
Abstract
In March 2020, the ‘Everyone In’ initiative was introduced by the UK government as a public health response to COVID-19. This initiative sought to temporarily accommodate people experiencing rough sleeping in hotels in all local authority areas throughout England. In London, ‘Everyone In’ involved the procurement of vacant accommodation in over 100 hotels and temporarily re-housed approximately 2000 individuals. A rapid qualitative study was undertaken within two hotels to explore experiences of the initiative from the perspective of people accommodated in the hotels. This article describes how standard qualitative methods were adapted and implemented to complete the study whilst meeting COVID-19 social distancing guidelines. The research involved a longitudinal design of a two-stage qualitative interview that sought to capture residents’ experience of ‘Everyone In’ at two points in time (while in the hotel and when residents had left the hotel). Adapted qualitative methods were employed by a team of 13 researchers. These adaptations included socially distanced leaflet dropping, telephone-based participant recruitment, a remote, multistage, longitudinal qualitative telephone interviewing and rapid framework analysis. 35 hotel residents were recruited into the study (two subsequently withdrew participation). A total of 299 (of a possible 330) short interviews were completed by 33 participants (26 male and 7 female) as part of the multi-stage, longitudinal design of the study. This study indicates that adapted qualitative research methods employed during a pandemic can be successfully applied to obtain insights and experiences (of individuals and groups) otherwise difficult to reach and/or complex to understand.
Keywords
Introduction
The global spread of the coronavirus (SARS-CoV-2), that causes COVID-19, has had (and continues to have) a devastating impact upon human health and society since its detection in late 2019. At an international level, the COVID-19 pandemic has created economic crises, restricted the worldwide movement of people and been responsible for an estimated 88+ million infections and almost 2 million deaths throughout the world, 1 of which over 73,500 2 occurred in the United Kingdom during 2020 alone (and rapidly rising during the early weeks of 2021). At national levels, public health control measures have been introduced to try to reduce the spread of the coronavirus and protect individuals. Across all four nations of the UK, these measures included an initial 12-week nationwide ‘lockdown’ that commenced on 23 March 2020. This lockdown involved the partial and/or complete closure of businesses including non-essential shops, restrictions placed on travel and meeting family and friends in homes and outside. In addition, anyone who tested positive for SARS-CoV-2 or suspected to have contracted it was asked to socially isolate for 2 weeks. Additionally, those at substantially high risk of severe morbidity or mortality from COVID-19 (such as people with specific cancers or severe respiratory conditions) were asked to ‘shield’ (stay at home and socially distance from household members). 3 These measures significantly impacted upon the economy, employment, travel, food supply and, of course, all social contact, human interaction and mental health.
In England, the strategic response to COVID-19 was (and continues to be) led by central government’s Department of Health and Social Care (DHSC) in conjunction with Public Health England (PHE). Whereas the former is a ministerial body responsible for the shaping of government policy, the latter is an executive agency, sponsored by DHSC, which provides evidence-based scientific support and advice to local and national government (as well as other organisations) 4 . As such, PHE typically provides scientific evidence that informs health-related policy and practice at a government level as well in matters relating to managing public health (e.g. reducing harms caused by diet or substance use). However, these protective measures posed significant difficulties for people with current experience of homelessness.
People who are homeless and who experience rough sleeping frequently experience other physical and mental health problems, and substance use disorders.1–6 Similarly, people with a recent (within the past year) diagnosis of a mental health disorder – or substance use disorder – may also have an increased risk for COVID-19 as compared to patients without, and may also have worse outcomes (such as higher rates of hospitalisation and death).7,8 In addition, people who are homeless and who experience rough sleeping are by definition unable to follow government guidelines that advocate ‘stay at home, protect the NHS and save lives’. 5 As such, they are also likely to have a higher risk of acquiring COVID-19 given they tend to have limited access to water and sanitation,9,10 live in close proximity to others and have restricted capacity to self-isolate and protect themselves. 11 Infectious disease outbreaks, such as COVID-19, generate fear and anxiety that can undermine otherwise good mental health and worsen pre-existing mental health problems. 12 For people who experience rough sleeping, this is likely to be exacerbated by the closure of many support services and day centres, increased social isolation and loss of income. People who are homeless and who have substance use disorders additionally experience other health problems which may place them at heightened risk of COVID-19.1,13 For example, people using opioids and stimulants are at increased risk of chronic lung disease and other respiratory problems.14–16 They may also be less able to recognise COVID-19 symptoms as these might be confused with opioid and alcohol withdrawal. Furthermore, they may be at increased risk of fatal opioid overdose if they do become infected with COVID-19. 17
As part of lockdown procedures during March 2020, the government’s Ministry for Housing, Communities and Local Government (MHCLG) implemented a policy initiative called ‘Everyone In’. This emergency directive aimed to provide temporary accommodation for every person experiencing rough sleeping in all local authority areas across England, 18 in an attempt to facilitate and safeguard national social isolating/distancing measures. As part of this programme, the government initially announced £105m to provide interim housing during the pandemic, including £16m for people in emergency accommodation to access specialist help for substance mis/use. In addition, ‘Everyone In’ aimed to prevent localised and concentrated outbreaks of COVID-19 amongst people experiencing homelessness whether they resided in street-based settings, shared rooms in shelters, hostels or within houses of multiple occupancy in order to avoid communal gatherings around shared facilities (washrooms, kitchens, sleeping areas, toilets, laundry-rooms, etc.). 18 This initiative therefore aimed to remove or minimise the environmental and social conditions that are conducive to the spread of infection. 6
In London, the ‘Everyone In’ initiative was coordinated by the Greater London Authority (GLA), and the capital’s 33 local authorities (aka borough councils). These organisations facilitated a strategic approach that sought to bring together devolved homeless policies across London. The temporary housing concerned typically took the form of vacant hotel rooms that were subsequently procured by the GLA and London borough councils across the capital (and managed by a number of charitable organisations). Over 100 hotels were involved in the initiative in London (and over 300 nationally) and organised as a three-tier system of care, in which each hotel was designated as COVID Care, COVID Protect or COVID Prevent. This nationwide, best practice, categorical system was designed to triage people to the most appropriate accommodation based upon their level of risk and vulnerability to COVID-19. COVID Care hotels provided accommodation to those either testing positive or displaying and reporting symptoms of the disease, COVID Protect hotels provided accommodation to those considered most vulnerable to the disease as a result of underlying health conditions and COVID Prevent hotels were those that provided accommodation to all other people who were homeless or experiencing rough sleeping. In London, this system was facilitated by the formation of the Homeless Drug and Alcohol Service (HDAS), commissioned by the Mayor and City of London. HDAS, as a ‘pan-London system’ involved collaborative partnerships between South London and Maudsley (SLAM) and Central North West London (CNWL) NHS Trusts, working with various charitable organisations such as Change Grow Live, Phoenix Futures, Turning Point, Westminster Drugs Project (WDP) and We Are With You. 19
This article describes methods employed during a focused and rapid qualitative study of two of the London hotels involved in the ‘Everyone In’ initiative. The study was never intended to provide an evaluation of the full initiative across London, due to the number of hotels involved (>100), the lack of available resources in the team/department and because the study was conducted on an unfunded basis. Instead, the aim was to explore the experiences of the initiative from the perspective of people accommodated in one or two of the hotels in order to provide rapid and focused feedback to the various key stakeholders and commissioning bodies. Members of the team had connections with HDAS, which, in turn, had links with the various organisations and charities managing the hotels. At the start of the pandemic, these organisations and charities were under significant pressure establishing and running the accommodation. However, they were also simultaneously experiencing requests from many researchers who wanted to study the initiative. This made access to the hotels difficult but eventually (after a delay of approximately 2 months) the research team were permitted to conduct the research in two sites. Ethical approval was granted by King’s College London (KCL) Research Ethics Committee (REC) on 01 May 2020 (CREC-HR-19/20-18676).
