
Abstract
Mixed methods have emerged as potential problem solvers particularly where traditional mono-method approaches fail to deal with specific research problems. The integration of quantitative and qualitative data within mixed methods approaches is central and should be carefully planned and executed. It is equally important to choose an appropriate mixed methods design, that promises to answer the research questions posed at the start of the research endeavour. The authors used an exploratory sequential mixed method approach to explore stroke knowledge and educational needs in a large population. They present the development and use of a framework (matrix) to ensure comprehensive and transparent data integration in their study and may be used as a template for future studies.
Background
Mixed methods are nowadays well established and are considered as a separate third entity from their basic components, namely quantitative and qualitative methods.1 This development followed multiple efforts by various authors who also tried to establish guidelines for conducting such research. John W. Creswell is regarded as a pioneer of mixed methods and described how one should not view quantitative and qualitative worldviews as antagonizing but rather view different paradigms as standing on a spectrum, in which mixed methods occupy the third chair.2 Creswell emphasizes the need to follow pragmatically the rules of both quantitative and qualitative research when conducting mixed methods research but also to ensure adequate mixing of the two traditional paradigms.3
Aim
Perhaps, the most difficult aspect of mixed methods research is the integration of qualitative and quantitative data as failure to do so will result in multiple methods instead. In this article, the authors present the development and use of a ‘matrix’ in an exploratory sequential mixed methods study regarding stroke knowledge. The ‘matrix’ assumed a 3-column table format, which aided the development of a new tool (questionnaire) to assess stroke knowledge and response. The table comprised data gathered from an initial exploratory qualitative phase as well as relevant data that emerged from a systematic literature review on the topic. This ensured a comprehensive and transparent way of merging the quantitative and qualitative phases of the study undertaken.
Statement of the problem underlying the current study
Stroke remains a leading cause of morbidity and mortality worldwide. Recent medical advances in the treatment of stroke have been the key to changing a preventable catastrophe to a potentially treatable disease. However, treatment is restricted to a time-window, which has led to the aphorism “Time is Brain”. Prompt presentation to emergency services has been extensively linked to patients’ knowledge about their symptomatology and recommended actions in stroke, which is subsequently influenced by more complex psychological ‘barriers’. The aim of this study was to explore and quantify stroke knowledge in Malta and to identify any potential educational lacunae in this respect. The data generated could in turn be used to adapt local practices and improve patients’ long-term outcomes. This required an in-depth investigation of the stroke experience as recalled by affected patients, followed by the development of a quantitative tool which was later used to generalize the findings. For these purposes, a mixed methods approach was utilized.
Study setting
This study was performed in Malta, which forms part of the European Union. Surprisingly, a local audit showed that only 1.59% of acute stroke patients who presented to hospital were eligible for (and received) Tissue Plasminogen Activator (t-PA) treatment.4 Although this finding may partly be attributed to the numerous contra-indications for intravenous t-PA, late arrival to hospital was the most common reason why this treatment could not be administered. Considering the Maltese geographical boundaries and the fact that the main acute hospital is centrally located on the island, one can hardly blame this late arrival on geographical factors. In fact,5 previously claimed that “one clear advantage resulting from small geographical size is easier access to the health care system”. Both pre- and in- hospital delays are at least partly attributable to lack of stroke knowledge. Although other social and cultural barriers exist and may act as potential barriers to an adequate stroke response, lack of knowledge on how to recognize the symptomatology of stroke and engage in the necessary action appear to be the main factors causing delayed presentation to health services. This knowledge deficit seems to be a global issue, as previously reported by numerous authors.6,7 A quick glance at the literature highlights the deficit of local studies investigating stroke knowledge, which has therefore led to an inability to determine and possibly tackle the causative factors for late presentation in stroke. It was thus considered that there was a desperate need to study this aspect of stroke and to highlight the major educational needs in Malta. The continuously changing guidelines in acute stroke treatment also mean that healthcare workers and medical doctors require continuous stroke education to ensure effective and timely treatment.
Research questions
In order to address the aim of the study, the following research questions guided the process:
What are the reflections of stroke sufferers on the way that they managed their stroke onset?
How much knowledge does the Maltese population have with regards to stroke recognition and management?
What findings emerge from comparing and merging data from the reflections of stroke sufferers to quantitative instrument data on the Maltese population’s knowledge?
Which educational lacunae are present in relation to the Maltese population’s knowledge about stroke recognition and management?
The first and second questions were tackled though qualitative and quantitative methods respectively, whilst the last two research questions necessitated mixed methods. Upon reflection on the research questions set out at the initial phase of this study, it emerged that neither qualitative nor quantitative methods would likely be adequate as a standalone approach in providing the answers required. Subsequently, the design of this study steered away from a monomethod investigation and towards an eclectic paradigm instead.
Overview of method used
After exploring several mixed-method approaches, the
Mixed methods approaches
The introduction of a research method that diverges from a monomethod approach has prompted many researchers to put forth different enquiry strategies and their respective elaborate procedures as well as mixed methods research nomenclature and classification. One prominent mixed methods typology was that presented by Caracelli and Greene.8 This included two broad categories, namely, a component design and an integrated design, which, in combination, have a total of seven sub-categories.
