
Abstract
Optimism and pessimism are psychological constructs that reflect individuals’ generalized expectations for future outcomes, often manifesting as positive or negative anticipations of outcomes across diverse life scenarios. The study of optimism and pessimism among veterans is particularly pressing due to the distinctive challenges and experiences they face both during and after military service. Using a sample of veterans in the United States (n = 1,495), this study examined predictors of loneliness among veterans, focusing on the role of life outlook (optimism versus pessimism) on their post-military well-being. Overall, results from multiple regression analyses showed that respondents who displayed higher levels of optimism exhibited lower levels of loneliness (B = −0.017, p < 0.001), whereas higher levels of pessimism were associated with higher levels of loneliness (B = 0.021, p < 0.001). Furthermore, respondents who placed a high value on serving others and experienced higher levels of guilt reported higher levels of loneliness. Additionally, respondents’ levels of pessimism were linked to how their guilt levels influenced their levels of loneliness, underscoring the complexity of these relationships in shaping loneliness. In the realm of mental health, respondents who reported negative emotions, substance misuse, and suicidal thoughts experienced higher levels of loneliness than those who did not, but these effect sizes were attenuated when accounting for their levels of optimism and pessimism, suggesting that optimism and pessimism cannot be understood as a simple construct along a single continuum. Furthermore, respondents’ levels of satisfaction with their living conditions were negatively linked to their levels of loneliness. When their sociodemographics were considered, Black, Hispanic, and married respondents were less lonely than their White and unmarried counterparts, respectively. Understanding the risk and protective factors shaping veterans’ health ecologies is critical to informing effective health promotion initiatives and improving practice outcomes.
Introduction
Optimism and pessimism are psychological constructs that reflect individuals’ generalized expectations for their future, often manifesting as the anticipation of positive or negative outcomes across diverse life scenarios. These outlooks are highly responsive to shifts in life events and circumstances (Chopik et al., 2020). In the health realm, optimism is associated with a range of favorable health outcomes, including more robust immune function, fewer and lower risks of chronic illnesses and cardiovascular diseases, less physical pain, and greater longevity (Boehm et al., 2020; Forte et al., 2022; L. O. Lee et al., 2019; Rasmussen et al., 2009). Empirical evidence suggests that patients with optimism report a greater likelihood of recovery from diseases, such as cancer, cardiovascular disease, diabetes, and obesity, in part because optimism seems to support behaviors and choices that, in turn, support good health (Forte et al., 2022; Robert et al., 2020; Zhao et al., 2019). In the realm of mental health, optimists report better mental health, greater life satisfaction, and reduced risks of mood disorders, anxiety disorders, and probable alcohol abuse (Öcal et al., 2022; Piper, 2022). It is, therefore, not surprising that those with higher levels of optimism tend to employ proactive coping skills and exhibit greater resilience to stress (Conversano et al., 2010; Mens et al., 2021). In contrast, pessimists are more likely to engage in unhealthy behaviors, such as smoking, using substances, and engaging in behaviors that exacerbate their health risks (Scheier & Carver, 2018).
Using a sample of veterans in the United States (n = 1,495), this study examined predictors of loneliness among veterans, focusing on the role life outlook (optimism versus pessimism) played in their post-military well-being. Although the study of optimism and pessimism has garnered increased empirical attention in diverse academic disciplines such as psychology and health research, their complex and multifaceted nature presents significant challenges to researchers and practitioners seeking to understand and accurately define them (Carver & Scheier, 2019; Millstein et al., 2019). The study of optimism and pessimism among veterans is particularly pressing due to the distinctive challenges and experiences they face both during and after military service. Veterans may experience a range of emotions ranging from pride to guilt and self-stigma (Blais & Renshaw, 2014; Bryan et al., 2015; McCormick et al., 2019). The ethical conflicts soldiers face, especially in combat scenarios, can generate moral trauma, manifesting guilt, anger, and betrayal (Molendijk et al., 2022). In addition to confronting combat exposure, deployment stress, and challenges of reintegration into civilian life, post-military service members encounter a multitude of roadblocks that can profoundly influence their mental health resilience and future aspirations (Parker et al., 2019; RAND, n.d.; U.S. Department of Veterans Affairs, 2022). These factors, when combined, can exacerbate feelings of disconnection, isolation, and loneliness (G. Wilson et al., 2018). Understanding the risk and protective factors that shape veterans’ health ecologies has the potential to inform effective health promotion initiatives, enhance their overall well-being, reduce the nation’s healthcare expenditure, and mitigate the societal impacts of employment loss among veterans.
Military Context
The United States has one of the world’s largest active military forces, with nearly 1.3 million active military personnel (U.S. Department of Defense, 2022). Service members are governed by the Uniformed Code of Military Justice, which includes character requirements that hold different standards from civilians, and any violation of these standards can lead to removal from the military (Harding, 2016; U.S. Department of Defense, n.d.). Furthermore, service members learn about military culture through basic training or boot camp, which helps them assimilate into the military culture (Redmond et al., 2015). The social organization in the military is hierarchical and determined by military rank, yet the military is often regarded by its members as a second family. Military communication, which is more direct, authoritative, and hierarchical, requires service members to follow instructions and commands from their supervisors (Hall, 2011). In addition to focusing on collective needs over individual needs (Weiss et al., 2011), active combat service members must remain present-oriented and mission-focused while simultaneously preparing for potential disasters (Harding, 2016).