The article commences with a descriptive summary of the design and delivery of the qualitative research project. This account includes an overview of the various processes attached to the use of assorted methods (and their adaptation) that were (by design) consistent with the conduct of socially distanced fieldwork and socially distanced data generation. This is followed by a more reflexive account of these methods in which the adapted methods are discussed in terms of qualitative methodology, and with regard to their relevance to ongoing (and future) qualitative research in a post-COVID era.
Socially distanced qualitative research: design, method and analysis
During June–November 2020, rapid qualitative inquiry20,21 was used to evaluate the London hotel initiative using two hotels as fieldwork sites. Rapid qualitative inquiry adopts a team-based approach to reduce time ‘on the ground’ whilst in the field during data generation and analysis. Qualitative research can provide rich data and is particularly useful when trying to understand the implementation of complex interventions in a real-world setting. The research was undertaken from the perspective of people accommodated in the two hotels using a qualitative longitudinal and socially distanced design. Data were collected from residents at regular intervals whilst the hotel was providing accommodation and for up to 5 weeks after residents left the hotel (either to move to another hotel or back into the community). Data generation was designed to be as simple, flexible and non-burdensome as possible to maximise the chances of obtaining data from as many residents as possible.
The following section provides a descriptive account of the methods that were employed during this 6-month period of rapid qualitative data generation. It is organised into two subsections, namely ‘preparing for socially distanced fieldwork’ and ‘conducting socially distanced fieldwork’.
Preparing for socially distanced fieldwork and data generation
Once ethical approval for the study had been granted, a team of KCL researchers were recruited to assist with the research at a time when all KCL staff had been advised to work from home (where possible). The Joint Principal Investigators managing the unfunded study recruited a team of researchers already working in substance use research, within the National Addiction Centre (KCL), to take part in the study on a voluntary basis. Notification of the study and associated opportunities were broadcast using a variety of internal channels (e.g. departmental meetings, staff email and notice to line managers).
A total of 11 researchers volunteered as field interviewers for the study, with each offering varying levels of availability. Interviewer recruitment occurred at two points during the study, in which six interviewers were initially recruited at the onset of the study (May 2020), followed by a further five interviewers in July 2020. This second phase of interviewer recruitment took place due to the number of residents who wished to participate in the study and the consequent need for additional interviewer capacity. The time volunteered to interviewing during the study ranged per individual interviewer (from approximately 4 h to over 28 h) and was dependent upon interviewers’ availability or upon the number of residents within each interviewer’s ‘participant caseload’ (ranging from 1 to 7 residents).
The KCL researchers who volunteered had varying levels of experience in conducting qualitative research interviews with people who are homeless. For example, several of the interviewers were established qualitative researchers in this field, others had experience of qualitative research as a result of contributing to mixed methods studies of alcohol and other drugs (AOD) and others’ qualitative research experience was informed by telephone-based interviewing as part of randomised controlled trials. Preparation for socially distanced fieldwork involved a period of home-based orientation (reading study materials) and online training, which occurred at each of the two points of interviewer recruitment (May and July 2020).
Online training took place via the communication platform Microsoft Teams 6 . These 2-hour sessions were designed and delivered by the Joint Principal Investigators of the study and provided an overview of the study, tasks required of the interviewer team, training on interview skills and techniques, data management and storage and the application of a distress protocol (to be implemented should the resident/interview participant express an intent to self-harm, or report other potentially harmful circumstances).
Conducting socially distanced qualitative fieldwork
All interviewers involved in this study were based at home throughout the study and were not permitted access to the university campus or to conduct face-to-face interviews with research participants. As such, members of the team worked remotely from home and were concentrated mainly around the London-area. Others worked from locations outside of the London, for example, in Hampshire, Kent, Suffolk, Yorkshire and even Germany. Therefore, throughout the study, almost all the team were completely removed from the main fieldwork settings and never visited the two hotels during the 6 months of data collection. Indeed, only three members of the team actually visited the field locations in order to conduct socially distanced distribution of the study information sheets and consent forms.
Socially distanced distribution of the study information sheets and consent forms
Three (female-identifying) members of the team received permission from the two charities managing the ‘Everyone In’ hotels in the study (henceforth Hotel A and Hotel B) to deliver the Participant Information Sheet (PIS) and Informed Consent Forms (ICF) providing information about the study to the hotel residents. In order to maintain social distancing regulations, visits were arranged in advance (with designated time and place) and required the researchers to wear face coverings and plastic gloves throughout their respective visits. Once at the hotel, an information pack (consisting of the PIS/ICF) was placed outside of the door of each residents’ room. Permission was also granted to knock on room doors, hand deliver the information pack and briefly explain the study (while wearing mask and gloves at a safe distance) if the resident was in their room at the time of the visit. In one of the hotels, a member of the charity also accompanied the researchers as they delivered the information packs.
This system of contacting residents to recruit them into the study was negotiated with the charities managing the hotels and agreed with KCL REC. It was not possible for hotel staff to assist in the recruitment of residents due to their limited time and capacity. Although residents had landline telephones in their rooms, it was not thought ethical, without residents’ prior consent, to provide researchers with these numbers. However, as most residents had been issued with a new mobile phone, free of charge, as part of the ‘Everyone In’ initiative, there was the potential for people to ‘opt in’ to the study if they were made aware of its existence. Accordingly, the information pack provided details of the study contact number, which residents could call if they wanted to participate.