A more recent interpretation and adaptation of these different designs that features in the literature presents the distinction between basic and advanced approaches.3 The types of basic approaches are convergent design and a sequential strategy. The advanced designs consist of the intervention approach, social justice design, and multistage evaluation design. A sequential mixed methods strategy may be of the explanatory type, which involves an initial quantitative part to test a theory or concept followed by a qualitative aspect to facilitate further deeper exploration. Alternatively, a sequential exploratory mixed methods approach necessitates commencing with qualitative data collection for an exploratory intent followed by a quantitative stage so as to allow for generalizability.3
Choice of a specific mixed methods design
Following their experiences of using different types of mixed method designs, Cronholm and Hjalmarsson9 advocate for the use of an exploratory approach in situations where the topic of interest is complex, relatively unknown, or understudied or when one needs guidance to ask the right question. Creswell and Plano Clark1 add that this type of research is also useful when data collection instruments or measures do not exist and when the variables are not known. Since this was considered to be the status quo of the current study and the situation regarding stroke knowledge in Malta, a sequential exploratory design was therefore deemed as being more likely to act as an effective guide to the research process and to yield rich results. Utilizing this framework offered the opportunity to test the qualitative categories in the quantitative part. Moreover, it is a design which is known to be easy to implement, despite being time-consuming. Conversely, unless the initial qualitative stage provides findings which can be easily translated into a quantitative measure, proceeding into the second stage may pose difficulties.1
The data collection strategy in the mixed methods paradigm that formed the framework of this study involved both constructivism and objectivity, as is commonly practiced in the mix of epistemologies that characterize such an approach. Constructivism was applied during the qualitative phase, which involved a direct meeting and discussion with the informants. During this phase, meanings associated with interactions between experiences and ideas were explored – this is congruent with Piaget’s constructivist views.10 Objectivity was more visibly employed during the second stage of the study with a focus on quantitative data collection. The issue of researcher objectivity may be questionable since it is somewhat impossible to approach a research study with a ‘tabula rasa’ due to the tendency for human nature to have an opinion about even relatively unknown situations.11 In the case of this study, objectivity was an even greater challenge since the authors’ field of work is closely related to the topic under study and so their experiences and opinions may have introduced an element of bias in all phases of the research process, especially in the interpretation of results. However, the risk of bias was limited by cross-checking actions and interpretations with other researchers during the journey. Although this process was carried out throughout the study, it was increasingly necessary during the qualitative part since quantitative data collection and interpretation tends to be more objective whereas in qualitative research, the researcher may be more personally immersed in the process. On a more positive note, it should be acknowledged that this potential limitation proved to be a strength since the authors’ experience and previous knowledge of stroke facilitated the understanding of attitudes in the local scenario.
Research design
Although the research process followed in this study was based on an exploratory sequential mixed methods design, it should be noted that since the introduction of the mixed methods paradigm, many academics have put forward their understanding and presentation of different designs that fall under this kind of research. In this regard, an overview of the available literature shows that consensus is not always reached and while this leads to healthy critical discussions, it also highlights the need for a researcher to select one particular approach and use it as guidance. Thus, in this study, the exploratory sequential mixed methods design was that proposed by Creswell and Plano Clark1 because of the clear explanation provided and apparent effectiveness and simplicity to implement.
As an overview, this framework involves three stages. The first stage is the qualitative phase, during which the problem is explored in depth and subsequently analyzed. This leads to the second stage, which involves an examination of the qualitative analysis in order to use the information to construct an instrument or measure to be used for quantitative data collection. In this stage, conversion from the qualitative aspect to a quantitative one may be challenging since it involves the conversion of themes into scales, codes into variables, and quotes into items. While this process invariably has an element of complexity, existing sources for instrument construction, such as the guidance provided by Creswell,3 may be of assistance. The main strength in this process is that the quantitative tool that results is based on the informants’ experiences, thus enhancing the pragmatic aspect of the study. The final and third stage is the application of the tool to a large sample – this can subsequently provide insight into the generalizability of the initial qualitative findings. While the exploratory sequential design is the most complex and time consuming of the basic designs, its rigor characterizes it with a sophistication that the other methods do not exhibit.3
Current study stages and data integration
As depicted in Figure 1, three research stages were adopted during the study, each of which aimed to use a different source, method, and data collection tool to attempt the collection of data that is both comprehensive and holistic. As described by Creswell,3 one of the most important aspect of mixed methods research is the integration of data. While this process simply refers to the mixing of quantitative and qualitative data that should occur within such research, it should be acknowledged that the process merits particular attention since it is what actually characterizes the mixed methods paradigm. Consequently, Creswell3 identified four types of data integration according to the type of research design being followed. For application to the current exploratory sequential design, the main integration type that featured was ‘building of the data’ which is actuated by using qualitative data in one phase to build the quantitative part, such as the construction of a new tool as seen in this study.
