation that it could be if we just sat around and discussed assessment issues and if I felt free to say more… The dual role of interviewer and ex-colleague/friend was difficult. Also, having my own opinion and experiences and wanting to join in the discussion was an issue, however I did resist this.” (Research journal, 29/3/00)
These kinds of reflexive, unstructured and personal accounts of researcher positionality can be triangulated with research data to produce an audit trail where researcher bias is not eliminated but dealt with explicitly, centre-stage. 47 Integrating this kind of reflexive writing with qualitative data can be challenging as researchers should not undermine their data by overly attributing participants’ narratives to researcher influence. However, giving these reflexive accounts equal, or at least some, space within research publications and reports is a good way to both qualify potential bias or researcher influence, and to engage in debate about issues like subjectivity, impact and researcher positionality on data collection and analysis. The Discussion section of academic papers, student theses and research reports are good places for this debate yet are often side-lined in favour of standardized descriptions of research processes, limitations and ideas for future work.
Theoretically informed Reflexivity
In the case study research, it was through the use of a specific theory that informed the process of reflexivity that we identified the issue of identity duality as one with potential impacts on data quality. To make sense of the dilemma and how we might best navigate the issue, we turned to theory. Engaging with theory to inform and analyse reflexive journal entries enhances the credibility of reflexive practice and can also lend insights into analysis of research data. We particularly identified sociologist Erving Goffman’s work on ‘dramaturgy’ as particularly useful. Briefly, Goffman’s theory uses the analogy of a theatrical performance to highlight the ways in which people engage in ‘impression management’ and present themselves to others in diverse ways depending on context and audience. 48 Partly taking his lead from Jacque’s monologue in Shakespeare’s As You like It, Goffman argued that people adopt different masks to play different roles in social interactions depending on the expectations of a particular situation and how individuals wish to be perceived within it. For Goffman, people (actors) both give and give off impressions; impressions are given through purposively used props and verbal signals, whereas impressions are given off through non-verbal cues that verify, or undermine, the impressions actors give. The theatrical analogy continues in Goffman’s treatment of the physical and symbolic spaces of such performances and he distinguishes between front and back regions, or front- and backstage. Performances on the frontstage are given with the audience in mind and carefully managed according to the formal and informal rules governing that particular space, while actors backstage are able to relax and often deliberately shake off the impressions cultivated frontstage. To demonstrate this, he used the example of restaurant waiting staff moving between formal frontstage performance in the dining room where guests are served and the backstage region of the kitchen where gossip, swearing, sexual remarks, ‘sloppy’ posture, shouting and playing are common. 48
While Goffman’s theory has been critiqued for focussing too closely on everyday mundanities rather than wider social structures, it continues to hold traction in the social sciences as a framework for understanding self-presentation. 49 Recently, for example, researchers have examined the relevance of Goffman’s work in the online world, applying his notion of impression management to Second Life, 50 social media 51 and online dating profiles. 52
Goffman’s analogy of masks seemed an entirely appropriate theoretical lens through which to consider self-presentation in research encounters during the case study research. Given that we wanted to collect honest data about participants’ use of medicines even where this use might be non-adherent or risky, we designed the research so that when interviewing, APR’s onstage identity was that of a researcher, not a pharmacist. Although health professionals are well-versed in emotional labour, 53 we felt that the potential power asymmetry 54 between APR and our participants presented a significant risk that participants would feel compelled to act as ‘good patients’. As such, Goffman’s theory was used to facilitate discussions with participants, explaining to them that APR’s role in the interview encounter was as an open-minded researcher and that, although was also a pharmacist, this pharmacist identity would by ‘put to one side’ during the interview. The success of swapping masks or identities is reliant upon a degree of audience complicity. 55 Not only must the performer deliver their ‘lines’ convincingly to control the impression that they are giving, the audience must also be willing to believe and be convinced by the identity performance being given. Using theory through Goffman’s mask analogy to navigate the potential complications of inhabiting dual roles built rapport between researchers and participants through conversations about identity and authenticity in the research encounter. While most decisions around mask-swapping are consciously or unconsciously kept from audiences (to facilitate a more convincing performance of an ‘authentic’ self), we actively engaged participants in conversations about APR’s diverse roles, masks and identities, and which he would occupy during the research. In doing so, we made audience complicity explicit and actively asked participants to be complicit in ARP’s performance while he inhabited a researcher (rather than pharmacist) role. We believe that APR stepping outside of his pharmacy role and engaging participants in conversations about this decision led to better quality, more honest data about medicines use and, crucially, misuse.