Veterans are individuals who have previously served on active duty in at least one branch of the military, including the Army, Air Force, Navy, Coast Guard, and Marine Corps, in different periods ranging from the World War II, the Korean War, the Vietnam War, the Global War on Terrorism, the Operation Iraqi Freedom, and the Operation Enduring Freedom in Afghanistan (Holder, 2016). Veterans currently represent 6% of the U.S. population, totaling approximately 18 million individuals (Schaeffer, 2023). Many veterans face impediments to reintegration, including struggles with interpersonal difficulties, personal growth, and juggling the disparities between civilian and military life after leaving the U.S. Armed Forces (McCormick et al., 2019). Veterans’ reactions to their military experience vary greatly; however, they range from upholding military culture closely to distancing themselves and, in some cases, developing distrust toward the government due to perceived betrayals by bureaucracy, leadership, or their superiors, as well as presumed transgressions of core values (Coll et al., 2011; McCormick et al., 2019).
Veteran Identity and Values
Military culture guides conduct in the military (McCormick et al., 2019) and binds service members through values such as loyalty, unity, and cohesiveness in order to enhance survival in armed conflicts (Farnsworth et al., 2014). Integral to this culture are patriotism and nationalistic pride (McCormick et al., 2019), which have been linked to boosting self-esteem and improving social status (Moldjord et al., 2021), as enlistment allows service members to serve a cause greater than themselves (McCormick et al., 2019). Notwithstanding, military personnel often face considerable challenges reintegrating into civilian life upon leaving the military and navigating cultural differences that affect their sense of identity. Stigma, for instance, can significantly impact veterans’ well-being and successful reintegration. In addition to having to confront public stigma (e.g., stereotypes, hostility, or discrimination against veterans) (Blais & Renshaw, 2014), veterans may internalize these stigmas, feeling ashamed or embarrassed about their struggles. Veterans may also experience moral injury when they perceive their ethical beliefs have been violated—whether through actions they committed, failed to prevent, or witnessed (e.g., atrocities)—and may feel betrayed by legitimate authorities in high-stakes situations (Jinkerson & Battles, 2019; Shay, 2014). Moral injury can lead to guilt, self-blame, distress, and post-traumatic stress disorder (PTSD) and is a risk factor for suicidal ideation and suicide attempts (Bryan et al., 2015). Some veterans have disclosed feeling ambivalent about help-seeking and prefer not to reveal their military experience with someone outside of the U.S. Armed Forces because they believe others cannot understand the differences between military and civilian life (McCormick et al., 2019).
Mental Health
The mental health of veterans is a critical concern in the United States, underscored by higher rates of depression, PTSD, and suicide compared to civilians (Ramchand, 2022; U.S. Department of Veterans Affairs, 2022; Wells et al., 2010). Combat duty can result in profound social isolation and loneliness for returning veterans, sometimes exacerbated by a number of other challenges, including physical injuries, exposure to traumatic events, psychological trauma, substance misuse, and marital adjustment (Brunet et al., 2015; Morin, 2011; G. Wilson et al., 2018). Negative emotions can increase the propensity for substance use disorders (Stellern et al., 2023). Veterans’ higher rates of tobacco, alcohol, and prescription pain reliever use compared to non-veterans can have profound effects on their daily functioning and overall well-being (Agaku et al., 2020). According to the most recent National Veteran Suicide Prevention Annual Report, the average number of veterans committing suicide per day in 2020 was 16.8 (U.S. Department of Veterans Affairs, 2022). Loneliness and social isolation can further erode mental health, leading to depression, suicidal ideation, and, at times, suicide (G. Wilson et al., 2018). By contrast, factors that have been noted to contribute to promoting psychological resilience in trauma-exposed veterans include partaking in prosocial behaviors and having a strong sense of life purpose, emotional stability, and gratitude (Fogle et al., 2020). Veterans’ capacity to manage life stressors, higher psychological resilience, and access to social support also contribute to increased well-being as they transition to civilian roles (Vogt et al., 2021).
Perceived Quality of Life
Many veterans face health-related challenges, service-related injuries, and chronic health conditions that impact their quality of life. Military service members often face unique physical challenges that stem from the rigorous demands of military service, including lower extremity and low back injuries. High-impact activities, heavy gear, and prolonged periods of standing or marching can contribute to chronic knee, hip, and ankle issues, leading to pain, instability, and even long-term mobility limitations (Cameron et al., 2016; Molloy et al., 2020). Additionally, the repetitive strain on the lower back from carrying equipment or enduring extended deployments in challenging environments can lead to significant lower back pain, muscular imbalances, and spinal conditions (Mattila et al., 2017; Molloy et al., 2020). These injuries not only impact physical health but can also affect their post-service daily functioning, mental well-being, and overall quality of life. Mobility is critical for supporting veterans’ independence, social engagement, and access to care. Physical mobility, for example, may positively shape one’s outlook on life as one experiences greater independence, opportunities, and interactions with others. In contrast, restrictions in mobility can lead to social isolation and hopelessness. Reliable transportation facilitates access to healthcare, employment, and social interactions, reducing isolation and supporting a more active, engaged lifestyle, thereby improving quality of life (R. J. Lee & Sener, 2016). Satisfaction with life, which is linked to a sense of well-being, plays a crucial role in shaping one’s outlook and can be a protective factor in stressful life events (Padmanabhanunni et al., 2023). Chang et al. (2020) found that low environmental quality negatively impacted all aspects of quality of life via the mediating effects of increased stress and poor sleep.