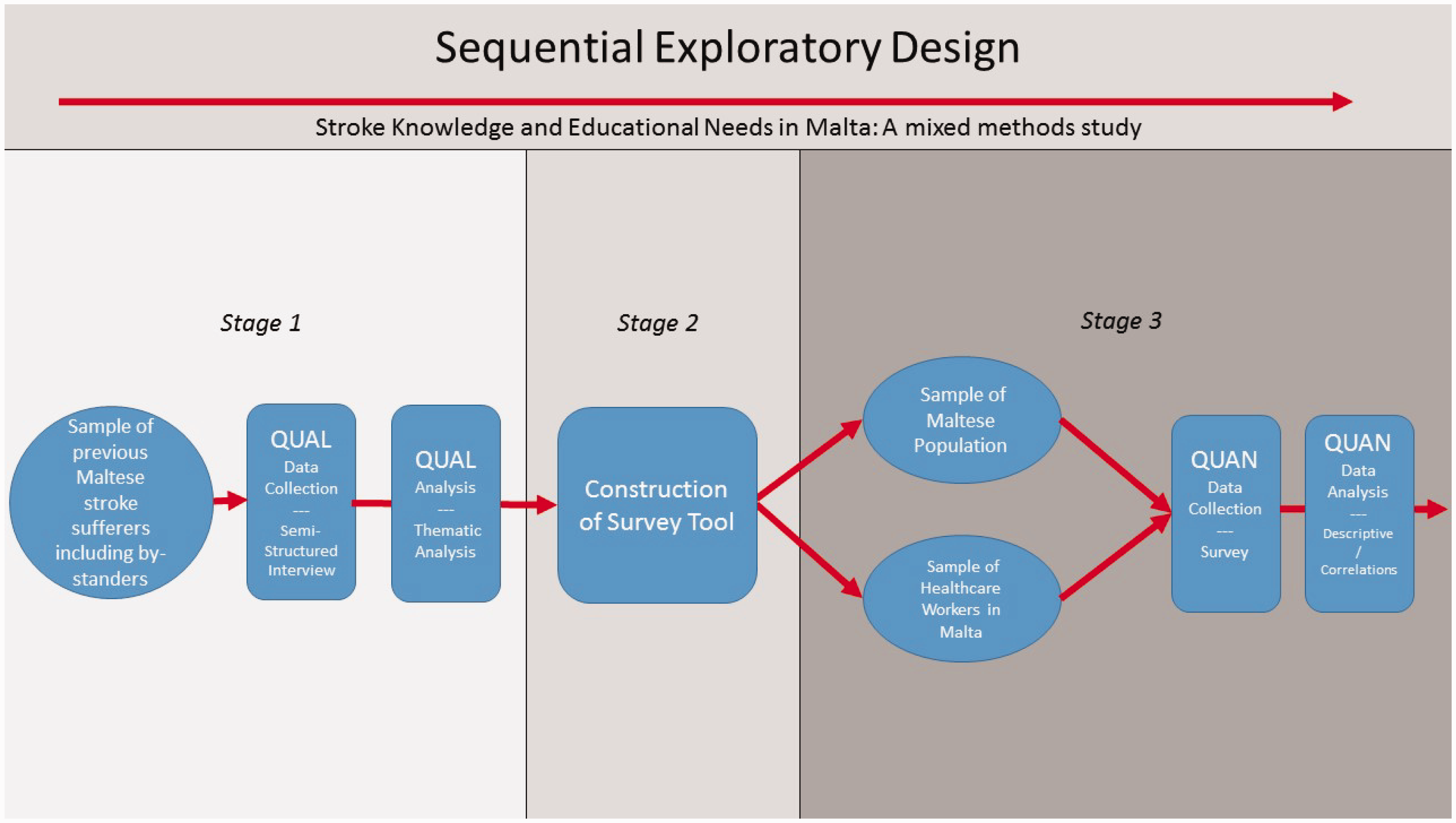
Study design.
Thus, in this case, quantitative and qualitative data were connected (mixed) at the analysis phase using a matrix system to construct the tool in phase 2 (of the study) and at the interpretation phase through a discussion.
Stage 1 of the study
The first part of the study comprised qualitative data collection. The main purpose of this phase was to gain insight into the reflections of stroke sufferers and bystanders on the way that they managed the onset of stroke. Areas explored included attitudes and perceived knowledge about stroke prior to and after onset, the events leading up to stroke onset, and the immediate aftermath, as well as a critical evaluation of the way that the participants managed the onset. The findings generated informed the development of the data collection tool in the second phase of the study.
In view of the purpose of Stage 1, it was concluded that a semi-structured interview should be used to collect data from individuals who had suffered from a stroke during the previous 2 years as well as from any bystanders who accompanied the patient. The rationale behind this data collection method lies in the knowledge that the area under study has not been researched and so this merits a detailed and comprehensive inquiry which can be afforded by one-to-one interviews.12 The fact that a semi-structured format was used (as opposed to a structured one) transcends other methods in that the researcher has a degree of flexibility and can adapt the direction of data collection based on emerging data during the discussion with the participant. Additionally, answers can be probed and clarifications or elaborations can be demanded instantly.2 Perhaps the major drawback of using this data collection method is the time consumption that characterizes one-to-one interviews and their transcription and analysis.13 The semi-structured interview schedule was based on the research questions guiding the study and on prominent themes emerging from literature on the topic. Before commencement of the actual study, two pilot interviews were carried out in order to evaluate the feasibility and overall clarity of the interview guide and process as well as to practice interviewing techniques.
The reason for selecting stroke sufferers as the participant group in Stage 1 emerged from the realization that these individuals are likely in a very strong position to provide rich data since they have first-hand experience of stroke and its consequences. Thus, capturing the voice of this group can add to the pragmatic and humanistic dimensions of the study.
Similarly, the rationale for including bystanders emerged from the pilot study since it was realized that they frequently prompted or reminded the stroke sufferer of certain details during the interview and so represented good sources of information as well as serving as a support for the patient.
Creswell’s input to determining the sample size for the qualitative part of a study revolves around the recommendation to opt for a small sample. 2 This advice is based on the idea that qualitative focus is concerned with the generation of an in-depth understanding of an area and so the emphasis is on an exploration of heterogeneities (or homogeneities) in meaning. Commonly, this involves an inductive and emergent process based on the how and why, processes, situations or social interactions. In this view, a small sample size is adequate since the aim is not to generalize or to test a hypothesis.
In light of these reflections, it was decided to recruit eight to ten stroke sufferers and their bystanders (if any) for the first stage of this research study.
Sampling was carried out using a purposeful random sampling technique. This is a technique that draws upon the strengths of purposive sampling and random sampling while avoiding the lack of rigor and credibility that is associated with convenience sampling.14 First, patients who had been admitted to a state hospital due to a stroke during the previous 2 years (to allow for accurate memory recall) but not earlier than 3 months prior to data collection (to allow for recovery following the acute period) were identified. A list of potential participants was compiled by liaising with multidisciplinary healthcare team members to assess whether the participants satisfied the inclusion and exclusion criteria. Random selection of twelve participants (two for the pilot phase and ten for the actual study) from the latter list was then performed.