A total of six socially distanced PIS/ICF leaflet deliveries took place throughout the study, involving four visits to Hotel A and two visits to Hotel B. Approximately 300 leaflets were delivered during all of these visits. Whereas the initial visits to each hotel were speculative (in terms of informing the residents of the research) all subsequent visits were intended to boost the number of residents recruited into the study. The initial visits to Hotel A and Hotel B took place on 11 June and 18 June 2020; second visits were made to each location in July 2020 (at a time just before Hotel B was closed and withdrawn from the ‘Everyone In’ initiative) and third and fourth visits to Hotel A were made on 17 August and 10 September 2020 (the latter to specifically increase the number of people in the cohort who use/d drugs and/or alcohol). During the initial visits in June, England was in full lockdown and residents were typically requested to spend most of their time in their hotel room. During the July visit, lockdown restrictions had eased throughout the UK and residents were more able to spend time outside the hotel. By the time of the final visit during August and September, measures in the relevant areas of London were more relaxed and less restrictive, despite concerns of a second rising peak of COVID-19 at that point in time. On 30 September 2020, Hotel A was also closed and withdrawn from the ‘Everyone In’ initiative and all residents (regardless of participation in the study) had been rehoused or moved-on to next step temporary accommodation.
Regardless of when the information sheets were delivered, it was the residents’ individual decision to opt into the study by calling or texting a dedicated telephone number contained within the PIS. This was the mobile telephone number of the Research Co-ordinator who was responsible for the recruitment of residents into the study as research participants.
Recruitment, eligibility and screening
When residents called the dedicated telephone number to express their interest, the Research Co-ordinator explained the study to them and/or answered any questions asked about the research. Although all residents were eligible to take part, it was a requirement that residents could understand and communicate effectively in English. As such, the initial conversation sought to determine that the resident had received and read the PIS/ICF and that they understood the nature of the study. Residents were given the opportunity to ask questions about the study. If the Research Co-ordinator was satisfied with the level of English language ability, the resident was asked whether they agreed to taking part in the study and, if so, they were allocated a unique study identity number. The resident was then informed that ‘another KCL researcher called (name of interviewer) will be in touch at your preferred time’.
A total of 35 residents were recruited into the study during June– September2020
7
(31 from Hotel A and 4 from Hotel B). In addition, six residents were excluded from the study because of limited English language ability. Of these, four had requested a translator (or had asked another person to call on their behalf). Two residents, who spoke English as a foreign language (EFL) subsequently withdrew from the study after expressing fears about the intent and purpose of the research. The final dataset consisted of 33 participants who were residents of the two hotels (see Diagram 1). Participant Flow Diagram. Topic A: Personal Circumstances Topic B: Housing and Homelessness Topic C: Alcohol and Other Drug Use Topic D: Smoking Topic E: Health (Physical and Mental) Topic F: Support and Services Accessed Topic G: Relationships and Social Distancing Topic H: Use of Technology Topic I: Expectations About Life After the Hotel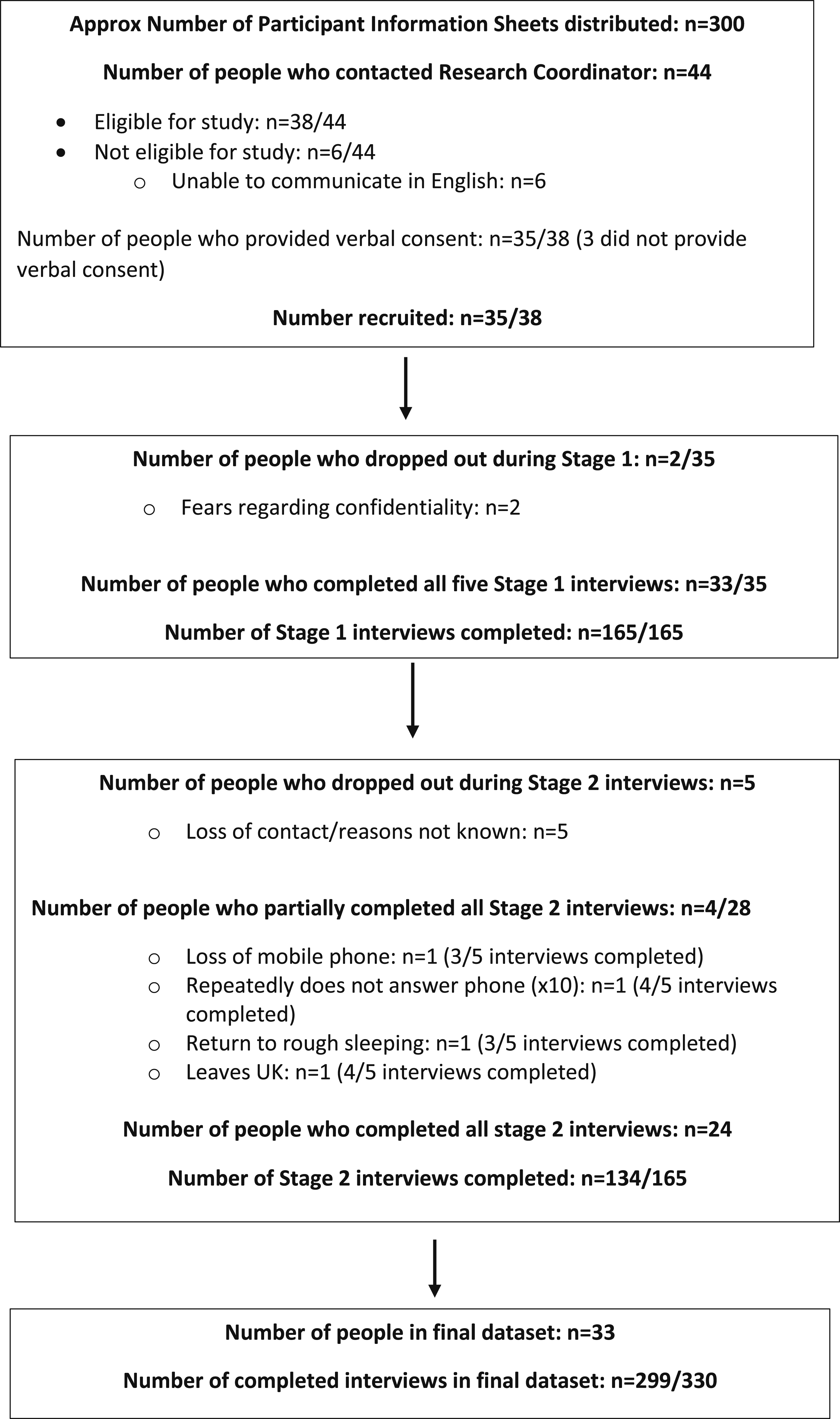
Box 1: Stage 1 Interview Topics (NB: topic guide not included)
Audio-recorded informed consent
In all research, it is required ethical practice to obtain informed consent from research participants. Written informed consent is usually required. Research participants are usually asked to sign an ICF that sets out reciprocal agreements, expectations and conditions associated with the study.