As well as helping us to design and carry out our data collection, we also employed Goffman’s theory to help our data analysis. Adopting the perspective of a pharmacist, the analysis might use a positivist perspective to dissect participants’ experiences of adherence to identify facilitators and barriers, linking responses to stimulus, focussing on specific medicines using a pharmaceutical gaze. However, adopting a social science perspective, the analysis could remain open to, and engage with, participants’ constructed life worlds and medicines use within it, using a sociological imagination to understand lived experience.
However, just as an actor can move between the front- and backstage regions, APR could move back to his pharmacist identity to support participants as a pharmacist, if needed. The metaphorical ‘researcher mask’ and ‘practitioner mask’ are inter-changeable and can be deployed at the discretion of an individual within any given context – be it clinical or research-oriented. This approach enabled APR to fulfil his commitment as a qualitative social researcher (who traditionally would not be expected to intervene), as well as fulfilling his professional obligations as a pharmacist (who is statutorily compelled to intervene). For example, when participants disclosed potentially dangerous medicines use practices, APR was able to adopt his pharmacist mask to offer advice. It should be noted, however, that moving to the ‘practitioner mask’ in this way was only ever done at the end of the interview itself to ensure that this role slippage did not disrupt the flow, rapport or quality of the data collection.
Engaging with Goffman’s theory of self-presentation presents a novel approach that enabled the navigation of ethical and legal concerns, while undertaking robust data collection using a method that was theoretically sound. Goffman’s theory of identity helped us to be flexible, providing a theoretical scaffold to understand and navigate the role of the researcher on data collection and analysis. This ensured that the study design and data collection were carried out rigorously and transparently by providing a theoretical backdrop to support our decision-making and ensuring the context of our findings are explained to other researchers. Contextualising the design, data collection and analysis of the case study project to specific or multiple theoretical positions can help readers understand the how the project was conducted in action. Exposing and making explicit researchers’ theoretical positions improves, in our opinion, the dependability and rigour of the findings.
Identifying and using this specific theory was only possible because researchers had a degree of knowledge of broad theoretical landscapes outwith medical or health sciences disciplines. While an in-depth knowledge of theories from across diverse disciplines is practically challenging, we advocate for an open-minded approach and, where possible, interdisciplinary working for medical and health sciences researchers to find the most appropriate theoretical frameworks for navigating complex issues during data collection.
Concluding remarks
Theory is important in all aspects of qualitative research. In this paper, we have outlined the place of theory in qualitative research planning, data analysis and data collection. We have particularly attended to the question of theory in processes of data collection which can be overlooked in qualitative research reports. We have argued that since data collection is not an asocial process, and researchers always bring subjectivities to their research, theory can provide a useful tool for navigating and articulating these complex issues. In doing so, we have extended Meyer and Ward’s 5 approach to the integration of theory into healthcare research which focused solely on theory’s relationship with research design and data analysis. To do this, we have drawn on an illustrative exemplar case study of research on medicines use and our employment of sociologist Erving Goffman’s dramaturgical theoretical perspective to manage the competing expectations that occur when healthcare practitioners enter into new roles as researchers. To deal with such complexity, we introduce reflexivity as a practice to locate researcher bias from the outset. By using reflexivity to identify Goffman’s dramaturgy as a way to underpin our approach to data collection, we have identified a mechanism by which dual-identity healthcare professional researchers can engage in high-quality data collection. Medical and health sciences researchers’ engagement with theory around identity and role-swapping is not limited to Goffman though. Other theory-informed approaches to data collection could draw on Foucault’s work on power, using this theoretical framework to weigh up the balance of power between researcher and participant during data collection. 56 Alternatively, McIntosh’s ‘white privilege’ framework might be useful to untangle the politics of race and ethnicity in data collection encounters. 57 By using theory to underpin methods of data collection, healthcare professional researchers will be demonstrating reflexivity.
In making our argument, we advocate medical and health science researchers being attuned and open to theoretical perspectives outside of their own discipline. As the academic world becomes increasingly globalized and inter-disciplinary 58 such boundary-crossing will not only become commonplace, but also increasingly necessary. Shifts in medical and health science education towards, amongst other things, social determinants of health, clinical skills and communication competence 59 will bring both researchers and students into contact with theoretical frameworks from non-medical disciplines. Within this somewhat eclectic theoretical landscape, we encourage medical and related health researchers to use theoretical ideas in the way French philosopher Michel Foucault suggested – as ‘a kind of tool-box [to] rummage through to find a tool which they can use however they wish in their own area’. 59
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.