The first step of data analysis was the creation of documents from each interview, including transcripts of the interview as well as the notes and the recordings of the personal reactions to the interviews. The qualitative analysis software ATLAS.TI (Scientific Software Development GmbH) was used to facilitate data management and presentation. Yin’s models of data analysis were used as guidance.15
A preliminary analysis was initially conducted during which the documents were thoroughly reviewed and initial codes were extracted, as guided by Braun and Clarke.16 During this process, the research questions were not given prominence, and the focus was instead on the respondents’ perspective. Thus, an inductive coding technique was applied. The second step was to form themes for each case.
The themes were subsequently compared across the cases so that similarities and differences could be analyzed and interpreted. This process followed Yin’s analytic technique of cross synthesis. These similarities were then interpreted and contrasts performed. Interpretation involved both ‘direct interpretation’, which involved the process of deriving meaning from a single incident, as well as the developing of naturalistic generalizations, which consisted of the application of the findings from one case to the other cases2 (p. 245). This necessitated a review of each case to establish its uniqueness as well as its similarities to the other cases. Another coder was involved in this process to enhance the validity of the themes. Any discrepancies were explored, and amendments carried out accordingly.
Stage 2—Development of a framework for data interchange—The ‘matrix’
The content of the tool was predominantly guided by the qualitative Stage 1 data. The other source for tool construction was the information that emerged from a thematic synthesis of literature on the topic, which shall be described in detail further on.
In order to facilitate and portray the conversion of qualitative data (Stage 1 + literature review) to quantitative (Stage 3) survey questions, a framework was constructed. This type of system ensures that all important qualitative themes are addressed in the quantitative stage, a necessary process because neglecting to address the comprehensive interchange of data between the stages is often a major pitfall of the mixed methods approach. Adequate mixing of the data is what renders a study truly mixed methods in design, since otherwise it would simply be a case of using multiple methods within the same research process. Moreover, the development and use of such a framework was also aimed at enhancing transparency.
A template of the framework used can be viewed in Figure 2.
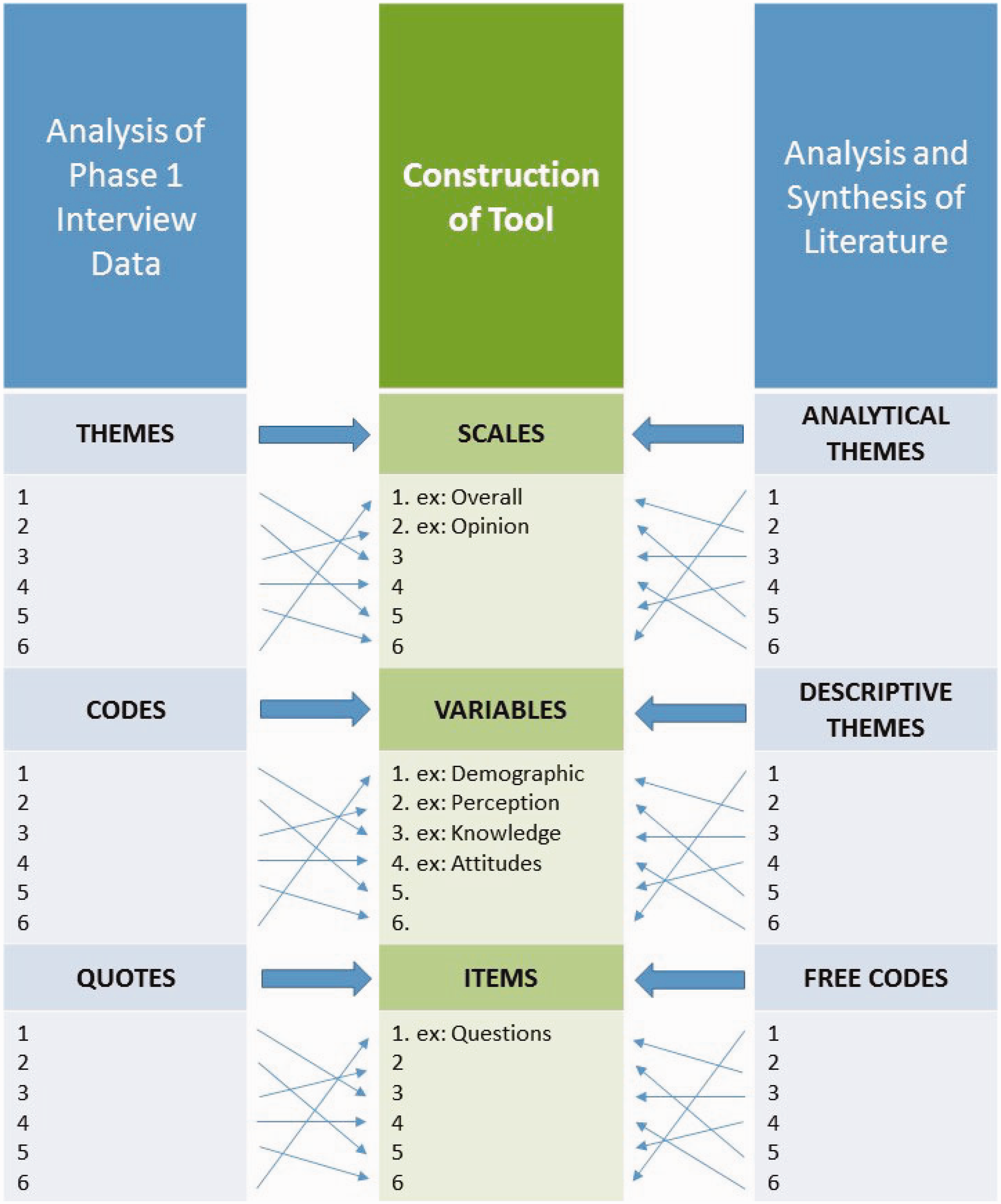
Framework used to facilitate conversion of qualitative data into a quantitative tool.