Hypotheses
Several hypotheses were formulated to investigate factors associated with the extent of loneliness among veterans in the United States. First, we hypothesized that respondents with higher levels of optimism would exhibit lower levels of loneliness (H1) in contrast to those with higher levels of pessimism (H2). Next, respondents’ sense of pride about having served in the U.S. Armed Forces was hypothesized to be positively related to their well-being, leading to reduced levels of loneliness (H3). Furthermore, respondents who embraced service as a fundamental aspect of their life purpose would be more inclined to report lower levels of loneliness (H4). Next, respondents who harbored guilt about their military service/experience would exhibit heightened levels of loneliness (H5). When mental health was taken into consideration, respondents reporting negative emotions more frequently would be prone to displaying higher levels of loneliness than their counterparts who did not (H6). Similarly, respondents who acknowledged substance misuse would report higher levels of loneliness than their counterparts who did not (H7). Hypothetically, respondents with suicidal thoughts would be lonelier in comparison to respondents without such thoughts (H8). When considering their perceived quality of life, respondents who were mobile (H9) and more satisfied with their living conditions (H10) would be less lonely than those who were not. Lastly, respondents’ sociodemographics (i.e., gender, age, race, marital status, and employment status) were modeled as control variables. Controlling for these variables allowed us to isolate the effect of the respondents’ outlook on life, identity and values, mental health, and perceived quality of life in shaping their feelings of loneliness. It also allowed us to provide a more nuanced understanding of potential variations across different sociodemographic groups, offering deeper insight into how these factors affect loneliness. We also explored the potential moderating effects of optimism and pessimism on respondents’ loneliness.
Method
Data
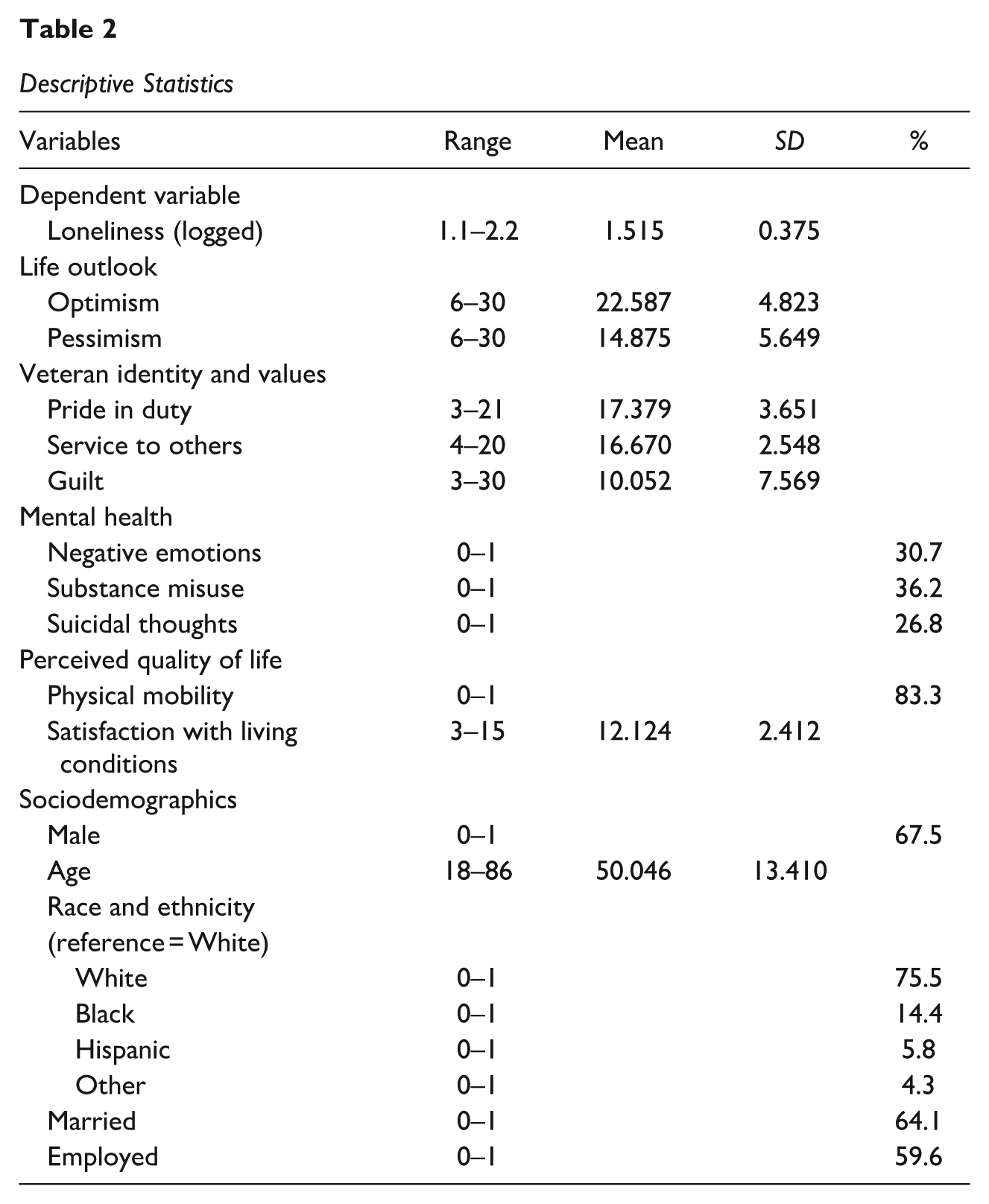
Data from this study came from the Military Health and Well-Being Project, which can be accessed from the Inter-University Consortium for Political and Social Research housed within the Institute for Social Research at the University of Michigan. Data were collected through an online survey administered via Qualtrics Panels. Respondents were a pre-selected group of individuals who had voluntarily opted in to be contacted by a market research service for survey participation (Qualtrics, n.d.). To be eligible for participation in the survey, respondents in this study had to be at least 18 years old, U.S. veterans of the post-Vietnam War era, and residing in the United States at the time of the data collection. Potential respondents received an email invitation from Qualtrics outlining the study’s purpose and procedures and providing a hyperlink to access the survey. The data collection, supported by the North Carolina State University’s 2019 Non-Laboratory Research Scholarship Program, commenced in May 2020 and lasted approximately a month. The researchers used stratified sampling to achieve a sample comprising nearly 15% of Black veterans and one-third of female veterans. Of the 1,863 responses collected, 1,495 responses met the inclusion criteria and were considered valid (i.e., survey completion time fell within three standard deviations of the mean) and were therefore included in this study (Desmarais & Cacace, 2020). The mean age of the respondents was 50 years old. Approximately 67.5% identified as male, 75.5% identified as White, 14.4% as Black, 5.8% as Hispanic, and 4.3% identified as belonging to other racial groups. Additionally, 64.1% were married, and 59.6% were employed. The secondary data analyses of this article received an exemption from the Institutional Review Board at The University of Texas at El Paso (ID#: 2216259). The dataset, developed to understand psychosocial factors associated with veterans’ health and wellness, was instrumental for this study as it contains measures related to military identity, health risks, and social integration. Thus far, no studies have examined the influence of veterans’ life outlooks in shaping their loneliness. Missing data for our selected variables in this study were estimated to be 0.24%.