The standard requirements for receiving informed consent were adapted in this rapid qualitative study so that verbal consent was obtained from each resident who participated. Verbal consent is a process that has been approved as ethical in studies that require expedited responses from research participants.22–25 Verbal consent from each participant was obtained during the first telephone call by the research interviewer allocated to each resident. This required the interviewer to read verbatim a series of nine standard consent statements (that would be expected by any Research Ethics Committee) contained within the ICF delivered to the resident’s room. During this conversation, the resident agreed to each statement in order to provide consent for participation. This was audio-recorded on digital equipment (provided by the university) as part of the initial interviewer contact with every resident recruited into the study.
The two-stage, longitudinal, semi-structured interview
Having obtained consent to participate in the study, a two-stage, longitudinal semi-structured interview took place. This was the main method of data generation and involved a series of 10 short telephone-based interviews organised into two stages. Stage 1 comprised five short interviews conducted, where possible, over five consecutive days, designed to be delivered while residents were accommodated in the hotel during lockdown. Stage 1 interviews were semi-structured and focused upon nine interview topics (see Topics A–I in Box 1). Each of the five Stage 1 interviews was designed to take approximately 20–30 min to complete. This required the resident (and interviewer) to commit to approximately 100–150 min to the study whilst they were within the hotel. Regular, short interviews were undertaken rather than one longer interview because it was assumed that participants would appreciate some form of daily social contact whilst unable to leave their hotel rooms, while minimising mental exhaustion and interview overload (resident and interviewer), avoiding boredom with questions (resident) and maintaining interest (resident and interviewer) in the study.
The ‘Everyone In’ initiative was originally designed to be a 12-week programme of statutory intervention and, as such, the emergency accommodation was never intended to be provided on a permanent basis. Thus, the semi-structured interview schedule was designed to capture this impermanence with the inclusion of a 10th interview topic (Topic J). Topic J focused entirely upon events that happened once residents had left the hotel, as part of next-step or move-on arrangements to more stable rehousing, or, to other hotels or other temporary, emergency accommodation. Topic J therefore formed Stage 2 interviews, and were designed to ‘follow-up’ each resident interviewed at Stage 1 as and when they left Hotels A and B.
Stage 2 interviews consisted of a further five short telephone interviews that took place on a weekly basis as part of the longitudinal (follow-up) design of the study. These weekly interviews were purposely designed to capture any change (positive or negative) in each residents’ circumstances following departure from their respective hotels. Stage 2 interviews were designed to be short conversations that were not expected to exceed 20 min. As such, the five follow-up interviews involved a further approximately 100 min of commitment to the research by each resident (and interviewer).
In order to maximise participation in the study, if residents did not answer their telephone the relevant researcher would call a maximum of four times over a period of several days. If the resident did not answer after four calls, and subsequently did not respond to a text message sent from the Research Co-ordinator, they were considered ‘lost’ to the study. All interviews during Stage 1 and Stage 2 were audio-recorded. This typically involved the interviewer enabling the ‘speaker’ function on their telephone and placing digital recording equipment alongside the handset/device (all with prior consent and approval from the resident) 8 .
Residents received a total of £ 90 in shopping vouchers upon completion of Stage 1 (£ 40) and Stage 2 (£ 50) interviews. Residents were able to select their preferred retailer from several high street outlets, and these vouchers were posted using Royal Mail recorded delivery services, requiring a signature upon receipt. All vouchers were sent to the address provided by the resident at the time of completing each stage of the interview.
Data charting and data reduction
A further adaptation was made to the way in which qualitative data were recorded in order to facilitate a rapid framework analysis. In conventional qualitative research, ‘rigorous analysis’ follows the verbatim transcription (of the audio recording of the interview), familiarisation and interpretation (usually assisted by software designed for qualitative data analysis) of a complete dataset. In this study, rapid data analysis 26 was required due to the aim of providing timely and relevant feedback to stakeholders. In order to expedite data analysis, all interviewers were trained in data charting 27 and data reduction.28,29 The data reduction technique involves transferring summaries of respondent answers into a matrix (data charting) that corresponds to the semi-structured interview schedule.
As such, prior to data generation, a spreadsheet was purposely designed to reflect all Stage 1 and 2 topics as a Framework table. This framework contained 10 spreadsheets (one sheet for each of the 10 interview Topics A–J), in which each column (in each spreadsheet) was titled with the key question asked of the resident. Similarly, each row reflected the response of an individual resident throughout the 10 worksheets. Each of the 11 interviewers received (by email) their own unique spreadsheet and were able to employ the data charting and data reduction techniques with their respective resident caseloads as they completed each of the Stage 1 and Stage 2 interviews. The time required for this data reduction task averaged 30 min per interview topic (approximately 300 min in total per resident), which was therefore additional to the time volunteered to the study (see above).
Interviewers were requested to complete these spreadsheets as soon as possible after each resident interview, in order to maximise recall and accuracy. This process was further assisted by playing-back the recording of the interview and, if necessary, charting selected words, expressions or experiences verbatim within the matrix.
The template produced 110 spreadsheets (10 sheets x 11 interviewers) of data that summarised experiences of 35 residents (which reduced to 33 after 2 withdrawals from study). In addition, due to the structured format of the workbook design, all 11 matrices could be merged into a single framework by the Data Manager (DM).
Data merging
Data merging involved the collapse of all 110 spreadsheets from each of the interviewers into a single workbook. At various times during the study, the DM requested all interviewers to send their current (password protected) workbooks to a centralised point via email. At this location (London), the DM merged all the spreadsheets into one document that eventually provided a summary of all data generated during the Stage 1 and Stage 2 interviews from the 35 residents who were interviewed.
This merging process acted as a quality control measure to ensure consistency in the level of detail recorded (by the interviewer team) and enabled a rapid framework analysis (FA) to occur with all data generated from the 10 topics discussed in interview. As noted elsewhere,27,30,31 FA is an approach that provides opportunities to analyse large tracts of data and identify trends, patterns and anomalies in a rapid and expedited manner. For the purpose of this study, rapid FA was used in a deductive manner during primary analysis in order to reflect the range of questions asked during semi-structured interviews. Rapid FA was also utilised as a method for providing evaluative feedback to key organisations involved in the study and to produce initial reports of emerging findings.32,33
Communication within the interviewer team
Due to the dispersed and remote locations of the interviewer team, routine communication was essential in order to facilitate socially distanced fieldwork. To this end, the application of Microsoft Teams and WhatsApp became essential media for maintaining regular contact and providing support within the team before, during and after socially distanced fieldwork.