The framework was constructed based on guidance offered separately by Braun and Clarke,16 Thomas and Harden,17 DeVellis,18 Creswell,3 and Tay and Jebb.19 In his guidance on tool construction, Creswell3 described the process of translating qualitative results into a quantitative instrument. To this extent, he referred to qualitative results which have already been analyzed thematically into quotes, codes, and themes. At this stage, he recommended the conversion of quotes into the new instrument’s items, the codes into variables, and the themes into scales. This guidance was followed during the construction of the instrument in the current study. However, rather than using the interview results only in the construction of the tool, it was decided to also include certain aspects from the existing body of the literature on the subject. The reason behind using both of these sources was to construct a tool that has local relevance but which is also informed by the existing evidence base on the topic. The construction process of the framework is described below.
Analysis of phase 1 interview data (Figure 2 column 1)
As described earlier, the thematic analysis of the data that emerged from the interviews was carried out as guided by Braun and Clarke.16 In particular, this involved a process during which selected quotes led to the extraction of codes which were then grouped into overarching themes.
Analysis and synthesis of the literature (Figure 2 column 3)
Literature search
Data sources
An extensive electronic search was performed using ‘StarPlus – Library Catalogue’ and the Ovid MEDLINE database without language restrictions for studies published in the past 10 years. To enhance the sensitivity of the search, free text and subject headings (MeSH and EMTREE) were utilised. Four main keywords were derived from the aims of this research: ‘stroke knowledge’, ‘stroke recognition’, ‘stroke education’, and ‘stroke preparedness’. Exploded headings relating to these keywords were combined with the Boolean operators ‘OR’ and ‘AND’ for use in the searches. Synonyms and wildcards were utilised to expand the search and increase its sensitivity. In order to validate the search strategy, manual searching was next performed through the two journals that contributed the largest number of papers to this review, Stroke: A Journal of Cerebral Circulation and the International Journal of Stroke from 2007 to 2017. Reference lists of included studies were also checked to further validate the search.
Selection criteria
In order to minimise bias and to strategically select those studies which could best contribute to the informational needs of this review, stringent inclusion and exclusion criteria were applied. The latter were developed beforehand. Potential studies for inclusion were further assessed by a validated quality assessment tool, the RTI item bank,20 to enhance consistency and uniformity in the appraisal. Peer-reviewed quantitative and qualitative studies in any language with living human participants were included while animal and in vitro studies were excluded.
Data extraction
Titles and abstracts of retrieved studies were initially screened to identify eligible studies for inclusion. Full-text articles were then obtained for these studies as well as in cases where the primary evaluation was not sufficient to determine whether a study should be included or not. Any inclusion and exclusion decisions during this stage were documented and used to complete a Preferred Reporting Items for Systematic Review and Metaanalysis (PRISMA) flowchart.21 Articles that were not in the English language were translated. Reference management software (EndNote X7) was used to organise the articles retrieved and to exclude duplicate publications. Eligible papers were then grouped according to their main focus, which guided the development of chapters and sub-chapters within this literature review.
Analysis and synthesis of the literature for tool construction
In an article by Thomas and Harden,17 the authors presented a process of thematic analysis as applied to a body of literature rather than to raw qualitative data as per the norm. The rationale for this application was to explore and promote the use of a more structured and rigorous process when attempting to integrate the results of qualitative studies in systematic reviews. The authors exhibited the use of such an approach, which they termed
Construction of the tool (Figure 2 column 2)
The outcome of the parallel analysis of the interview data and the literature was next used to inform the construction of the tool (Figure 3).
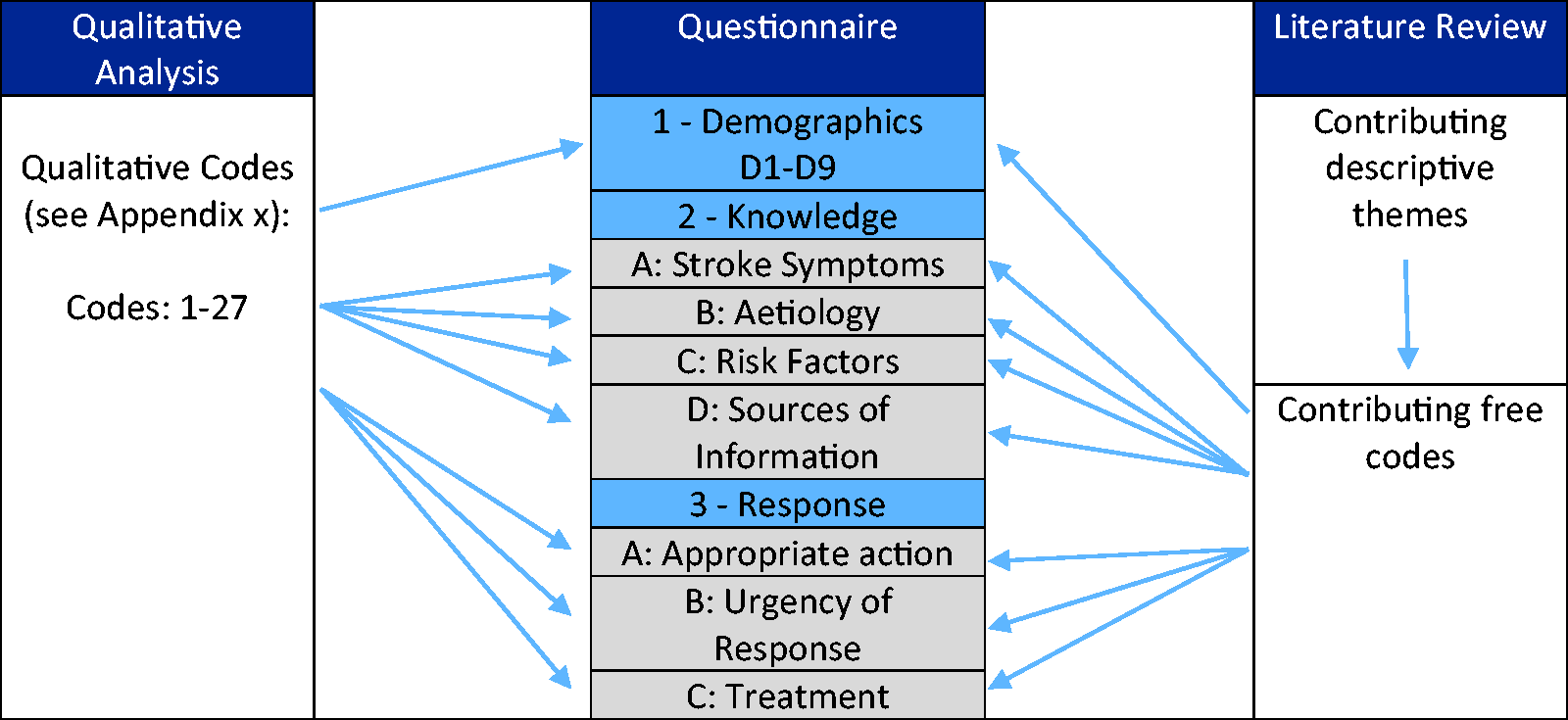
Framework used in study.