Measures
Loneliness
Loneliness was measured using three items from the UCLA Loneliness Scale (Russell, 1996) that tapped into respondents’ sense of connection across various aspects of their lives (i.e., lack of companionship, feeling left out, and isolation). Using a 3-point Likert response scale (“Hardly ever,” “Some of the time,” and “Often”), items were coded where higher values indicate higher levels of loneliness. Factor analysis, using the principal components method and varimax rotation, revealed a one-factor solution with all items loaded onto a single factor with loadings of at least 0.87. Responses to each item were summed to create a composite loneliness scale, with lower scores indicating lower levels of loneliness. Log transformation was performed to reduce the skewness of the scale prior to running the regression analyses. Previous work has shown the items to be reliable and valid measures of loneliness (Alsubheen et al., 2023).
Life Outlook
Using a set of questionnaires completed by respondents and designed to assess their perceptions of wellness, factor analyses identified two distinct factors, with one measuring optimism and the other measuring pessimism, underlying respondents’ perceptions of overall wellness. The measure of respondents’ optimism was assessed by summing responses to the six items capturing their positive perceptions of life orientations (e.g., confidence in their abilities, focus on the bright side of things). Respondents’ pessimism was assessed by summing responses to the six items capturing negative self-view and perceptions of their future (i.e., felt inferior, hopeless, and rarely counted on good things happening to them).
Veteran Identity and Values
To assess respondents’ predisposition at the time of the data collection, we constructed three scales: (a) their pride in serving in the U.S. Armed Forces, comprising three items that assessed their patriotism, motivations for military service, and national identity, (b) their commitment to service as a core life principle, consisting of four items that measured their altruistic motivations, belief in humanity, and attitude about services, and (c) their guilt about their experience as military personnel, including three items that assessed their combat guilt, shame, and moral conflict. The selected items provided three cohesive measures of veteran identity and values, with three separate factor analyses revealing a distinct single-factor solution for each item set.
Mental Health
We selected six items from the original questionnaire to assess three mental health measures. One item measured the frequency of negative emotions (e.g., anxiety and depression). Four items assessed the history of substance misuse, and one item evaluated suicidal thoughts. All measures were coded as dichotomous variables.
Perceived Quality of Life
To assess their perceived quality of life, respondents were asked to rate their physical mobility (one item) and satisfaction with their living conditions (three items assessing living place, health services, and transportation). Physical mobility was coded as a dichotomous variable where those who were able to get around “well” or “very well” were coded 1, otherwise 0. Respondents’ satisfaction with their living environment was measured using a composite of three items assessing their subjective experiences and functioning over the prior two weeks. The three items were selected based on a factor analysis that revealed a single-factor solution, indicating a cohesive construct of satisfaction with the living environment. Both measures served as indicators of respondents’ overall well-being and quality of life, with the first capturing respondents’ ability to move freely to ensure their safety and the latter signifying their contentment with various aspects of their home environment and immediate surroundings.