Microsoft Teams was used mainly as a forum for providing training but also for data sessions 34 involving shared reflection of resident/interviewer experiences. These data sessions also provided debriefing opportunities for the team in which matters relating to the study (data, methods and reflections) were shared and discussed in a reflective and supportive environment.
The creation of a dedicated WhatsApp Group, with its encrypted data/message service, proved useful as a ‘group noticeboard’ of all research related activity. The WhatsApp group consisted of 11 interviewers and 2 investigators and was used on a frequent (almost daily) basis during Stage 1 and Stage 2 interviews. The WhatsApp Group was primarily used as a mode of pushing ‘live’ communication but also facilitated team learning though sharing individual experience (e.g. implementing the interview) and other information across the group. In addition, WhatsApp was particularly useful in circulating requests for interviewer availability during the recruitment of residents; for interviewers to notify the Research Co-ordinator when residents had completed a full set of Stage 1 and Stage 2 interviews and were ready to receive a shopping voucher; for notifying the team of issues arising from individual interviews; for sharing updates on the policy relating to the ‘Everyone In’ initiative; for sharing media reports of the initiative reported in mainstream journalism; for notifying others of potential distress issues; and even for sharing visual data of the hotels (photographs of empty spaces with no people/participants/residents) during the socially distanced information circulation. (n.b. information that could lead to the identification of research participants was never shared via WhatsApp).
Informing qualitative methodology for a post-COVID era
The previous section describes the methods underpinning a qualitative study that was situated within a public health crisis caused by a pandemic (COVID-19). Whilst the methods described are not ‘new’, the ways in which they were deployed to generate data (that prioritised a remote, team-based, telephonic approach) illustrates innovation regarding the conduct of qualitative research. This was largely occasioned by regulations that limited face-to-face interaction between members of the research team and between the interviewers and all research participants. As a result of these adaptations, various methodological learning points have been acquired, especially in terms of the design and delivery of qualitative research that minimises risk of exposure to (and transmission of) COVID-19. These are presented below as virtual recruitment, audio recorded verbal consent, telephone-based interviewing, telephonic rapport and telephone ownership (by participants), data charting and team structure and role allocation.
Virtual recruitment involving people who speak English as a foreign language
Perhaps the greatest surprise to the research team was the number of residents who responded to the PIS who spoke English as a foreign language (EFL) (in fact, only 11/35 were born in the UK). 32 As recruitment developed, it also became apparent that several residents were people seeking refuge and involved in applications for asylum or visa applications to remain in the UK. Indeed, as noted in the first report from this study, 32 the profile of study participants with experience of rough sleeping was different from that typically found in generic studies of rough sleeping and homelessness.
It was also due to an early recognition of varying EFL ability amongst residents responding to the PIS that led to the introduction of an informal assessment of language competency when potential participants contacted the study co-ordinator 9 by telephone. This assessment was considered integral to recruitment in order to ensure that people making contact were not only able to understand interview questions but, perhaps more importantly, to satisfy the Research Co-ordinator that they were able to comprehend written and verbal instructions regarding their provision of verbal consent to participate fully in the study. Subsequently, six residents who made initial contact did not have sufficient EFL proficiency to be eligible to participate in the study. In four of these cases, other people (who could speak English more fluently) made contact on behalf of the relevant residents (who had received the PIS) and offered to be a ‘translator’ for the person concerned. Those offering to be translators were mainly support staff within the hotel although one resident (already recruited into the study) called on behalf of a relative in the same hotel 10 . In two other cases, it was clear that their EFL was ‘survival level’ 35 and they would have struggled answering complex questions about health, homelessness and service engagement.
In each of these six cases, the Research Co-ordinator was required to make difficult decisions regarding eligibility for participation in the study. Whilst recognising each individual had experience of rough sleeping and associated destitution (possibly including government guidance relating to no recourse to public funds and/or barred from employment 11 ), decisions regarding participation had to prioritise an ability to communicate effectively with a researcher during a telephone-based interview about sensitive issues (such as substance use, financial affairs and residency in the UK), and without assistance from a third party. It was therefore imperative that residents were able to recognise that these questions sought to understand their collective experience and their answers would be treated in confidence and not be used as evidence to justify further sanction or validate deportation of individuals. Indeed, suspicions surrounding these latter concerns led to two participants withdrawing from the study despite assurances that the interviewers were not connected (or reported) to the Home Office (so that their interview data/responses would have no impact upon their application for UK residency).
One possible solution to this language-based dilemma would have been to accept and include third party translators, who could have acted as intermediaries during the telephone-based interviews. However, this too would have raised a number of ethical problems relating to confidentiality and location of interview. For example, social distancing regulations aside, all third parties would have become privy to personal and sensitive material disclosed during translation. However, this would potentially breach confidentiality and anonymity, especially if the third parties were independent of the research team. Furthermore, the use of translation services in social research may be challenged on grounds of linguistic accuracy especially in terms of (forward and back) translation. In such circumstances, both the researcher and the respondent would be completely reliant upon the translation skills of a third party (whether ‘professional’ or ‘non-professional’).
Recognition and awareness of these kinds of ethical issue is perhaps more established in some fields of scholarship than in others. In qualitative studies of the experiences of people seeking refuge/asylum and/or those affected by other international displacement, scholars36–40 have highlighted similar ethical concerns. For example, Kalbranian-Melkonian 41 summarises a range of difficulties relating to language, translation and comprehension when studying people with refugee backgrounds, regardless of whether or not they speak the same language as the researcher or translator. Researchers cannot necessarily predict the many ethical issues that may arise when participants are recruited from multi-cultural (and especially multi-linguistic) backgrounds. Indeed, as Birman 42 notes, efforts to include diverse groups in qualitative research, (despite being hugely rewarding), are ‘extremely labour-intensive and time-consuming’ (p.166). Although Birman (ibid) and other authors (see,36,39,40 have described a variety of techniques for assuring inclusivity and addressing multi-cultural informed consent within qualitative studies, their assorted suggestions were made in a pre-COVID-19 era, at a time when face-to-face interviewing could take place.
New or adapted strategies are likely to be required when conducting remote/telephone-based interviews as used in the study reported here. In addition, the current research was unfunded with no resources for translators, and all communication socially distanced thereby prohibiting participants and translators sitting closely together to facilitate understanding. Several members of the research team spoke more than one language. However, none had the skills to conduct complex research interviews in the range of languages (such as Chinese, Czech, Polish and Romanian) spoken by the study participants.
Audio-recorded verbal consent
One difficulty noted by all of the interviewer team was the method of obtaining audio-recorded verbal consent from residents. This process required the interviewer to read verbatim a series of nine standard consent statements (from the ICF) to the resident (who listened to the statements as they simultaneously read/held the ICF in their hotel room). After each statement, the resident was required to give a positive response in order to provide consent (a negative response meant consent was not given and thus the conversation was designed to end immediately).