Thus, quotes (column 1) and free codes (column 3) became items within the tool (column 2). Similarly, codes (column 1) and descriptive themes (column 3) were translated into variables (column 2). Finally, themes (column 1) and analytical themes (column 3) were used to form scales (column 2). This part of the process of the construction of the tool was informed by Creswell.3 Moreover, guidance provided by DeVellis18 and Tay and Jebb19 on the different approaches to scale creation, principles of item creation, and psychometric properties was followed. Figure 4 demonstrates how the framework guided the development of the ‘Knowledge’ section of the questionnaire. The framework was similarly utilized for the construction of the ‘Response’ section. In addition to items assessing stroke knowledge, a section aimed at eliciting the participants’ demographic profile was included at the beginning of the tool and addressed the gender, age, educational level, and occupation (if any) of the participants.
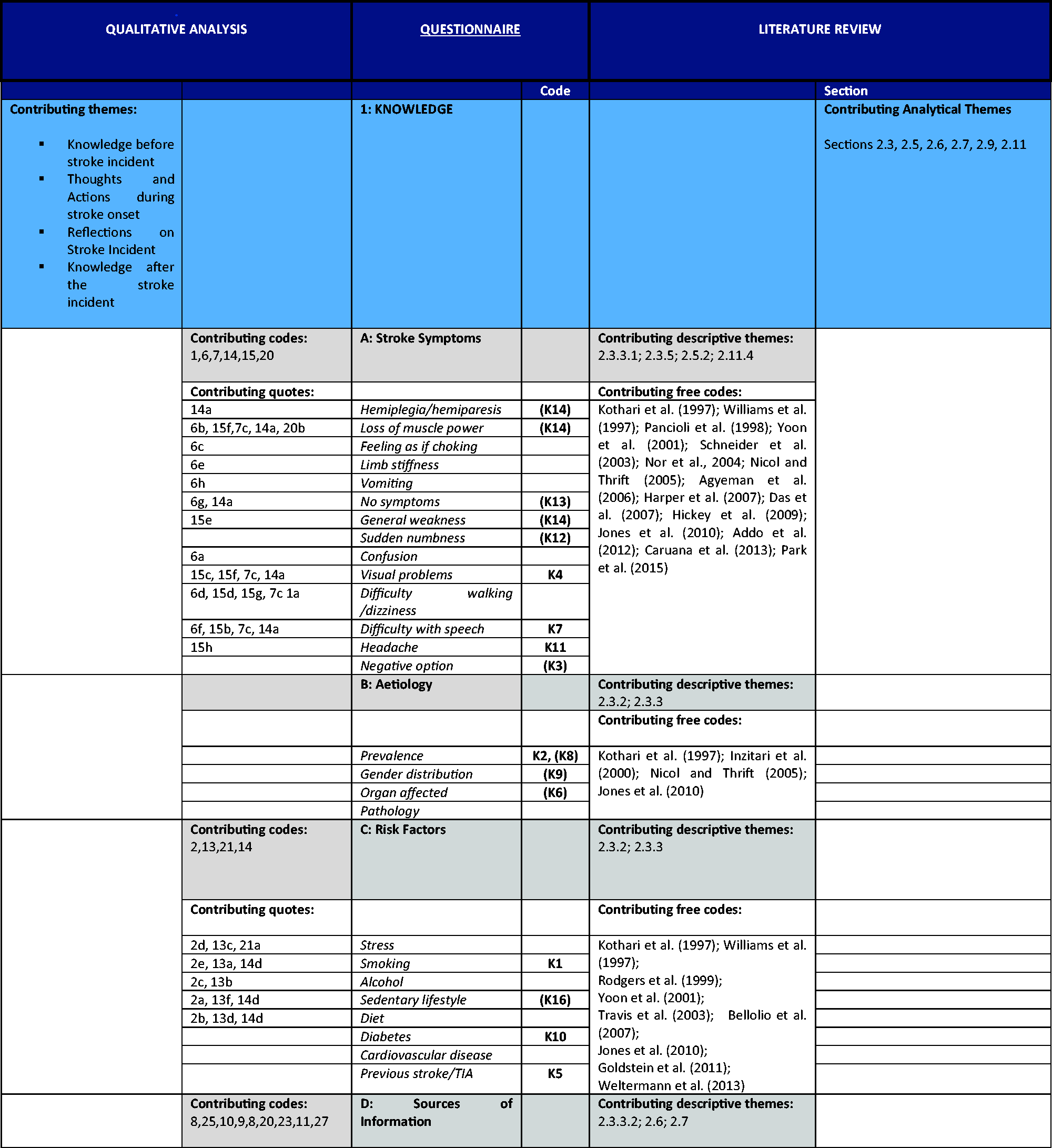
Matrix—knowledge section.