Sociodemographics
Several sociodemographics of respondents were examined in this study. Respondents’ gender is a dichotomous variable where male respondents were coded 1, and female respondents were coded 0. Age is a continuous variable. Race/ethnicity is represented by four dummy variables (i.e., White, Black, Hispanic, and other racial classifications) with White as the reference category. With respect to their marital status, respondents who were married or in a domestic partnership were coded as 1, and those who identified as single, divorced, and widowed were coded as 0. To capture their employment status, respondents who worked for pay or profit the week before the data collection were coded as 1; otherwise, they were coded as 0.
The items comprising each scale used in the current study, along with the coefficient alpha for each scale, are presented in Table 1. Descriptive statistics for all study variables can be found in Table 2.
Description of Variables in Analyses

Descriptive Statistics
Analytical Approach
This study employed multiple regression analyses with Full Information Maximum Likelihood (FIML) as the estimation procedure. FIML, known to predict unbiased parameter values in the presence of missing data (Baker, 2019), is used to estimate the parameter values using all model information. Because the residuals from our initial regression model violated the assumption of normality, a log transformation of the outcome variable was performed before running the regression analyses to reduce skewness. An additional test was conducted to check for collinearity, but no concerns were identified. To understand how life outlook impacts veteran well-being, we examined the variables in three models. The veteran model (Model 1) integrated all variables pertinent to veterans’ experiences and sociodemographics. The optimism (Model 2) and the pessimism (Model 3) models incorporated the optimism and pessimism variables, respectively, in addition to all the variables in the veteran model. The setup of our models allowed us to examine the effect of optimism and pessimism above and beyond the effect of other variables on our outcome variable more confidently. To explore how veterans’ optimism or pessimism impacted the effects of their identity and values, mental health, or physical health on their levels of loneliness, we integrated eight interaction effects of these characteristics (i.e., identity and values, mental health, physical health) with their levels of optimism and pessimism in their subsequent models. To reduce the likelihood of making Type I errors (i.e., incorrectly rejecting a true null hypothesis), the Bonferroni correction was employed to yield a more conservative p-value, rather than the conventional p-value, in our analyses that included interaction terms. The Bonferroni-adjusted p-value is calculated by dividing the critical p-value by the number of tests performed.
Results
This study examined factors associated with loneliness in a sample of U.S. veterans. Overall, controlling for the effects of other variables in the model, respondents’ levels of optimism were negatively associated with their levels of loneliness (B = −0.017, p < 0.001 in Model 2). Their levels of pessimism, on the contrary, were positively linked to their levels of loneliness (B = 0.021, p < 0.001 in Model 3).
When considering their identity and values, we found that the respondents who placed a high value on serving others reported higher levels of loneliness across all three models with a statistical significance level of at least p < 0.05. Respondents’ levels of guilt were also positively linked to their levels of loneliness across all models (p < 0.001). However, the effect sizes of their levels of guilt decreased when pessimism was included in the model.
Next, we found that respondents who acknowledged experiencing negative emotions reported higher levels of loneliness (p < 0.001) than their counterparts who did not. In a similar fashion, respondents who disclosed substance misuse reported higher levels of loneliness than those without such experience (p < 0.01). This was also the case for respondents who had suicidal thoughts in comparison to their counterparts without such thoughts (p < 0.001). However, the effect sizes of their adverse mental health outcomes weakened when optimism or pessimism was included in the model.
When their perceived quality of life was considered, respondents with unimpeded mobility experienced less loneliness than those without (B = −0.050, p < 0.05), but this effect was only statistically significant in Model 1. The statistical significance of respondents’ mobility was rendered non-significant upon adding optimism or pessimism variable into the subsequent models. Respondents who experienced greater satisfaction with their living conditions experienced lower levels of loneliness (p < 0.001). Its statistical significance remained with and without the inclusion of optimism and pessimism into the model despite its reduced effect sizes in Models 2 and 3.
Respondents’ age was negatively related to their levels of loneliness in Model 2 (B = −0.002, p < 0.05). When race was considered, Black respondents reported lower levels of loneliness compared with the White respondents in Models 1 and 3 (B = −0.073, p < 0.01 in Model 1 and B = −0.052, p < 0.05 in Model 3). Similarly, Hispanic respondents also reported lower levels of loneliness than their White counterparts in these models (B = −0.069 in Model 1 and B = −0.072 in Model 3, p < 0.05). The marital status of the respondents appeared to exert a protective effect, with married respondents reporting lower levels of loneliness than their unmarried counterparts in all three models (p < 0.001). Table 3 shows the results from the multiple regression analyses.