However, difficulties arose in this process due to the complex, technical language, contained within statements preferred by Research Ethics Committees, that had to be read out by the interviewer and to which the resident preferably provides a positive response (i.e. consent). This process was not only time consuming for both interviewer and resident but was particularly problematic for those whose spoke EFL. For example, one standard ICF statement reads: ‘I understand that such information will be handled in accordance with the terms of the UK General Data Protection Regulation (GDPR)’. In at least one interview this statement resulted in a lengthy explanation (lasting approximately 15 min) and discussion of what GDPR law involves and that it has no consequence to those making visa applications for UK residency. Similarly, in another interview, the British resident (UK citizen, English speaking) simply disconnected from the conversation (turned off their phone/hung up the telephone) during the verbatim reading of the nine statements. In this instance, the resident concerned became ‘lost’ to the study due to disengagement.
These experiences of obtaining informed consent via telephone perhaps reflect existing challenges in more ‘traditional’, face-to-face, qualitative research interviews. This is due to the long-standing, well established issues of ‘participant comprehension’ and ‘researcher intuition’ during the informed consent process and whether or not a researcher is sufficiently skilled to physically observe and intuit (from previous experience) whether or not a participant has understood the terms and conditions of a research interview. During remote, detached interviews (as with those done by audio via telephones and without any visual/video accompaniment), participant comprehension of a research project (and its aims and expectations) is premised less upon researcher observation and intuition, and more upon the questions asked (or not asked) by the participant, and responses provided (or not provided) to the informed consent statements by each individual participant. In short, this study perhaps demonstrates that in order to enhance the process of informed consent during a telephone-based qualitative study, all text-based materials associated with the research (such as information sheets and consent forms) should be written (and verbalised when appropriate) in ‘plain English’. This style of informal communication would aim to avoid complex, technical language (see Ref.[42] in order to assist comprehension of the relevant study – especially if the target population may include people who speak English as foreign language.
Telephone-based Interviews, Telephonic Rapport and Telephone Ownership by Research Participants
The strengths, limitations and opportunities of telephone-based interviewing as a research method are well established.43–46 However, this study used an innovative design of short, multiple, and frequent telephone-based interviews. The strengths and weaknesses of these are discussed below based on the views and experiences of the individual interviewers responsible for data generation in this study.
Strengths of this design related to the ability to contact residents as the telephone calls in Stage 1 were conducted when residents were ‘in the hotel’. At this Stage of the study, residents were typically in their rooms at a pre-arranged interview time/date when the interviewer called possibly as a result of the social distancing measures in place during the national lockdown.
Stage 2 interviews took place when there were fewer COVID-19 social restrictions and when participants had moved to residential settings that ranged from private flats, hostels, hotel rooms and ‘bed and breakfast’ accommodation. These conditions made telephone contact more difficult to maintain (even with the application of four calls to ensure participation; see above), compared to when residents were hotel-based. This was often due to residents’ involvement in other activities (appointments with services, shopping, exercising in public parks, street-drinking) or they simply did not answer the call (or subsequent texts) for reasons unknown. In short, whereas the five Stage 1 interviews (per resident) were completed relatively quickly over 5–7 consecutive days, the five, weekly, Stage 2 interviews often extended over the anticipated 5 weeks to complete. Location of the resident when receiving the telephone call was therefore a strength (the hotel room) and a limitation (when in community settings) regarding the conduct and completion of telephone interviews. 12 Indeed, the relatively low attrition rate (in which contact was completely lost with only five residents when they relocated to community settings) during Stage 2 interviews perhaps reflects the overall strengths of this approach to telephone-based interviewing.
A further strength of telephone-based interviewing was the volume of data that was generated across all Stage 1 and Stage 2 interviews. As each of the interviews (five within each stage) were designed to be short and topic focused, it was possible for the interviewers to obtain rich descriptions of residents’ experiences of rough sleeping, and of the ‘Everybody In’ initiative. However, some residents also preferred to complete multiple topics during Stage 1 interviews so that they could be completed in less than 5 days (a few residents even completed all five Stage 1 interviews in an extended period lasting more than 2 h). As such, telephone-based interviewing was found to be a method that offered flexibility (for the residents and interviewers alike), so that Stage 1 interviews could be completed in periods ranging from a few hours to several days. Stage 2 interviews premised a single issue (‘experiences after the hotel’) and these interviews also reflected upon the various topics covered in Stage 1 and any (positive or negative) change that had occurred to individual circumstances. As such, these interviews offered similar flexibility in terms of time commitment. For example, if a resident did not complete a Stage 2 interview for 1 week, the same questions could be adapted the following week so that they included any relevant experiences from the ‘missing’ time period.
Telephone-based interviewing conducted over an extended period of time (across the two stages) also assisted in building rapport between some of the researchers and the residents they interviewed (especially those participants who were fluent in English). Contrary to concerns that telephone interviews do not assist with building rapport between interviewer-participant, the longitudinal design of this study led to many residents reporting they enjoyed the experience of speaking on a regular basis to their allocated interviewer.
Interviewer accounts of rapport were shared in group meetings, or directly with the Research Co-ordinator, in which residents had stated/texted they ‘looked forward’ to speaking to the interviewer, that the interview had been ‘therapeutic’ as problems were shared with another or that the ‘little chats’ had been ‘good’ for an individual’s mental health. In addition, several residents also volunteered additional material to their relevant interviewer that provided further insights into their lives before, during and after lockdown. These materials included artwork, poems, videos, photographs and text messages/voicemails and generated supplementary (and unexpected) data. Residents donating these items were asked if the material they provided could be used as ‘artefacts’ obtained from socially distanced fieldwork – to which all agreed. From a resident-interviewer perspective however, the voluntary provision of such artefacts suggests that rapport had been successfully achieved and that those donating such material clearly trusted the interviewer in whom they confided by sharing such personal material.
In addition, the interviewer team consisted of female (n = 6) and male (n = 5) researchers who collectively volunteered to interview a cohort of 6 female and 29 male participants. Allocation of participants to interviewer was based on the availability (and associated work-related/personal capacity) of the latter and not on the basis of any shared characteristics between researcher and participant (such as gender or sex). This method of allocation did not appear to establish any significant barrier or obstacle in establishing and maintaining rapport with participants during data generation (as none of the research team reported this as an issue and none of the participants verbally objected to speaking to a particular researcher).