Following its construction, the tool was subjected to a number of tests in order to assure its quality. This was primarily done using a critical appraisal framework developed by Hou, Hoffmann22 in their endeavor to assess the quality of stroke knowledge assessment tools included in their systematic review. The authors developed this framework by consulting with professionals and by synthesizing three already-established criteria and checklists. The resulting appraisal framework consisted of three sections:1 conceptual framework,2 psychometric properties (e.g. validity and reliability), and3 feasibility.22
Stage 3 of the study
The final part of the study consisted of quantitative data collection. The main purpose of this phase was to explore the Maltese population’s knowledge in relation to stroke recognition and management.
In mixed methods research, it is common practice to include the same participants from the first stage of the study during the subsequent stages. However, this does not necessarily apply to exploratory designs since the recruitment of different participants may enhance and broaden the exploratory process as well as allowing generalizability.1 Therefore, in the current study, the participants in the quantitative phase were not the same as those in the qualitative phase. The decision to use the general public as one group of the target population in Stage 3 was based on the aim of the study, which was to explore stroke knowledge and education needs in Malta. Since stroke onset does not discriminate with regards to location, person, and time, it is highly likely that when a stroke occurs, the person is alone or with others in a non-healthcare setting and so symptom management depends on his or her knowledge and that of those around him or her. Nevertheless, and particularly if the symptoms are not overly alarming, the next step is typically to contact a GP or relative/friend who is also a healthcare professional. It is therefore also important to explore the stroke knowledge and educational needs of healthcare professionals as they can find themselves in the position to provide good advice and to refer the person to emergency services in a timely manner. This background information led to the decision to recruit healthcare professionals as the second participant group in the third stage of the study.
A total number of 1872 responses were collected. The Maltese population was taken to be 450,000 and the following mathematical calculation was used to determine the confidence interval of this sample size:
Margin of error
For a 95% confidence level,
The proportion p is unknown, however
When the sample size is


A sample size of 1872 participants selected from the entire Maltese population guarantees a maximum margin of error of 2.26%, assuming a 95% degree of confidence.
A stratified probability sampling technique was employed to allow for adequate representation of sub-groups (strata) within the whole population,23 as listed in the general electoral register.
Eligible individuals were contacted by email to invite them to participate in the study. The email contained information about the study as well as a link to the online survey. In a similar manner to the Stage 1 interviews, each potential participant was informed of his or her right to refuse participation and to withdraw from the study at any point. Moreover, reassurances regarding confidentiality, anonymity, and other ethical issues were provided. The consent form was not attached to the email but placed on the first page of the online survey so that unless the respondent completed this page, he or she would not be able to access the survey. The potential participants were given a deadline for survey completion and informed that a reminder email would be sent in 2 weeks’ time.
Following data collection, descriptive and inferential statistics were performed as part of the data analysis process.
Findings and discussion
A detailed account of the current study’s findings is beyond the scope of this article. Instead, only highlight findings will be discussed briefly in order to demonstrate how all the research questions were answered, particularly those that necessitated a mixed methods approach.
Stroke knowledge and response in Malta were found to be severely lacking and to reflect what has been reported in the literature. Several variables were found to affect this knowledge, including demographic factors as well as broader social and cultural influences. The interactions between these factors were deemed crucial to understanding the underlying problem and were explored with respect to Bronfenbrenner’s ecological framework as well as by adapting several health-promotion theories and models.
Action in stroke was found to be dependent on the degree of stroke knowledge. Spearman’s rho was calculated for the correlation between Knowledge and Response scores as the latter were both non-normalised data sets. The Spearman correlation coefficient was 0.753 showing a strong positive relationship between the two variables. Moreover, this relationship is significant since the p-value (approximately 0) was less than the 0.05 level of significance. Hence, we can generalise that participants who have a high knowledge score also tend to achieve a high response score. This direct correlation persists even when one considers potential social and cultural barriers to action.
From the study findings, it also emerged that new approaches to public education regarding stroke are needed and may include:
culturally appropriate descriptions of stroke symptoms. educational campaigns targeted at broader audiences other than patients at risk. an emphasis on the fact that effective treatment now exists and may improve clinical outcomes. an emphasis on the fact that stroke symptoms (no matter how trivial) merit immediate medical attention. patients at risk or who have already suffered a stroke need support to modify potential risk factors and reduce the chances of a future event.
The study also highlighted the fact that stroke treatment and practice guidelines are continuously evolving and improving and hence medical doctors and healthcare workers need to keep abreast of such advances.