Multiple Regression Analyses With Loneliness (logged) as the Dependent Variable
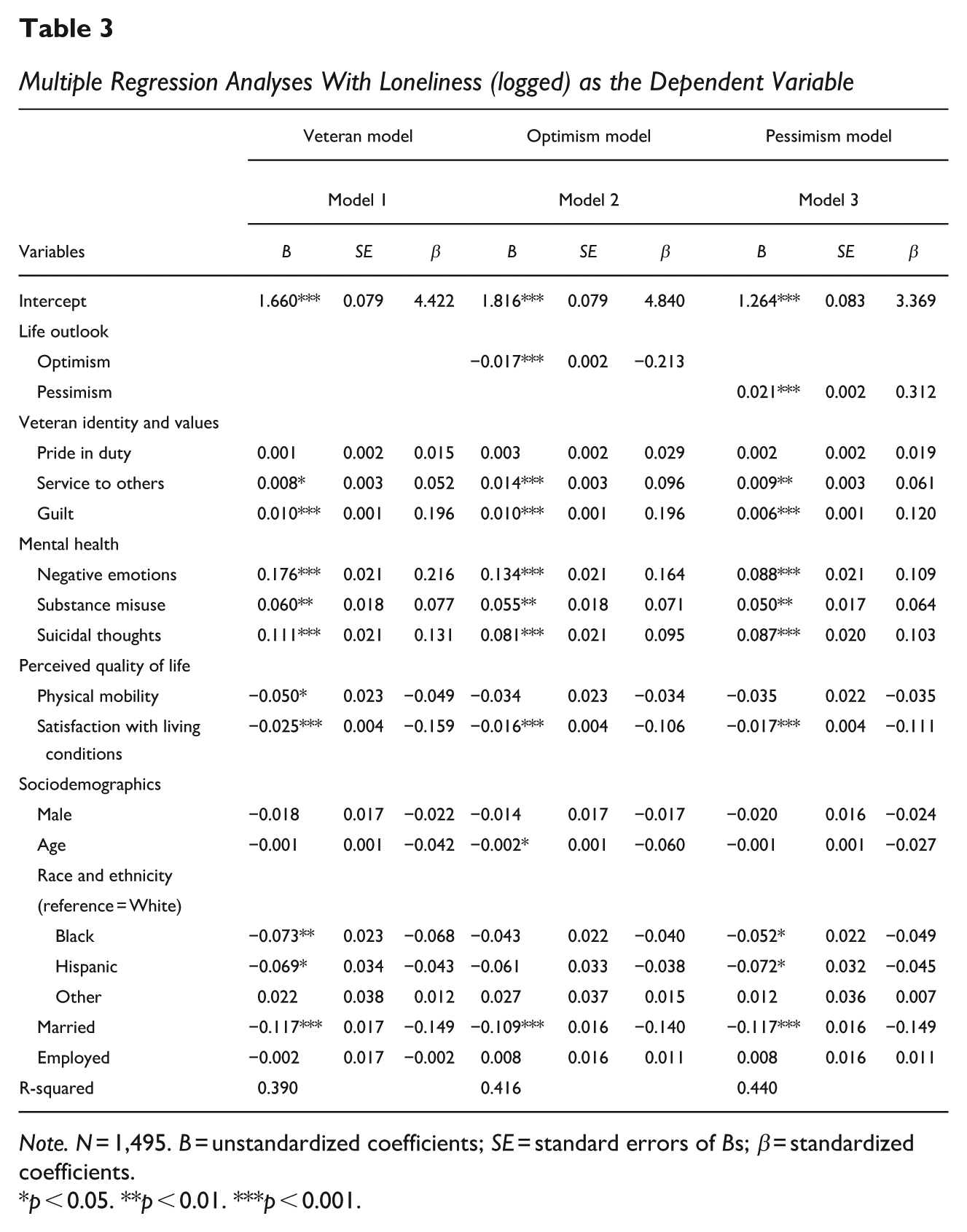
Note. N = 1,495. B = unstandardized coefficients; SE = standard errors of Bs; β = standardized coefficients.
p < 0.05. **p < 0.01. ***p < 0.001.
We presented the interaction effects in this study graphically (instead of in a new table), with only one effect showing statistical significance at the Bonferroni-adjusted p-value. Figure 1 illustrates that when guilt levels were low, respondents with high pessimism tended to report higher levels of loneliness compared to those with low pessimism. However, as guilt levels increased, those with low pessimism experienced higher levels of loneliness. This moderating effect implied that the protective effect of low pessimism in reducing loneliness might be contingent on respondents’ guilt levels. In other words, low pessimism could act as a buffer against loneliness for respondents with lower levels of guilt, but its benefit diminished as the guilt levels rose. This highlights that the relationship between veterans’ pessimism and guilt in shaping their loneliness is not always straightforward.