Conversely, group discussions within the research team also identified several common difficulties associated with the process of conducting telephone-based interviewing. One such difficulty was the way in which the telephonic interview prevented important visual cues (such as body posture, facial expressions, hesitation during speech and other non-verbal communication) from being noted in situ by the interviewer. In conventional qualitative interviews, these forms of non-verbal communication often provide opportunities to develop new questions or follow unexpected lines of inquiry. 47
A further limitation noted throughout by the interviewer team relates to the quality of the audio-connection between devices used in the telephone-based interview. Clearly, a good connection resulted in an audible conversation that could be digitally recorded with ease. However, on occasions during both stages of the longitudinal interview (i.e. in the hotel and after the hotel) some residents were inaudible and difficult to hear. In most cases this was due to connectivity, in others it was due to the accent/dialect of the resident – and on at least one occasion it was due to both. In the most extreme example of this situation, the relevant interviewer had to stop the interview in order to avoid providing inappropriate interviewer responses to the resident’s dialogue that may have concerned a sensitive topic. In another situation, one of the team reported that ‘there are only so many times the interviewer can ask (residents) to repeat what they are saying or seek clarification without it seeming rude (as) this can damage the rapport’. As such, the telephone-based interview created ‘audio’ limitations that could be better resolved when occurring in more conventional, face-to-face, meetings. However, whilst these sound-related limitations are well established within the literature, in this study, the interviewer team had the advantage of being able to return to a topic (for example, if not fully understood as a result of poor sound quality) due to the longitudinal design of the interview schedule.
The value and importance of mobile telephone ownership by the residents interviewed in this study cannot be overstated. Perhaps more significantly, the distribution of mobile telephones by various service providers to residents as and when they arrived at the hotel (during March 2020) undoubtedly assisted this study and contributed to the successful completion of the two-stage longitudinal interview with 28 of the 33 residents (see Diagram 1).
To reiterate, ownership of these devices by residents contributed towards the completion of 299 of a possible 330 interviews. In addition, the provision of free hotel Wi-Fi and free credit on these devices (paid for by services) also ensured that residents could contact the Research Co-ordinator during the recruitment phases of the study. Although these mobile phones were provided as part of the ‘Everyone In’ initiative in London (so that caseworkers, services and organisations managing the hotels could contact residents in a socially distant manner), from a research perspective they were instrumental in facilitating the successful progress of the interviews while residents were in the hotel and after they had left. For almost all of those interviewed, the ownership of the hotel-issued phone continued until all Stage 2 interviews were completed. While the automatic provision of free credit typically ceased upon departure from the hotel, several residents commented during interview that their mobile phone provided a ‘lifeline’ for continued contact with services and people, when they had moved-on to other accommodation. Indeed, without these phones it is unlikely that this study would have generated high volumes of data and ‘successful’ follow-up during the longitudinal interview design.
Data charting
Data charting in this study involved the rapid transfer of summary data to a framework template (spreadsheet) by each of the 11 interviewers. Data charting typically took place immediately after each interview and, when collated and merged across the team, produced an extensive dataset that summarised 299 interviews conducted with 33 residents.
This method of collective data reduction and collective data charting produced immediate results that could be shared (in password protected formats) throughout the team and with the DM. Indeed, it was this method of data management that facilitated the rapid production of the initial formal report 32 that documented ‘life in the hotel’ (based upon Stage 1 interviews). The relevant findings were subsequently consolidated in a second report 32 that summarised ‘life after the hotel’ (based upon Stage 2 follow-up interviews). These documents were published in November 2020 and January 2021 respectively and provided timely, relevant and rapid feedback of key findings to the organisers of the ‘Everyone In’ initiative (including GLA and charitable organisations managing Hotel A and Hotel B).
Similarly, as a method, the team of interviewers did not appear to find data charting an arduous task. Feedback (verbal and written) to the Research Co-ordinator noted that the task of transferring audio data to written text was relatively ‘quick’ and ‘easy’, in which the framework was well designed to ‘accurately reflect’ the topics and associated questions. Others reported that the framework was easy to chart with data due to completing the task so soon after the interview when details were still ‘fresh in the mind’ and could be ‘easily remembered’. Indeed, the only criticism of the method was that (for those who had larger caseloads at least) the task could be ‘time-consuming’ especially when completed immediately after several (back-to-back) interviews.
From a methodological perspective, members of the interview team also recognised several limitations of the data charting and data reduction. For example, some team members expressed concern that the data charted may have been based upon the interviewers’ interpretation of the residents’ experiences (and thus data summaries were interpretations informed by particular biases). Others reported that data charting did not provide enough space to provide more ‘nuanced’ and ‘contextualised’ summaries of residents’ experience, and that these aspects of circumstances could be overlooked during rapid framework analysis. Indeed, these collective reflections confirmed that transcriptions of interviews would need to take place at a time when data generation was complete (as with conventional qualitative research). The production of verbatim transcripts would then facilitate more rigorous analyses in order to provide thicker descriptions of ‘life in/after the hotel’ by those concerned. This was especially agreed with regard to the production of potential manuscripts submitted to academic journals for peer review, in order to avoid criticisms relating to rapid analysis. 29
Team structure and role allocation
The assorted roles and responsibilities allocated within the team reflected existing experience/expertise and were implemented in order to enable/facilitate maximum participation by wider team members during a limited period of time/availability. For these reasons (enablement, facilitation and participation), several individuals were responsible for making decisions, overseeing and guiding research practice for the interviewers and holding conversations of a strategic nature with people outside of the research setting. These co-ordinating roles provided direction and guidance as part of a dialectical relationship between the full team, the external partners and the team of interviewers. From this organisational and operational structure, not only was knowledge of the ‘Everybody In’ initiative fully shared by those involved, but the process of conducting qualitative research amidst a pandemic enabled methodological innovation and solution-focused discussions (to address emergent problems and difficulties encountered during data generation).
Finally, facilitation of all research activity across the team by the various co-ordinators appears to have promoted participation throughout the team through the development of a community of practice situated mainly in the virtual world. 48 For example, the interviewer team were frequently invited to attend online meetings and to provide (verbal and written) summaries of their experiences (regarding the implementation of methods), to share the findings from their interviews and to comment upon output produced throughout the study (such as the two formal reports and this article). Not only did this facilitation seek to ensure participation, but made it visible while situated in remote, distributed settings. This, in turn, enabled best practice to emerge through collective feedback in which team members learnt how to improve the research via remote interaction.
Conclusion
This study demonstrates that the COVID-19 pandemic and the associated public health measures to control its spread did not prohibit the design or conduct of qualitative research with people experiencing rough sleeping in London. Where barriers to the study existed, these related more to the conditions and circumstances surrounding homelessness, fluency (or not) in English language ability, and the community settings to which residents returned after their stay in the hotels. As such, these barriers were largely a function of structural and personal constraints that impacted upon some individuals’ capacity to fully participate in the study.