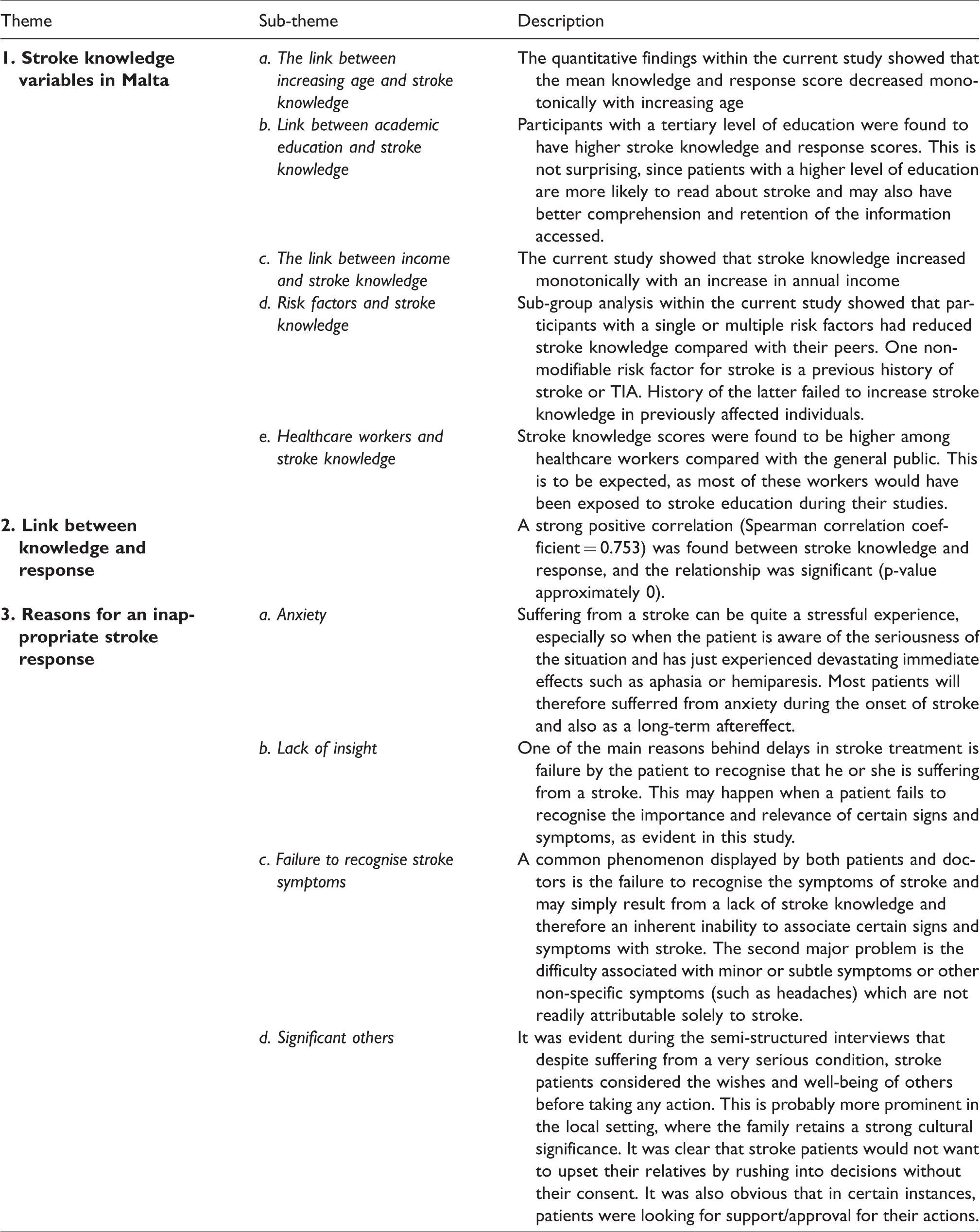
The above points not only summarize the research undertaken but also require consideration if further studies related to the subject or a national strategy on stroke should be implemented in practice. Table 1 depicts the main findings (themes and sub-themes) that emerged from the cross-synthesis process of the quantitative and qualitative findings.
Themes and sub-themes that emerged from the cross-synthesis process.
Strengths and limitations
The semi-structured interviews were performed by a person who worked in a healthcare setting. This may have unintentionally led to a degree of interviewer bias. The use of a semi-structured design with a standard group of questions may have limited such bias as the interviewer attempted to adhere to the pre-set questions.
Additionally, interviewees may have been influenced by bias introduced with hospital stay. An example of this would be consent bias, particularly since those who had received acute stroke treatment, may have felt obliged to participate in the study. This could have been further aggravated by power issues in the patient–doctor relationship. Thus, potential participants were approached by a third party in order to reduce this phenomenon.
The questionnaire was delivered via Google Forms and invitations to participate were sent via email, meaning that only people who were computer literate and had internet access received the invitation to participate. This resulted in selection bias during the quantitative phase of the study.
The main strength of this study lies in the meticulous use of a mixed methods paradigm which ultimately led to a comprehensive and reliable picture of the current situation in Malta. Throughout the study, several measures were taken in an attempt to enhance the trustworthiness of the study, in particular ensuring a transparent research trail during the construction of the matrix.
Conclusion
Mixed methods research is nowadays well established and may become handy in certain situations, particularly when the research questions posed cannot be answered by a traditional mono-method investigation. Although, mixed methods may be laborious and demanding in terms of acquaintance with quantitative and qualitative methods, the researcher cannot compromise on any of these research methods. Instead he needs to be pragmatic both in the quantitative and qualitative components of the study. One cannot overstress the importance of integrating the two components however as this is what ultimately comprises mixed methods. This integration needs to be planned as from the initial phase of any study and should follow specific guides to ensure its efficacy. In the current study, the authors describe the development and implementation of a framework (matrix) through which a quantitative tool was constructed in stage 2 by ‘building’ on qualitative data which emerged from stage 1 of the study (10 interviews with stroke patients and bystanders). The authors also describe the use of ‘thematic synthesis’ to inform the tool from the relevant literature which further enhances the comprehensiveness of the tool. The latter was then used to collect quantitative data from a large sample of the population (in stage 3) in order to enhance generalizability of the results.
Hence the described framework ensured and facilitated data integration throughout this study, and may serve as a template for future mixed methods studies, particularly those following an exploratory sequential design.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.