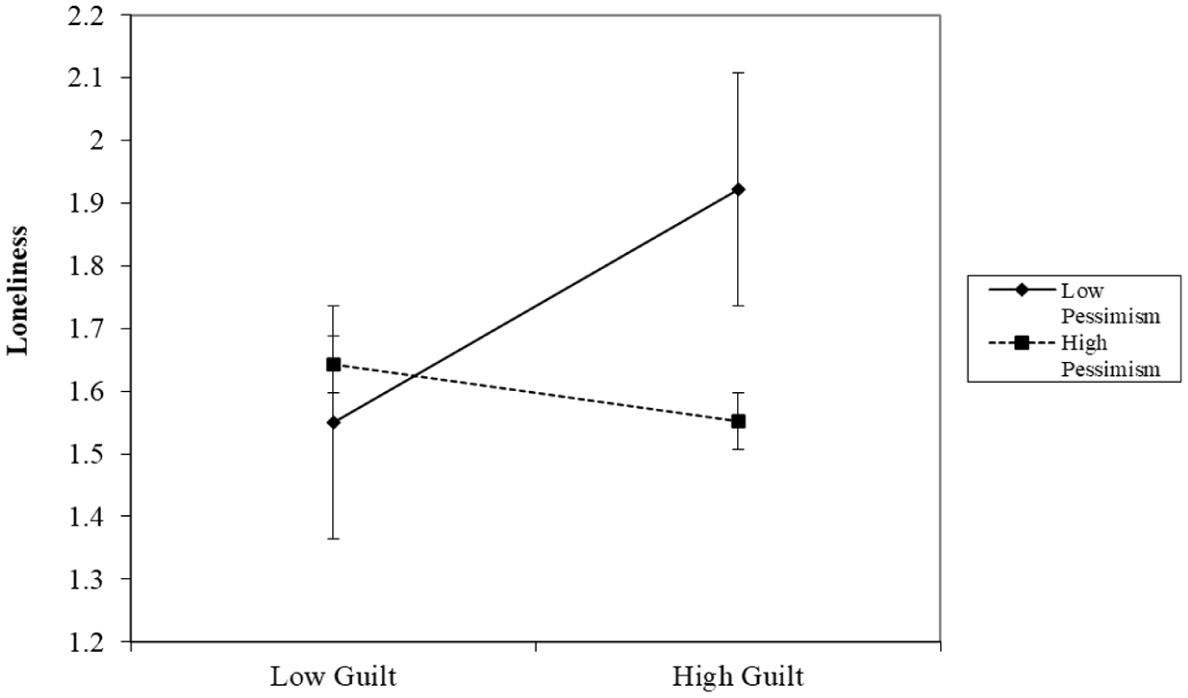
The Moderating Effect of Pessimism on the Relationship Between Guilt and Loneliness
Discussion
This study investigated factors influencing loneliness among veterans, emphasizing the roles of optimism and pessimism. In sum, we found that respondents who displayed higher levels of optimism exhibited lower levels of loneliness (H1), whereas higher levels of pessimism were associated with higher levels of loneliness (H2). Furthermore, respondents who placed a high value on serving others (H4) and experienced higher levels of guilt (H5) reported higher levels of loneliness. In the realm of mental health, respondents who reported negative emotions (H6), substance misuse (H7), and suicidal thoughts (H8) experienced higher levels of loneliness than those who did not, but these effect sizes were attenuated when accounting for their levels of optimism and pessimism, suggesting that optimism and pessimism cannot be understood as a simple construct along a single continuum. We also found that respondents’ mobility was negatively associated with their levels of loneliness (H9). However, this association lost statistical significance after accounting for their levels of optimism and pessimism. Additionally, respondents’ levels of satisfaction with their living conditions were negatively linked to their levels of loneliness, making loneliness less likely when life satisfaction was high (H10). When their sociodemographics were considered, Black, Hispanic, and married respondents were less lonely than their White and unmarried counterparts, respectively. Our interaction effect indicated that respondents’ levels of pessimism moderated the relationship between guilt and loneliness.
While studies in the past have noted that veterans’ pride in military service plays a crucial positive role in shaping veterans’ identity and self-esteem, fostering connections with their military past and contributing to a sense of accomplishment (Kleykamp et al., 2021; Moldjord et al., 2021), we did not find pride in military service to be significantly related to respondents’ experience with loneliness (H3). Conversely, our study found that respondents who placed value in serving others reported higher levels of loneliness (H4). It is well documented that veterans tend to be more civically engaged within their communities than non-veterans (S. E. Wilson & Ruger, 2021). We speculate that veterans’ sense of duty to help others might lead to feelings of isolation and loneliness when surrounded by those who do not share these values. We also suspect that respondents’ dedication and commitment to service beyond their military tenure might inflict emotional strain, particularly for those who struggled to reconcile their experience as military personnel when these expectations were unmet. As such, balancing the need to serve by adopting a positive outlook to find fulfillment may help veterans navigate post-service life more confidently and positively.
In addition, we found that respondents who reported high levels of guilt experienced higher levels of loneliness (H5). There is considerable evidence that exposure to potentially morally injurious events is linked to the development of varied psychiatric symptoms (of which guilt is one) among U.S. military personnel and veterans when they perceive themselves as having committed a moral violation (e.g., failing to prevent a death or killing someone in combat) or as victims of others’ transgressive acts (Griffin et al., 2019; Jinkerson & Battles, 2019; Shay, 2014). Nevertheless, it must be noted that many soldiers exposed to traumatic events during deployment report no severe psychiatric symptoms and are found to be resilient (Sinclair et al., 2013). Investigating the complex dynamics of how feelings of guilt influence the relationship between veterans’ life outlook and loneliness is imperative in future research endeavors, as our study showed that the nature of this relationship is not always clear-cut.
Our study underscores the role of mental health in mitigating the adverse impact of loneliness on combat veterans. Given the widespread prevalence of PTSD among veterans, Gettings et al. (2022) recommended addressing social isolation and loneliness in veterans with PTSD by empowering them to participate in their recovery through building trust, community, and purpose in the form of new skills that aid recovery. Empowering veterans to cultivate optimism may be fruitful in improving their mental health outcomes and strengthening resilience, as indicated by our study. Thomas et al. (2011) noted that dispositional optimism may not only optimize recovery from behavioral health concerns but also serve as a protective factor in mitigating the development of PTSD and the associated loneliness and social isolation that combat can generate.