From an operational perspective, the various methodological adaptations described in this article show how qualitative research can still be delivered in conditions that control and limit social contact. In so doing, this study provides insights regarding the design and conduct of socially distanced qualitative research. Given that social research will likely be affected by social distancing measures, with an increased emphasis upon technology and computer-assisted communication, for some time yet, the methods described herein should provide some guidance regarding the strengths and limitations of conducting future socially distanced qualitative research amongst people who are homeless and/or with experience of rough sleeping. Relatedly, this research has shown how it is possible to engage people who are homeless in longitudinal telephone interviews and has found that they are motivated to contribute to qualitative research about their experiences – if they have the relevant resources that facilitate participation. In this regard, a key resource is the ownership of a mobile telephone.
A further implication from the study relates to telephone ownership. In short, researchers should not assume that people who are homeless have guaranteed access to mobile devices – particularly if they are to be involved in longitudinal telephone interviews. People with experience of rough sleeping/homelessness may not have continuous access to mobile devices (or be able to afford the credit to pay for their operation) as frequently as those in more secure and stable accommodation. In this study, the provision of free mobile phones (and credit) greatly facilitated the completion of 299 topic-based interviews. Whether or not this number would have been achieved without such provision is open to conjecture. However, as mobile technology advances, coupled with an increased application in health and social research, it is important that researchers do not assume telephone ownership in vulnerable populations is universal or stable. Such an assumption may inadvertently perpetuate inequity (and exclusion from research) with researchers misreading non-participation as ‘informed choice’ rather than lack of resources. One suggestion here may be that researchers consider the inclusion of the purchase and distribution of mobile phones (including running costs) as part of applications for research funding (especially if that involves participant engagement with longitudinal qualitative studies that require secure telephone ownership).
This issue of secure (and insecure) telephone ownership is made more noteworthy given that all Stage 1 interviews (n=165) in this study were successfully completed during a period in which all residents were housed in stable (albeit temporary) accommodation. In contrast, when residents moved-on to other potentially less secure accommodation within the community, contact was lost with several individuals (n=5) and some of the Stage 2 interviews were only partially completed with other residents (n=3) [see Diagram 1]. Although the authors are unable to provide the exact reasons for these missing data, it is possible that this was a consequence of leaving the hotel and returning to ‘pre-lockdown’ lifestyles in which movement and social contact was less restrictive. For example, one individual with whom contact was ‘lost’ during Stage 2 interviewing was known to be living in a tent in a public park after moving-on from the hotel (and therefore had no access to electricity to charge the mobile phone). Similarly, another person appeared to have mislaid their phone as, at the time of a scheduled interview, it was answered by persons unknown who claimed to have ‘found’ the device at an Accident and Emergency Department within a London hospital. In short, these examples (of missing data) indicate barriers to research participation that are more associated with the wider experiences of homelessness than the restrictions imposed by COVID-19.
With specific regard to the conduct of socially distanced recruitment for telephone-based interviews, there is also a need for researchers to consider the way in which ICF are worded, presented and verbalised in attempts to obtain informed verbal consent. In this study, the process was found to be problematic and time consuming for both interviewers and participants, regardless of the latter’s English language competency. For example, the nine statements of consent used in this study were lengthy, complex sentences that required an advanced knowledge of English language in order to provide a response (positive or negative). A recommendation here is for researchers to work in conjunction with Research Ethics Committees to produce statements of consent that are succinct and comprehensible to research participants (who speak English fluently or as a foreign language) and especially for the purposes of conducting research recruitment by telephone. This simplification process would aim to increase participation, foster greater inclusion, reduce suspicion, fear and/or disengagement and further enable ‘hidden’ populations (concealed by less advanced levels of English language ability) to participate in qualitative studies of issues that equally affect the lives of those who speak English as a foreign language. Indeed, as Birman 42 notes, diversity in research is an ethical issue, in which a failure to include marginal voices risks under-representation in policy-related decisions. Furthermore, as others have commented,37,39,49,50 ethical frameworks are typically concerned with avoiding harm to research participants, and/or protecting the researcher/research institution, whilst simultaneously overlooking an obligation ‘to design and conduct research projects that aim to bring about reciprocal benefits’ (p.299) 50 for diverse populations and communities.
This article presents an account of how current and future social research may be managed in order to meet the aims and objectives of a programme of study. Not only has COVID-19 possibly changed forever the way in which qualitative research methods are delivered in the field (and how the ‘field’ is defined), but also the way in which researchers work together on a given topic, in remote and distributed settings. In this regard, the authors describe a core-team of individuals located throughout England (and beyond) who were responsible for the generation and analyses of qualitative data. Whilst this format of teamwork may be common in quantitative studies (such as randomised controlled trials or large cohort studies or surveys) where roles and responsibilities are routinely delineated by knowledge, expertise and seniority, such an approach is unusual in qualitative studies which typically involve individual researchers or smaller teams consisting of 2–3 researchers who all have intimate knowledge of the participants and data. Arguably, a change in approach to qualitative research, in which team members adopt particular roles that serve to co-ordinate, organise and enable larger teams of qualitative researchers, may become advantageous or even necessary in the adaptation of qualitative research methods in a post-COVID-19 era.
Finally, this study provides insights into new ways of engaging with similar marginalised populations (equally hard to reach or hard to engage) at a time when COVID-19 may be less of a public health risk. For example, the study illustrates the versality and utility of mobile technology, conducting fieldwork remotely and the way in which telephone-based interviews can be arranged on a flexible basis (rather than completed in a single session). The longitudinal design of the telephone-based interview further demonstrates how rapport and inclusion can be fostered and sustained over an extended period of time between researchers and research participants. Less positively, the study highlights the potential for ‘technological exclusion’ to occur, in which assumptions of telephone ownership may fail to include those affected by a given research topic. Relatedly, over reliance upon mobile technology for interviewing may create difficulties in terms of implementing ‘distress protocols’ if research participants become overwhelmed by questions considered ‘too sensitive’. As such, telephone-based interviewing may not be suited to addressing overtly sensitive topics (regardless of whether before, during or after a public health crisis) and some methodological innovation may be needed to ensure the well-being of research participants affected by trauma or distress during remote interviews.
Footnotes
Acknowledgements
The authors would like to thank all of the ‘hotel residents’ (research participants) who took part in this study, and for giving their time to complete the 10 interviews involved in the two stages of interviewing. The authors also thank the various charities and associated staff for providing assistance and access to the two hotels throughout Stage 1 of the study. The authors also acknowledge Dr Emily Finch (South London and Maudsley NHS Trust), and Professor Gail Gilchrist and Professor Colin Drummond (both National Addiction Centre, King’s College London) for their support and assistance. Finally, the authors thank the two anonymous peer reviewers for offering constructive and helpful comments to an earlier draft of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.