Our study attests to the need to improve veterans’ living conditions (i.e., living environment, access to health services, and mode of transportation) as contentment with one’s living environment has the potential to provide a sense of comfort, maintain social relationships, and reduce loneliness. In the extant literature, the effect of race on loneliness is mixed (Schochet et al., 2023; Sol et al., 2023). In our study, Black and Hispanic respondents reported lower levels of loneliness compared with their White respondents, but only for two of the three models examined. The effect of race on veterans’ loneliness warrants further exploration. On the one hand, Blacks are susceptible to life events that may increase loneliness (e.g., poverty and structural disadvantages) (Taylor & Nguyen, 2020). On the other hand, Black community is known for its strong cultural resource systems of social support (Bryant et al., 2024). Research has shown that Blacks often benefit from the adaptive coping strategies and key resources (spirituality and interpersonal support) they develop to navigate and overcome life challenges (Brenner et al., 2018). Likewise, Gallegos and Segrin (2019) found that spirituality promotes better health for Latinos than non-Latino Whites by reducing loneliness. Our study also found that marital status is a protective factor in reducing loneliness, likely because marriage provides emotional support and companionship that can buffer against feelings of isolation. We encourage future researchers to explore potential contextual factors that may be correlated with other sociodemographic variables absent in this study, such as military rank, income, educational attainment, and community of residence. To yield valuable insights for prevention, examining optimism and pessimism as outcome variables and exploring the mechanism shaping these dispositions would be fruitful.
Implications for Practice
Our study highlights the potential benefits of promoting optimism and reducing pessimism among veterans, advocating for the development of targeted interventions that improve their mental health and foster resilience. We recommend practitioners and the public develop greater awareness and sensitivity to veterans’ intra- and interpersonal struggles, as veterans who experience conflict with their values and beliefs may be reluctant to seek help or perceive themselves as undeserving of support (McCormick et al., 2019). Additionally, others may choose not to seek treatment due to self-stigma of mental illness (Barr et al., 2022). Evidence shows that veterans often find greater understanding and acceptance from fellow veterans (Mittal et al., 2013). Their shared bond and background may offer a sense of solidarity and understanding, enabling them to relate to each other’s challenges, cultivate mutual support, and foster a sense of camaraderie, which is challenging to come by elsewhere. As such, addressing and preventing moral injury using theoretically sound, evidence-informed intervention can play a critical role in empowering veterans and fostering their psychological resilience (Phelps et al., 2024).
To provide veterans with accessible support and improve their mental health, we recommend the implementation of outreach programs encouraging help-seeking behavior, along with treatment that facilitates self-forgiveness to reduce suicide attempts (Bryan et al., 2015). Hobfoll et al. (2016) found that veterans receiving cognitive–behavioral therapy web-based intervention for PTSD and depression that allowed them to complete the treatment in the comfort of their home reported reduced PTSD and depression. Because many veterans with traumatic experiences are likely to seek help from both clergy and mental health professionals, Farnsworth et al. (2014) suggested mental healthcare professionals explore with their military and veteran clients how clients’ religion and spirituality influence the perception of morally injurious experiences and prepare to coordinate and collaborate with spiritual care providers such as chaplains and community-based clergy, if necessary, to improve their clients’ mental health outcome. It is important to note that veterans frequently experience health disparities in healthcare utilization, health outcomes, or access to care (Kondo et al., 2017). Improving access to a quality living environment by addressing housing conditions and neighborhood features and enhancing transportation infrastructure and healthcare services can facilitate veterans’ access to essential care, foster healthier living conditions, and improve their overall quality of life (R. J. Lee & Sener, 2016), which is critical to lowering their perceived loneliness, as shown by this study.
Study Limitations
Our study offers a range of insights about various factors influencing veterans’ experience with loneliness, but several limitations should be acknowledged. First, our study could not draw causal inferences and generalizability due to the cross-sectional design and nonprobability sampling method utilized in the data collection. As such, the sociodemographic breakdown of survey respondents in this study may not fully align with the breakdown of the veteran population in the United States. Furthermore, like any self-report study, our study suffers from recall bias, a systematic error that occurs in research studies when participants are not able to remember past events accurately and erroneously provide responses based on their ability to recall experience (Althubaiti, 2016). Additionally, our study might be susceptible to selection bias as respondents with more health issues and mental health challenges might be less inclined to participate in the study. Moreover, respondents who are lonely might be more likely to engage in substance use and report adverse mental health, which may perpetuate a cycle that intensifies these challenges. Therefore, this study’s findings should be interpreted in light of these limitations. It is critical to point out that some of the scales in this study (such as those that tapped into the respondents’ life outlook, veteran identity and values, and satisfaction with living conditions) have not been previously validated in other studies. Therefore, these scales should be regarded as provisional proxies, with further validation necessary to establish their reliability. Our study was also limited to the coding and types of sociodemographic variables available in the existing dataset. Because the data were collected during the COVID-19 pandemic, widespread social isolation due to the global lockdown and social distancing measures, along with other pandemic-related stressors such as economic hardship/uncertainties, fear of disease infection, and elevated mortality rate, might have heightened feelings of loneliness (Ernst et al., 2022; Hwang et al., 2020).
Conclusion
This study examined factors leading to veterans’ feelings of loneliness. Overall, we found that respondents with greater optimism tended to experience lower levels of loneliness, whereas those who were more pessimistic reported higher levels of loneliness. This effect persisted even after accounting for other individual and contextual factors relevant to U.S. veterans. Additional factors that could influence their experiences with loneliness included their values on service, feelings of guilt, mental health, mobility, satisfaction with their living conditions, and sociodemographic characteristics. We recommend that future researchers explore potential moderating effects between veterans’ life outlooks and values to gain insights into how these factors may jointly influence their experiences with loneliness.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.